0280
Accuracy of Measuring Opening and Closing Characteristics of the Aortic Valve with SPEEDI MRI1Center for Magnetic Resonance Research, University of Illinois at Chicago, Chicago, IL, United States, 2College of Medicine, University of Illinois at Chicago, Chicago, IL, United States, 3Departments of Radiology, Neurosurgery, and Biomedical Engineering, University of Illinois at Chicago, Chicago, IL, United States
Synopsis
Keywords: Valves, Valves, SPEEDI, sub-millisecond, high temporal resolution
Motivation: get-SPEEDI, a recently published pulse sequence, offers a promising MRI technique for imaging the rapid dynamics of the aortic valve (AV) opening and closing with sub-millisecond temporal resolution.
Goal(s): This study aims to assess the accuracy of measuring the AV dynamics with get-SPEEDI by comparing its performance with transthoracic ultrasound, which is the gold standard clinically.
Approach: Ultrasound echocardiograms and get-SPEEDI MR images of AV were acquired in healthy human subjects with 0.6- and 0.8-ms temporal resolution, respectively.
Results: There were no statistically significant differences between get-SPEEDI and ultrasound in the measurements of AV opening and closing dynamics and the maximum AV area.
Impact: The dynamic characteristics of the aortic valve measured with get-SPEEDI MRI agree well with the ultrasound measurements. get-SPEEDI MRI provides a new imaging tool for diagnosis of aortic valve diseases.
Introduction
Diagnosis of aortic stenosis, regurgitation and other pathologies relies on accurate measurement of the opening and closing characteristics of the aortic valve (AV).1-2 MRI is not used for imaging the dynamic process of the AV in clinical practice because it cannot satisfy the requirement for high temporal resolution (~ ms).2-4 Recently, SPEEDI pulse sequences have been developed for detecting cyclic events with sub-millisecond temporal resolution, offering a promising MRI technique for imaging the AV dynamics.5-6 This study aims to evaluate the accuracy of measuring the opening and closing characteristics of the AV with SPEEDI by comparing its performance with ultrasound, which is the gold standard clinically.Methods
MRI acquisition: Ten healthy human subjects (five males and five females; age: 22-32 years with mean = 25.4 years) were recruited under an IRB-approved protocol. Using a get-SPEEDI sequence,6 MR image time series of AV with 0.6-ms temporal resolution were acquired on a 3T GE MR750 scanner (General Electric Healthcare, Waukesha, WI) with a 32-channel cardiac phased-array coil. The imaging plane was chosen orthogonally to the aortic outflow tract for simultaneous en face visualization of all three aortic valve cusps. The imaging parameters were: FOV = 24 × 24 cm2, matrix size = 118 × 80, slice thickness = 8 mm, TR/TE = 20/8.8 ms, flip angle = 10°, two ECG trigger delays (12 and 22 ms) with 36 cardiac phases per delay, echo train length = 16, and echo spacing = 0.6 ms. The get-SPEEDI MRI scan spanned over 160 heart beats with about 10 breath-holds.Ultrasound acquisition: For comparison, transthoracic 2D echocardiography was carried out on an iE33 ultrasound unit (Philips Healthcare, Best, The Netherlands) for the 10 subjects. The aorta dynamics were recorded in the parasternal long-axis view with one image acquired every 15ms under B-mode. Using the B-mode image as a reference, 1D M-mode echocardiograms covering the orifice plane were collected to capture the dynamics of AV movement with a frame rate of 0.8 ms, which was comparable to get-SPEEDI temporal resolution.
