0278
Navigator-gated Simultaneous Multi-Slice STEAM Diffusion Tensor Cardiac Magnetic Resonance1National Heart and Lung Institute, Imperial College London, London, United Kingdom, 2CMR Unit, The Royal Brompton Hospital, London, United Kingdom, 3Biomedical Engineering, King's College London, London, United Kingdom, 4Siemens Healthineers, London, United Kingdom
Synopsis
Keywords: Data Acquisition, Diffusion Tensor Imaging, Simultaneouse Multi-Slice; Navigator-gated Acqusition
Motivation: Low scanning efficiency of stimulated echo acquisition mode (STEAM) diffusion tensor cardiac magnetic resonance images (DT-CMR) limits its clinical translation.
Goal(s): We aimed to improve the slice coverage efficiency of DT-CMR utilizing simultaneous multi-slice (SMS) techniques.
Approach: The navigator-gated (Nav) SMS STEAM acquisition, integrated with a biofeedback system, was introduced, enabling controlled breathing and respiratory motion compensation.
Results: Nav SMS STEAM acquisition reduced scanning time by 46±6% compared to single-band (SB) acquisition. No significant difference in global mean MD and FA was observed, but a lower median |E2A| was noted for the SMS basal slice.
Impact: Our proposed Nav SMS STEAM acquisition would reduce the total breath-hold duration of STEAM DT-CMR acquisitions, enhancing clinical feasibility. Improved efficiency could also lead to whole heart coverage in DT-CMR scans, essential for example, in myocardial infarction.
Introduction
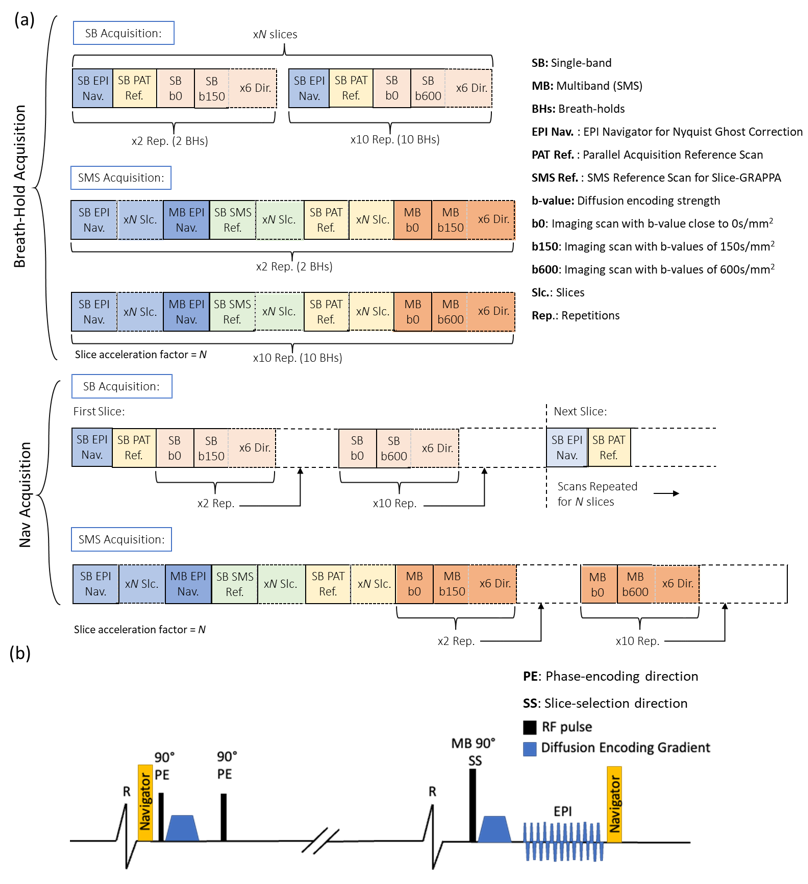
Stimulated echo acquisition mode (STEAM) is well-established for in-vivo diffusion tensor cardiac magnetic resonance (DT-CMR). However, its intrinsically low signal-to-noise ratio (SNR) mandates numerous repetitions of diffusion-weighted (DW) images, prolonging the scanning duration. Simultaneous multi-slice (SMS) parallel imaging (PI) techniques have the potential to enhance acquisition efficiency by capturing signals from multiple slices simultaneously. While SMS techniques have been successfully used in neuroimaging [1], only a limited number of studies have applied this technique to in-vivo DT-CMR [2, 3]. SMS image reconstruction leverages coil sensitivity encoding to disentangle the simultaneously acquired slices. Conventionally, in-vivo STEAM DT-CMR is acquired using breath-holding (BH). Even though SMS decreases the total number of breath-holds, its application is limited due to the increased number of reference scans required per breath-hold [Figure 1(a)]. To address this, we introduce a navigator-gated SMS DT-CMR acquisition with controlled breathing, allowing only one set of reference scans to be acquired for multiple repetitions, reducing the total scanning time by 46±6% compared to single-band (SB) DT-CMR.Methods
