0279
Automatic planning of T2-weighted fetal scans at 0.55T using fetal brain landmark detection1Centre for the Developing Brain, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom, 3MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 4London Collaborative Ultra High Field System (LoCUS), King's College London, London, United Kingdom, 5CNRS, CRMSB, UMR 5536, IHU Liryc, Université de Bordeaux, Bordeaux, France, 6Department of Women & Children’s Health, King's College London, London, United Kingdom
Synopsis
Keywords: Data Acquisition, Data Acquisition, Fetal
Motivation: Fetal MRI plays an important role in clinical and research settings. The variability of the fetal position and extensive fetal motion, however, create challenges limiting the use of fetal MRI mainly to specialist centres.
Goal(s): Real-time fully automatic planning of true radiological fetal brain planes for anatomical TSE scans.
Approach: Deep-learning based detection of key landmarks in the fetal brain on a whole-uterus EPI scan enables the subsequent automatic calculation of the radiological plane for the TSE scan.
Results: Prospective results on three fetal MRI scans on a clinical low-field 0.55T MRI scanner illustrate the ability of the framework to perform diagnostic planning.
Impact: Fully automated planning of radiological planes for low-field fetal MRI demonstrates time efficiency and carries the potential to significantly widen accessibility to fetal MRI beyond specialist centres.
MRI plays an increasing and growing role in both clinical antenatal diagnosis and research, complementing Ultrasound screening for suspected fetal pathologies. While MRI offers higher spatial resolution, enhanced soft tissue contrast and a wide range of functional contrasts, it poses unique challenges, such as safety considerations as well as involuntary fetal motion and variability in fetal position and maternal surroundings. Specialist radiographers are thus essential. Recently, low-field 0.55T MRI, with the benefits of increased field homogeneity, larger bore size and longer T2* among others has been shown [1], carrying the potential to widen access to this modality. Radiological assessment requires high-quality images in defined planes for various measurements such as the bi-parietal diameter and trans-cerebellar diameter, to assess fetal growth [2]. While recent advances in Slice-to-Volume-Reconstruction (SVR) [3] allow 3D reconstructed high-resolution results and thus re-orientation to