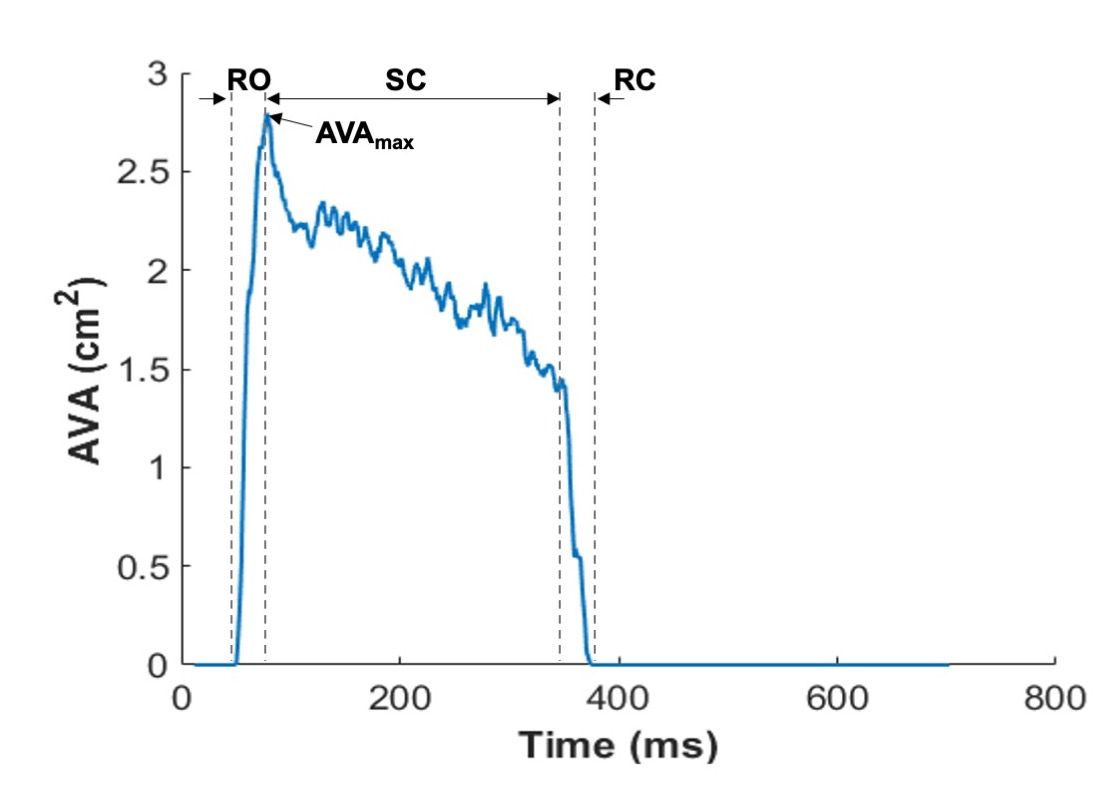
Data analysis: A total of 1152 time frames with 0.6-ms temporal resolution (= echo spacing) were obtained from the get-SPEEDI MRI scan. On each frame, the AV orifice was delineated by a semi-automated algorithm7 to derive the planimetric aortic valve area (AVA) and investigate its time evolution. From the time course of AVA, the durations of the three phases of the AV cycle3 – a rapid opening (RO), a slow closing (SC) and a rapid closing RC) – were measured, together with maximum AVA (AVAmax). The same parameters were also measured on the M-mode profiles of ultrasound data, followed by a statistical comparison between the SPEEDI and ultrasound measurements with a t-test.