We combined our in-house developed STEAM DT-CMR research sequence [1] with pencil beam navigators [Figure 1(b)] and real-time biofeedback, enabling controlled-breathing acquisitions [4]. DT-CMR data in systole was acquired on a 3T scanner (MAGNETOM Vida, Siemens Healthineers, Erlangen, Germany) for 8 healthy volunteers. Protocol parameters included: navigator acceptance window of 4mm, 2 DT-CMR slices (12 averages of “b0” = 30smm-2, 10 averages of b600 = 600smm-2, 2 averages of b150 = 150smm-2 images), slice thickness = 8mm, slice separation = 24mm, obtained with both SB and SMS mode (SMS slice acceleration factor = 2). Zonal excitation in phase-encoding (PE) direction with an in-plane PI acceleration factor of 2 was used to minimize the echo time, achieving a resolution of 1.4x1.4x8.0mm3 (interpolated from 2.8x2.8x8.0mm3). Vendor-provided image reconstruction utilized GRAPPA and Slice-GRAPPA for SB and SMS methods, respectively.The navigator-gated acquisitions [Figure 1(a)] reduced the need to repeat reference scans. For two slices, SB mode required 4 reference scans, including 2 EPI phase correction navigator scans (one per slice) and 2 in-plane PI reference scans for GRAPPA reconstruction (one per slice). The SMS mode required 7 reference scans, including 2 SB EPI phase correction navigator scans (one per slice), 1 multi-band (MB) EPI phase correction navigator scan, 2 SB SMS reference scans (one per slice) for Slice-GRAPPA reconstruction and 2 SB in-plane PI reference scans (one per slice) for GRAPPA reconstruction of the SB SMS reference scans. In total, the Nav STEAM acquisition would take 172 scans with SB mode and 91 scans with SMS mode for two slices at 100% navigator efficiency, leading to a 47% reduction in the number of scans.
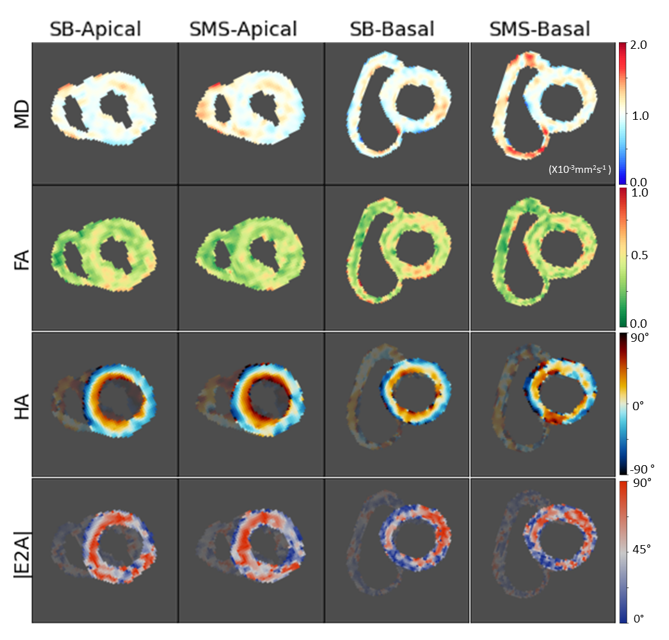
DT-CMR data was analyzed using our in-house built MATLAB post-processing tool [5]. DT-CMR parameters derived from the diffusion tensor model included mean diffusivity (MD), fractional anisotropy (FA), helix angle (HA) and absolute secondary vector angulation (|E2A|).
Results
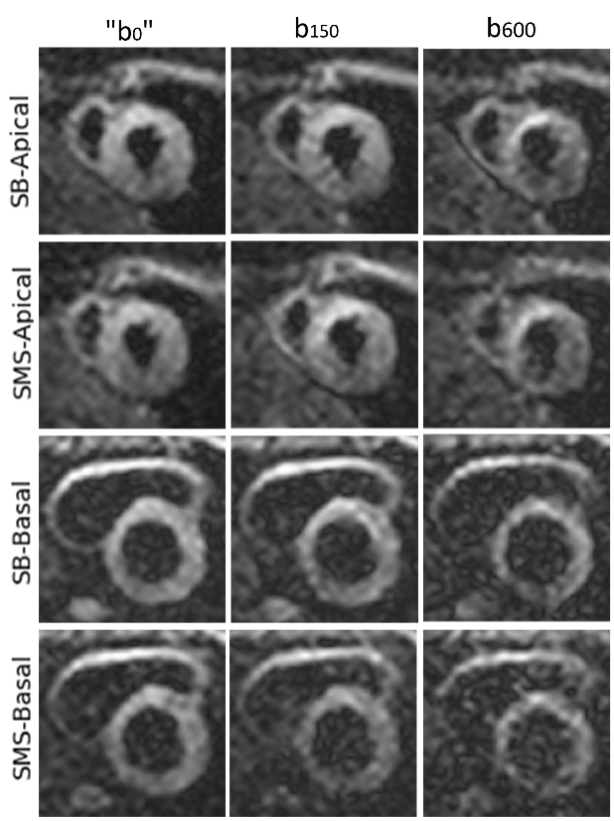
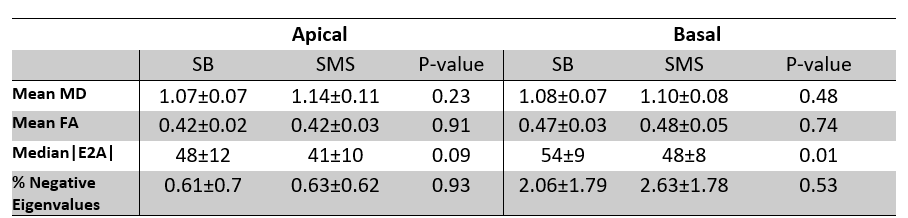
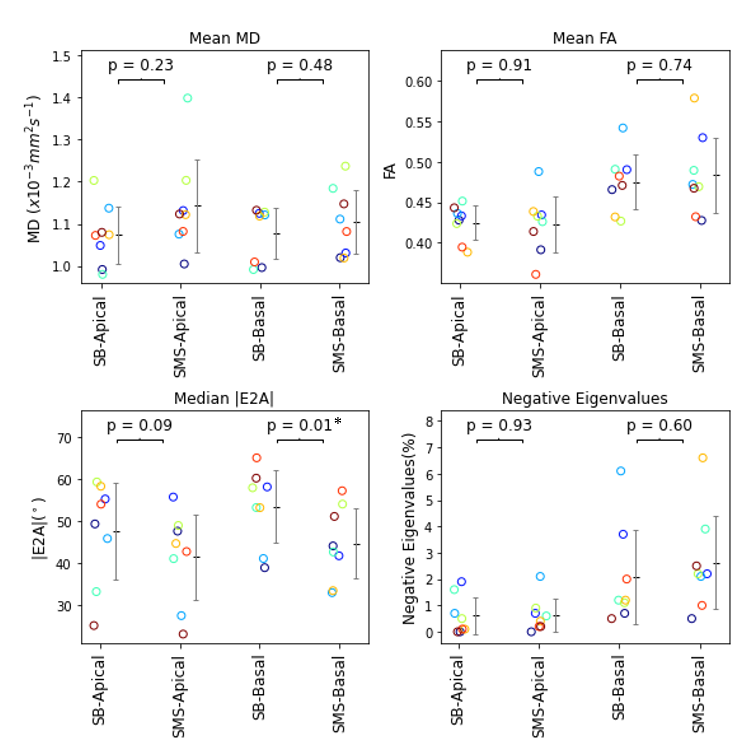