true brain anatomy, this technique is only available in specialist centres. Here, we present an automatic landmark detection and sequence planning, encompassing landmarking concepts from cardiac MRI [4]. Recent work highlighted the use of real-time AI methods in fetal MRI to perform quality control, automatic segmentation [5, 6] and automatic tracking [7]. Here, we present an automatic, Gadgetron-based fast landmark detection and subsequent automatic planning of true fetal brain scans, implemented, tested and evaluated on prospective 0.55T low field fetal MRI scans.
Methods:
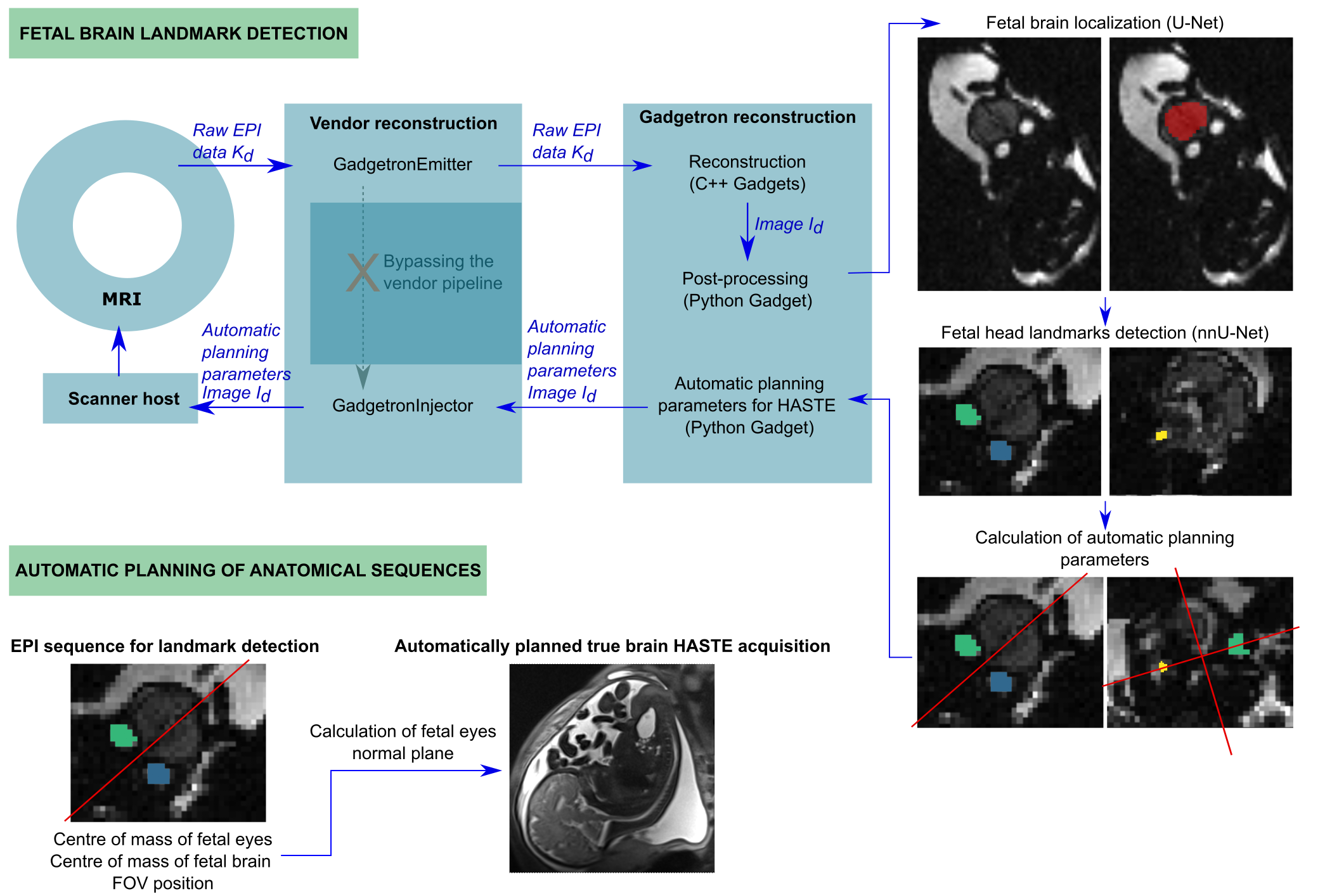
The automatic sequence planning framework was implemented on a 0.55T scanner (MAGNETOM Free.Max, Siemens Healthcare, Erlangen, Germany). A whole uterus multi-echo gradient-echo single-shot EPI sequence in coronal maternal orientation (resolution=3.13–4.03, TE=[46/120/194/268/342]ms, slices=50–59, matrix size=100x100–128x128, resolution=3.13–4.03 mm), acquired to perform T2* mapping, was used subsequently to extract the fetal head position. The pipeline consists of two steps (illustrated in Figure 1). First, the EPI sequence was modified to export the data to a Gadgetron pipeline. A two-step deep learning-based detection using the nnUNet [8] framework in python first localises the fetal head and calculates the centre of mass (CoM) and then extracts specific head landmarks (fetal eyes and cerebellum) and stores the CoM and the patient coordinate system into a file. The first network was trained on 125 labelled fetal datasets acquired at 1.5T/3T and tested on 29 0.55T fetal datasets. The second was trained and tested on cropped images of 76/15 fetal subjects, respectively, for the eyes and cerebellum. The mean distance in millimetres between automatic and manual landmarks was calculated. Next, the following HASTE sequence was modified to use the stored information to calculate a plane crossing the midline of the fetal eyes and orthogonal to their connection line. Figure 1 illustrates a comprehensive schemata. The entire real-time pipeline was acquired prospectively in three pregnant volunteers (GA 34-38 weeks, MEERKAT study REC19/LO/0852) on the 0.55T MRI scanner. The resulting automatically planned sagittal planes were assessed by a radiographer and a radiologist with >15 years of fetal MRI experience answering the questions “Would you repeat this scan for planning purposes?” and “Rate the quality [0”unusable”-5”perfect”].” respectively.