Results
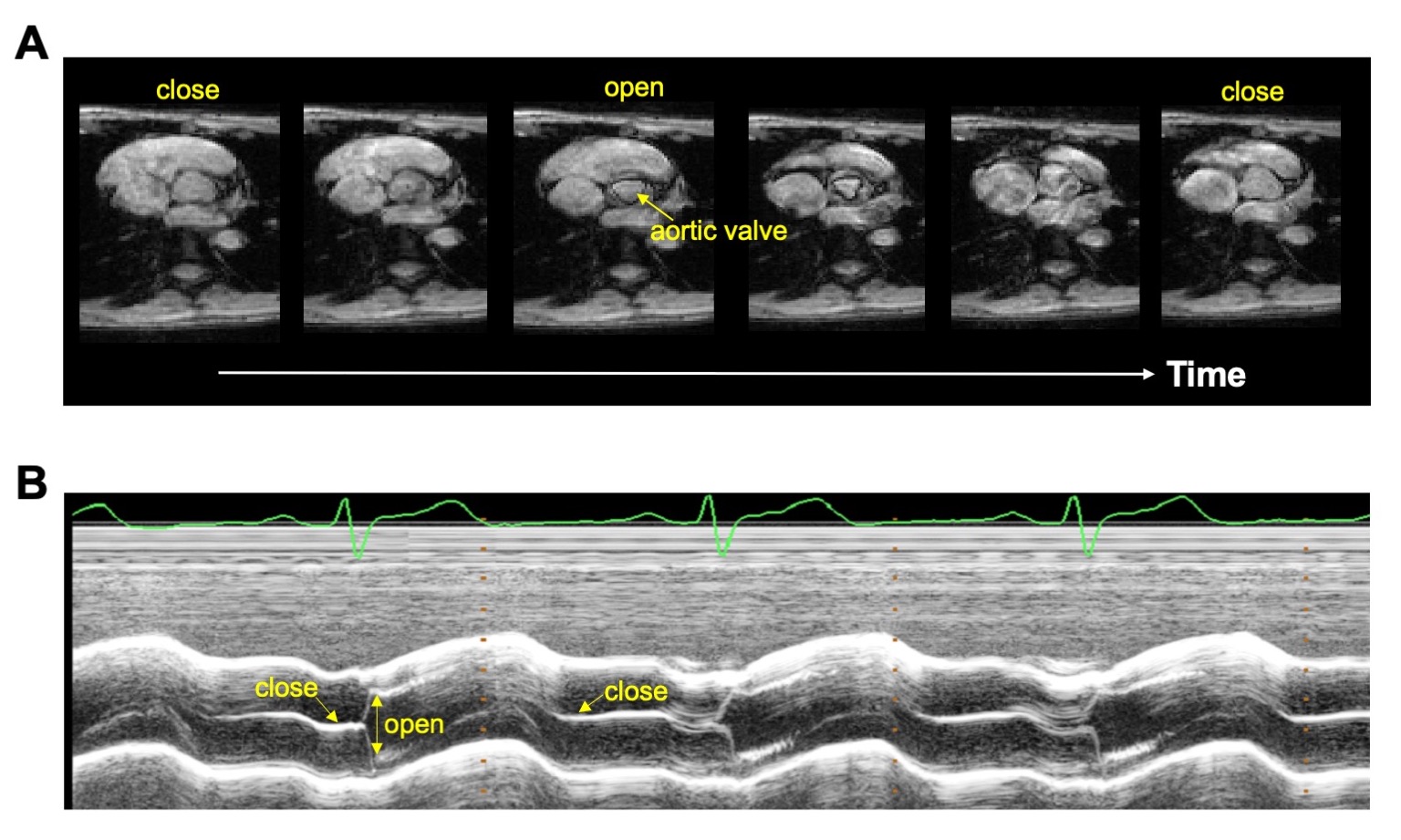
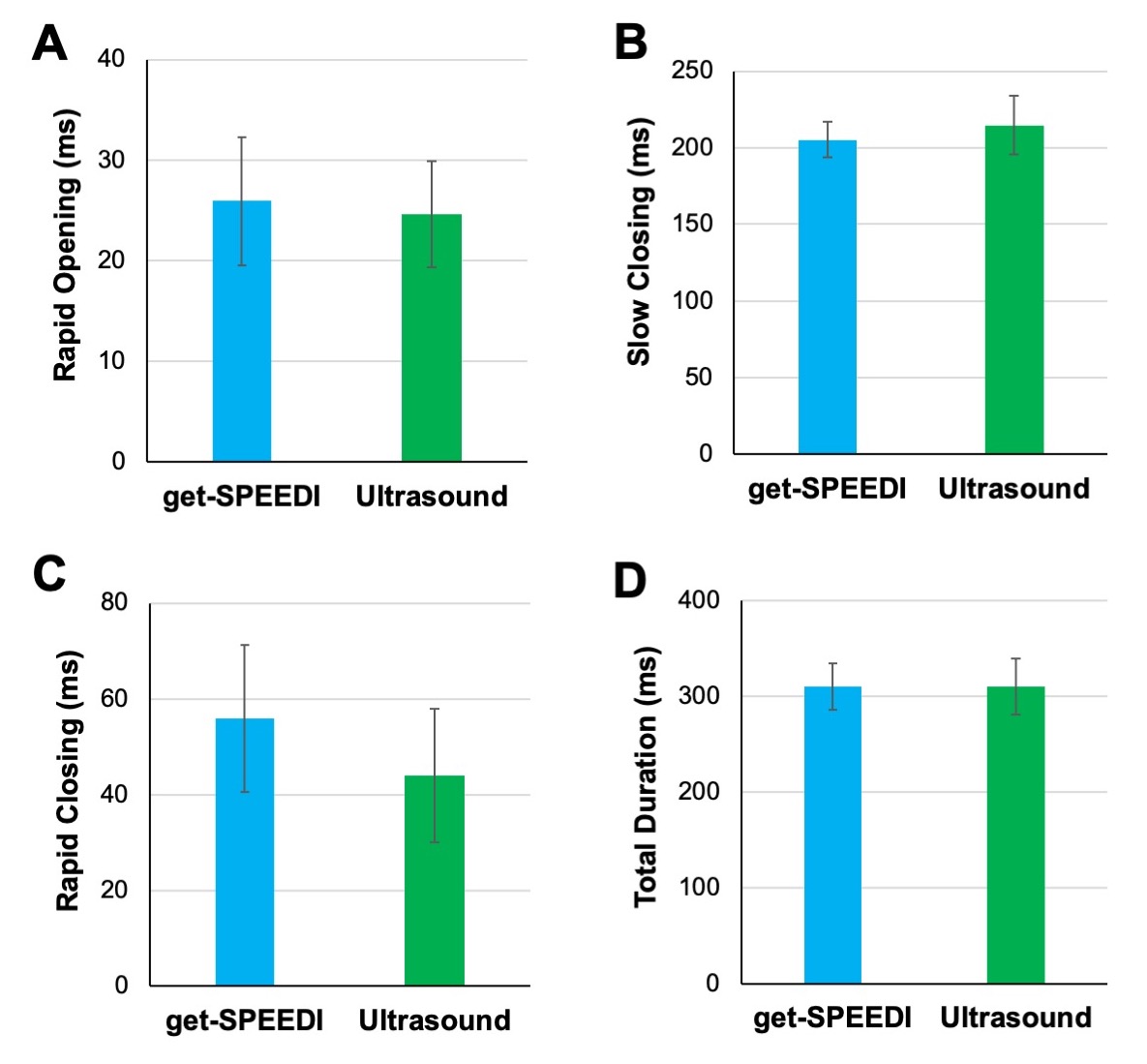
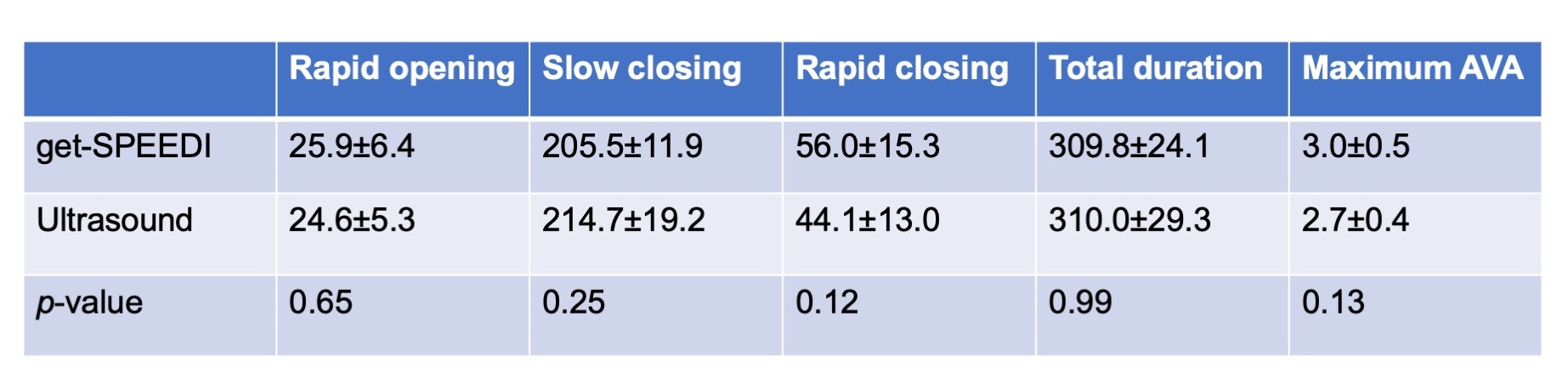
As shown in Fig. 1A, get-SPEEDI produced good MR image quality for visualizing the opening and closing process of the AV. Similarly, the M-mode ultrasound echocardiograms showed visible traces corresponding to the AV dynamic process (Fig. 1B). The three phases of AV (RO, SC, and RC) can be clearly identified in the AVA time courses from get-SPEEDI data (Fig. 2). The measured values of the opening and closing characteristics from the MRI and ultrasound data are summarized in Fig. 3 and Table 1. There was no statistically significant difference between the durations of the three AV phases measured with get-SPEEDI MRI and ultrasound echocardiography. The AVAmax values measured with the two modalities were also comparable. In addition, it was noted that the small differences between get-SPEEDI and ultrasound in the measurements of SC and RC were complementary, resulting in a good agreement for the total