Figure 2 shows example SB and SMS DW images with different b-values. Figure 3 demonstrates the typical DT-CMR parametric maps (MD, FA, HA and |E2A|) obtained from a healthy volunteer. Statistical evaluation [Table 1] underlines that there is no significant difference between the global mean values of MD (Apical: p=0.23; Basal: p=0.48) and FA (Apical: p=0.91; Basal: p=0.74) between SB and SMS methods. Examination of |E2A| median values across the volunteers indicates a lower value for SMS method (Apical: |E2A|SB = 48±12°; |E2A|SMS=41±10°; Basal: |E2A|SB=54±9°, |E2A|SMS=48±8°), with the apical slice exhibiting no significant difference (p=0.09), in contrast to the basal slice where a significant difference is noted (p=0.01). Additionally, there is no significant difference in the percentage of negative eigenvalues that appeared in the obtained diffusion tensors in the left ventricle (a higher proportion indicates poorer quality data). Figure 4 provides insights into the variation of these DT-CMR parameters between scans, slices and individual healthy volunteers (color-coded).The average acquisition time was 433±80s with the SB method and 232±43s using the SMS method. The median navigator acceptance rate stood at 74%, with an interquartile range of 11%. The experimental scanning time reduction was 46±6% using SMS over SB.
Conclusion
Our Nav SMS STEAM DT-CMR method has shown a 46±6% reduction in scanning time over equivalent SB protocols for two slices. While there is no significant difference between the obtained global mean MD and FA for both slices compared between the SB and SMS method, differences in global |E2A| values for the basal slice were obtained in this volunteer dataset. Further investigation with a larger sample size will be required.Acknowledgements
The authors would like to acknowledge funding from the British Heart Foundation programme grant (RG/19/1/34160) and the EPSRC Centre for Doctoral Training in Smart Medical Imaging, co-funded by Siemens Healthineers grant (EP/S022104/1).References
[1] K. Setsompop et al., Magnetic Resonance in Medicine, 2012, doi: abs/10.1002/mrm.23097
[2] A. Z. Lau et al., Magnetic Resonance in Medicine, 2015, doi: abs/10.1002/mrm.25200
[3] C. Mekkaoui et al., NMR in Biomedicine, 2017, doi: 10.1002/nbm.3426
[4] S. Nielles-Vallespin et al., Magnetic Resonance in Medicine, 2013, doi: 10.1002/MRM.24488
[5] P. F. Ferreira et al., J Cardiovasc Magn. Reson., 2014, doi: 10.1186/s12968-014-0087-8
Figures