Results:
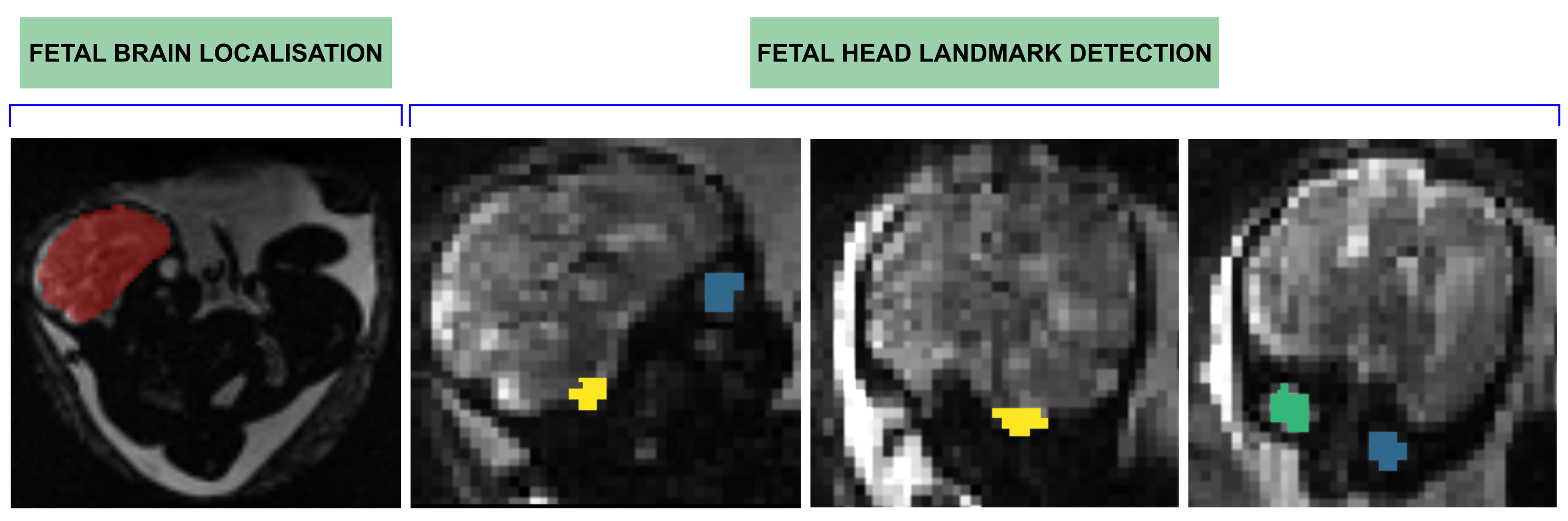
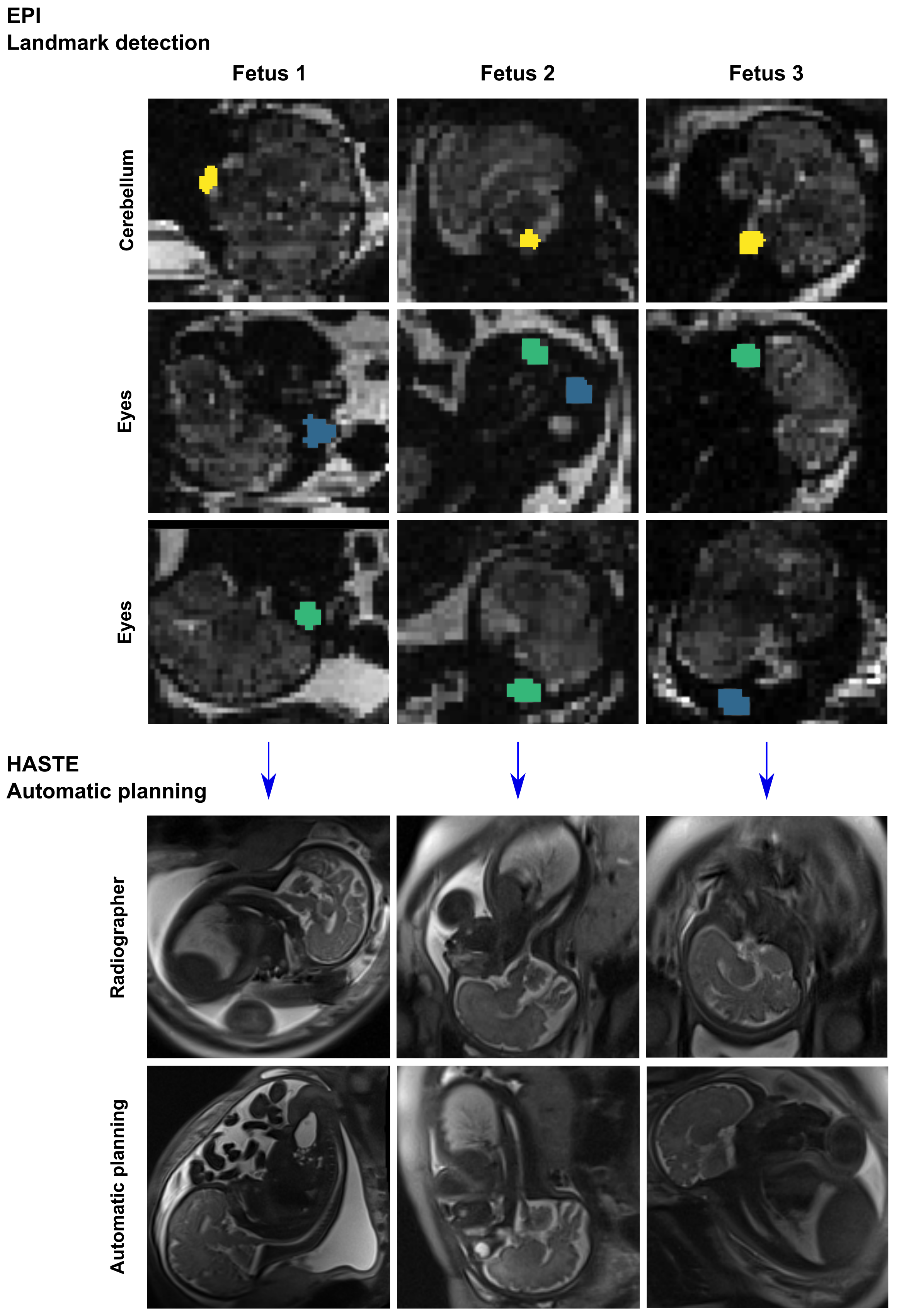
The brain localization task, trained on mid/high-field data, achieved an overall DSC of 82.3±17.5% and IoU of 82.3±17.5% when tested on low-field scans across all TEs, fetal positions, and gestational ages. Regarding the landmarks, the mean distance between the centre of the cerebellum label for automatic/manual landmarks was 6.47 mm. Fig. 2 shows the predicted brain and landmarks segmentations for one fetal subject of the landmarks model test set. Fetal head landmarks were successfully localised and the HASTE sequences planned in three fetal scans. Fig. 3 displays the automatic planning results and manual radiographer-performed planning. Quantitative evaluation of the achieved sagittal planes resulted in one scan where a repeat would be required both for the automatic and the radiographer-planned attempts. Radiological scoring (1-5) was on average 3.0±0.0 for automatic and 2.33±1.27 for the radiographer-planned attempts.