duration of the opening and closing processes (~ 310 ms). This observation may result from inaccuracies in determining the exact echocardiographic frame when the transition from slow to rapid closing occurred (see Fig. 1B).Discussion and Conclusions
In this study, we compared the opening and closing characteristics of the AV measured by get-SPEEDI MRI and ultrasound echocardiograms. This comparison indicates a substantial agreement between the techniques, suggesting that get-SPEEDI MRI can be a reliable technique for imaging AV dynamics and revealing abnormalities related to AV diseases. Compared to ultrasound echocardiograms, get-SPEEDI MRI can offer higher spatial resolution and better soft tissue contrast for visualizing the movement of all three leaflets throughout the cardiac cycle. Thus, get-SPEEDI MRI holds great potential to become a complementary or alternative diagnostic tool for valvular imaging.Acknowledgements
This work was supported in part by the National Institutes of Health (Grant No. 5R01EB026716-01, 1S10RR028898-01, and 1R03EB034480-01). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.References
1. Baumgartner H, et al. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr 2017;30:372-392.
2. Zoghbi WA, et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2017;30:303-371.
3. Leyh RG, Schmidtke C, Sievers HH and Yacoub MH. Opening and Closing Characteristics of the Aortic Valve After Different Types of Valve-Preserving Surgery. Circulation. 1999;100:2153-2160.
4. La Grutta L, et al. TAVI imaging: over the echocardiography. Radiol Med. 2020;125:1148-1166.
5. Zhong Z, Sun K, Karaman MM, Zhou XJ. Magnetic resonance imaging with submillisecond temporal resolution. Magn Reson Med. 2021;85(5):2434-2444
6. Zhong Z, Sun K, Dan G, Luo Q, Farzaneh-Far A, Karaman MM, Zhou XJ. Visualization of Human Aortic Valve Dynamics Using Magnetic Resonance Imaging with Sub-Millisecond Temporal Resolution. J Magn Reson Imaging. 2021;54:1246-1254.
7. Chan TF, Vese LA. Active contours without edges. IEEE Trans Image Process. 2001;10:266-277.
Figures