Discussion and Conclusion:
Automatic planning of T2-weighted fetal MRI was demonstrated in three fetal subjects and comparison with manual planning revealed good agreement. Further planes and focus areas such as cardiac views will be addressed in the future. Planning sequences in fetal protocols based on information from the previously acquired images is novel and opens up the possibility of performing fetal MRI more widely in non-specialist centres.
Acknowledgements
The authors thank all pregnant women and their families for taking part in this study, the midwives Imogen Desforges, Chidinma Iheanetu Oguejiofor, and Maggie Lee for their invaluable efforts in recruiting and looking after the women in this study as well as Kathleen Colford, Kamilah St Clair, and Massimo Marenzana for their involvement in the acquisition of these datasets. This work was supported by a Wellcome Trust Collaboration in Science grant [WT201526/Z/16/Z], a UKRI FL fellowship, an NIHR Advanced Fellowship to LS [NIHR3016640], an EPSRC Research Council DTP grant [EP/R513064/1] and by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z]. The views presented in this study represent these of the authors and not of Guy’s and St Thomas’ NHS Foundation Trust.References
[1] Aviles Verdera J, Story L, Hall M, Finck T, Egloff A, Seed PT, Malik SJ, Rutherford MA, Hajnal JV, Tomi-Tricot R, Hutter J. Reliability and Feasibility of Low-Field-Strength Fetal MRI at 0.55 T during Pregnancy. Radiology. 2023 Oct;309(1):e223050. doi: 10.1148/radiol.223050.
[2] Kyriakopoulou V, Vatansever D, Davidson A, Patkee P, Elkommos S, Chew A, Martinez-Biarge M, Hagberg B, Damodaram M, Allsop J, Fox M, Hajnal JV, Rutherford MA. Normative biometry of the fetal brain using magnetic resonance imaging. Brain Struct Funct. 2017 Jul;222(5):2295-2307. doi: 10.1007/s00429-016-1342-6.
[3] Uus A, Zhang T, Jackson LH, Roberts TA, Rutherford MA, Hajnal JV, Deprez M. Deformable Slice-to-Volume Registration for Motion Correction of Fetal Body and Placenta MRI. IEEE Trans Med Imaging. 2020 Sep;39(9):2750-2759. doi: 10.1109/TMI.2020.2974844.
[4] Xue H, Artico J, Fontana M, Moon JC, Davies RH, Kellman P. Landmark Detection in Cardiac MRI by Using a Convolutional Neural Network. Radiol Artif Intell. 2021 Jul 14;3(5):e200197. doi: 10.1148/ryai.2021200197.
[5] Faghihpirayesh, R., Karimi, D., Erdoğmuş, D., Gholipour, A. (2022). Deep Learning Framework for Real-Time Fetal Brain Segmentation in MRI. In: Licandro, R., Melbourne, A., Abaci Turk, E., Macgowan, C., Hutter, J. (eds) Perinatal, Preterm and Paediatric Image Analysis. PIPPI 2022. Lecture Notes in Computer Science, vol 13575. Springer, Cham. https://doi.org/10.1007/978-3-031-17117-8_6.
[6] S. S. M. Salehi et al., "Real-time automatic fetal brain extraction in fetal MRI by deep learning," 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 2018, pp. 720-724, doi: 10.1109/ISBI.2018.8363675.
[7] Neves Silva, S, Aviles Verdera, J, Tomi-Tricot, R, et al. Real-time fetal brain tracking for functional fetal MRI. Magn Reson Med. 2023; 90: 2306-2320. doi: 10.1002/mrm.29803[8] Isensee, F., Jaeger, P.F., Kohl, S.A.A. et al. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat Methods 18, 203–211 (2021). https://doi.org/10.1038/s41592-020-01008-z.
Figures