0273
Liver T1, T2 and ADC Magnetic Resonance Fingerprinting in a single breath-hold1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 3Millennium Institute for Intelligent Healthcare Engineering (iHEALTH), Pontificia Universidad Católica de Chile, Santiago, Chile, 4School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: MR Fingerprinting, MR Fingerprinting
Motivation: Single breath-hold simultaneous T1, T2 and ADC abdominal Magnetic Resonance Fingerprinting (MRF) in liver would allow for fast and comprehensive liver tissue characterization.
Goal(s): To develop a fast MRF sequence for T1, T2 and ADC quantification on liver tissue in a single breath-hold at 3T
Approach: Radial spoiled-GRE ~16-second acquisition with magnetization preparation modules for T1, T2 and ADC encoding was proposed, with an optimized diffusion-preparation module. Sequence was evaluated in phantoms and in 11 healthy subjects.
Results: T1, T2 and ADC quantification shows good correlation with reference maps in phantoms and good agreement in vivo against clinical scans.
Impact: Simultaneous quantification of T1, T2 and ADC in liver tissue in a single-scan is now possible with this proposed MRF sequence, allowing for a more comprehensive evaluation of hepatic disease through co-registered multiparametric imaging.
Introduction
Multiparametric MRI promises to provide a more comprehensive assessment of liver disease1,2. Multiparametric studies of T1, T2 and apparent diffusion coefficient (ADC) are traditionally performed in sequential scans3, which are prone to mis-registration artifacts. Recently, Magnetic Resonance Fingerprinting (MRF) has been proposed for simultaneous T1, T2 and ADC mapping of the brain4-6. However, single-breath-hold simultaneous T1, T2 and ADC MRF for liver tissue characterization has not been investigated. In this study we propose a triggered 16-heartbeat acquisition that enables fast, simultaneous T1, T2 and ADC quantification in a single scan of ~16s. The proposed sequence has been evaluated in phantoms and in eleven healthy subjects.Methods
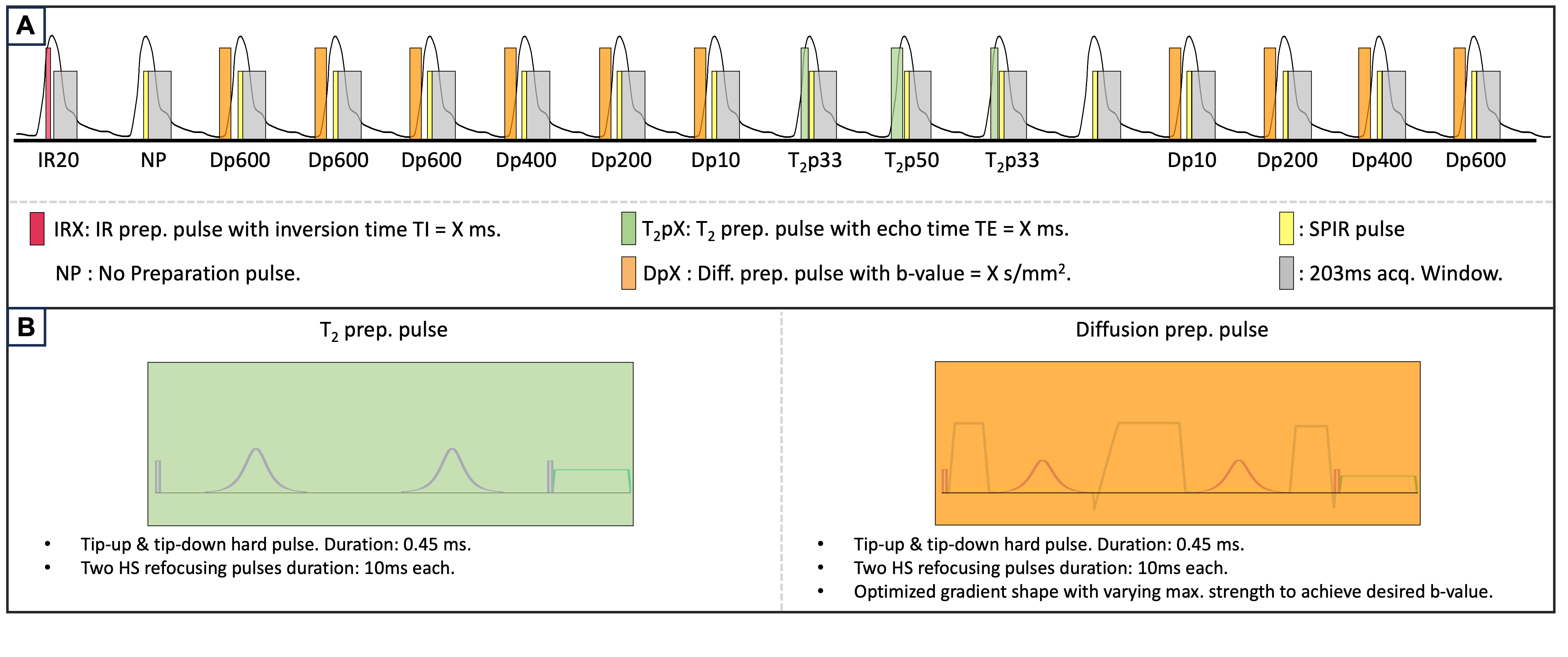
A GRE MRF sequence with golden radial trajectory and varying magnetization preparation pulses is proposed (Figure 1a). The acquisition consists of 16 blocks preceded by the following preparation pulses: IR (TI = 20ms), three T2 preparation (T2ps(repetitions) = {33(2),50(1)}ms), ten diffusion preparation (b-values(repetitions) = {10(2), 200(2), 400(2) and 600(4)} s/mm2) and two blocks without preparation. The diffusion preparation had a duration of 50ms, including two adiabatic refocusing pulses of 10.3 ms inserted in-between the diffusion gradients to increase robustness against high field inhomogeneities7. The pulse was optimized to reach the highest possible b-value for a given diffusion preparation, given hardware max. gradient and slew-rate specifications, and gradients were applied simultaneously along the three Cartesian axes. The presence of short eddy currents was alleviated by leaving a 1-ms gap between each gradient lobe and its consecutive RF. The gradient waveforms optimization problem had restrictions to compensate for concomitant gradients, and up to first-order moment nulling for increased robustness against body motion and blood flow. Each acquisition block contains a train of 30 shots with sinusoidally varying flip angles in the range 10°-20°. Acquisition parameters include: TE=3.3ms and TR=7.0ms, 1x1mm2 in-plane resolution, 6mm slice thickness and acquisition time ~16s. The acquisition was triggered at a fixed delay of 200ms using PPU. Reconstruction was performed using low-rank inversion approach8 and regularized with a multi-contrast patch-based higher-order reconstruction9. All scans were performed on a 3T scanner (Achieva TX, Philips; Gmax=62 mT/m, Smax=100 T/m/s). The proposed approach was evaluated in phantoms: a) a standardized T1MES phantom for T1, T2 validation and b) a set of tubes filled with a fixed concentration of NiCl2 and Agarose to obtain physiological T1, T2 values, as well as a varying concentration of polyvinylpyrrolidone to generate a range of isotropic diffusion values10. Measurements were compared against SE references. The sequence was additionally tested in eleven healthy volunteers (5 female, mean±SD age=30.1±3.7y) and compared against conventional individual single breath hold maps (T1-MOLLI (2x2x6mm), T2-GRaSE (2x2x6mm), and DWI-SE (3x3x4mm)) through Bland-Altman plots. Quantification for each subject was done by measuring T1, T2 and ADC in eight 10mm-diameter ROIs manually placed in the liver avoiding contamination from visible blood vessels.Results
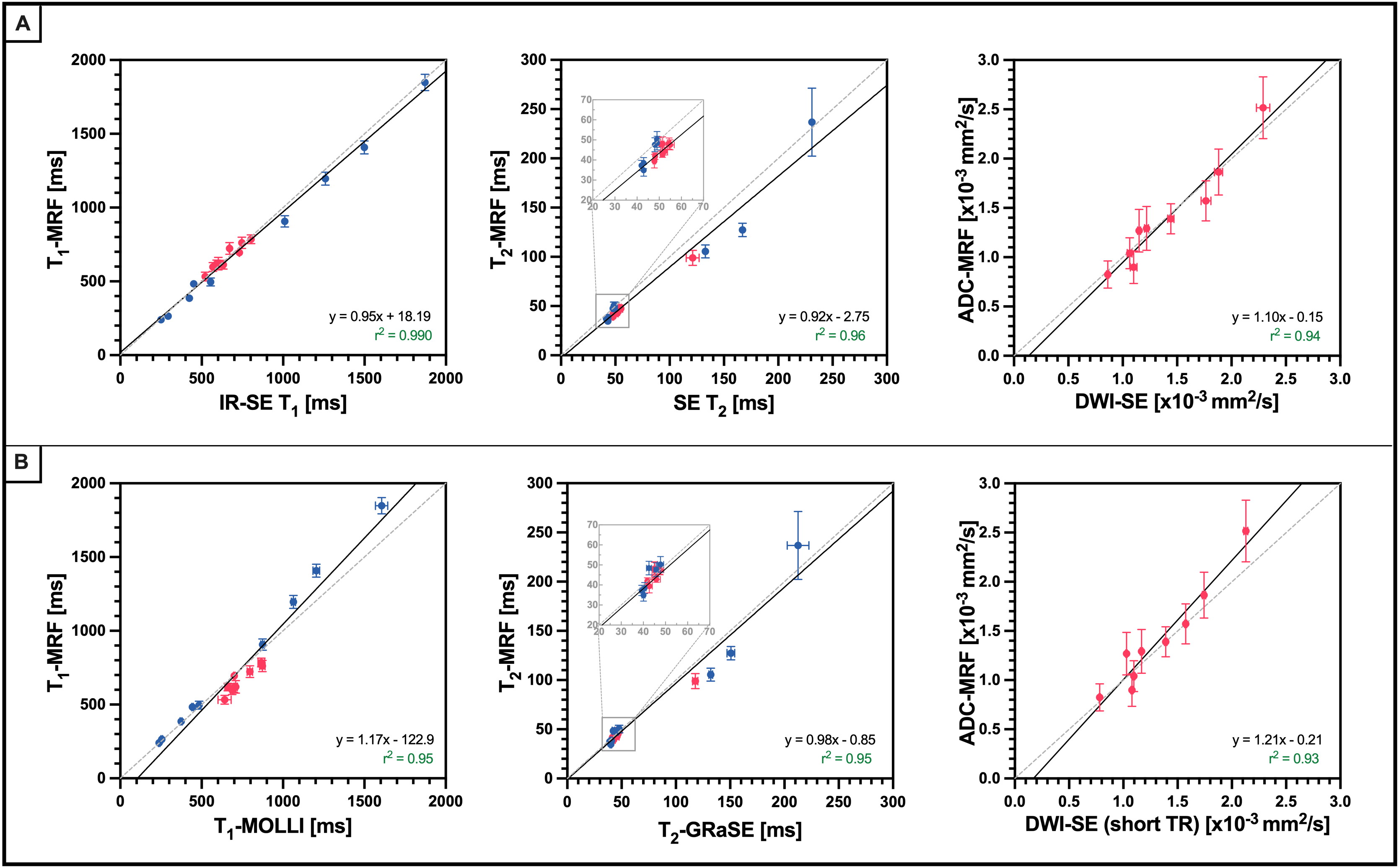
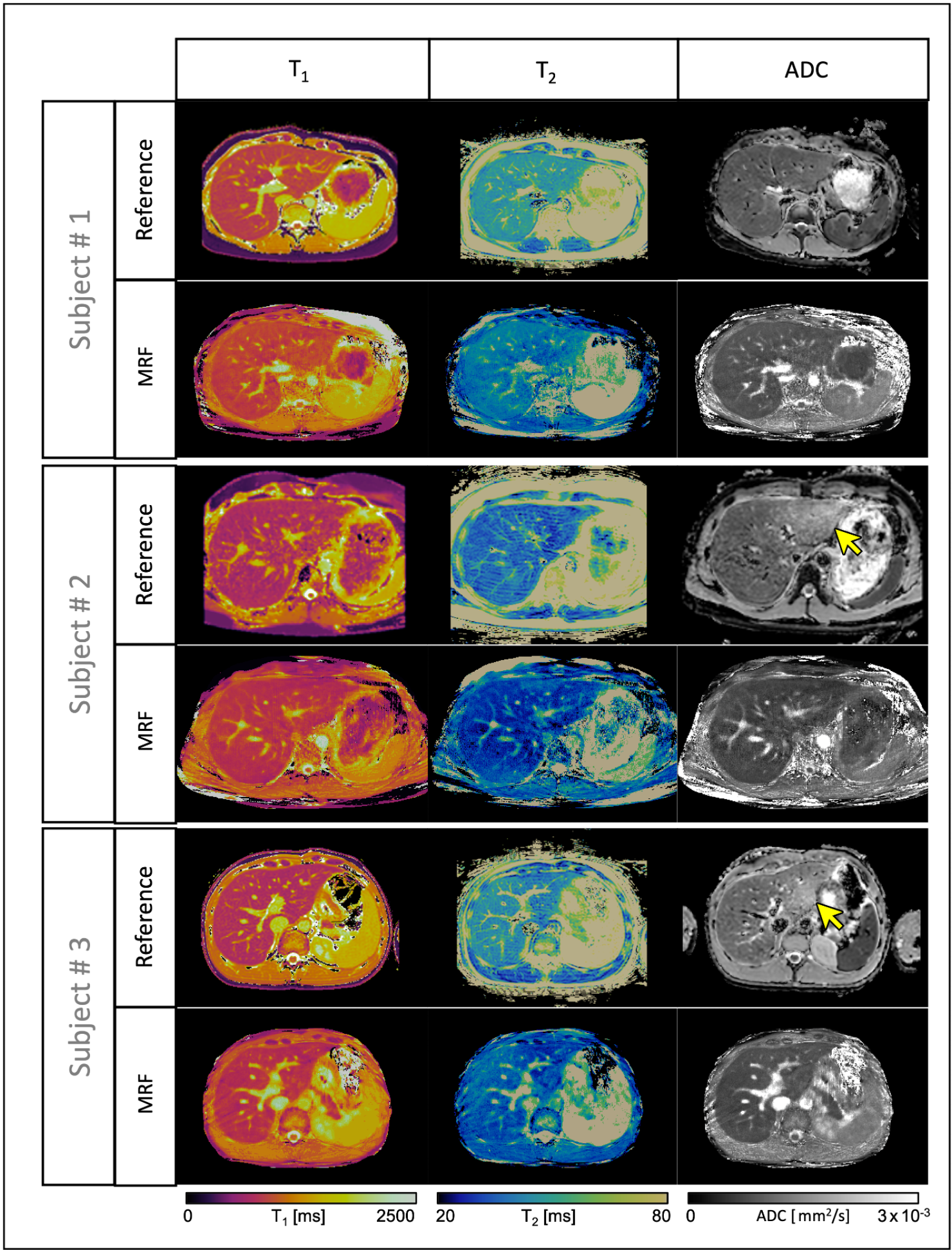
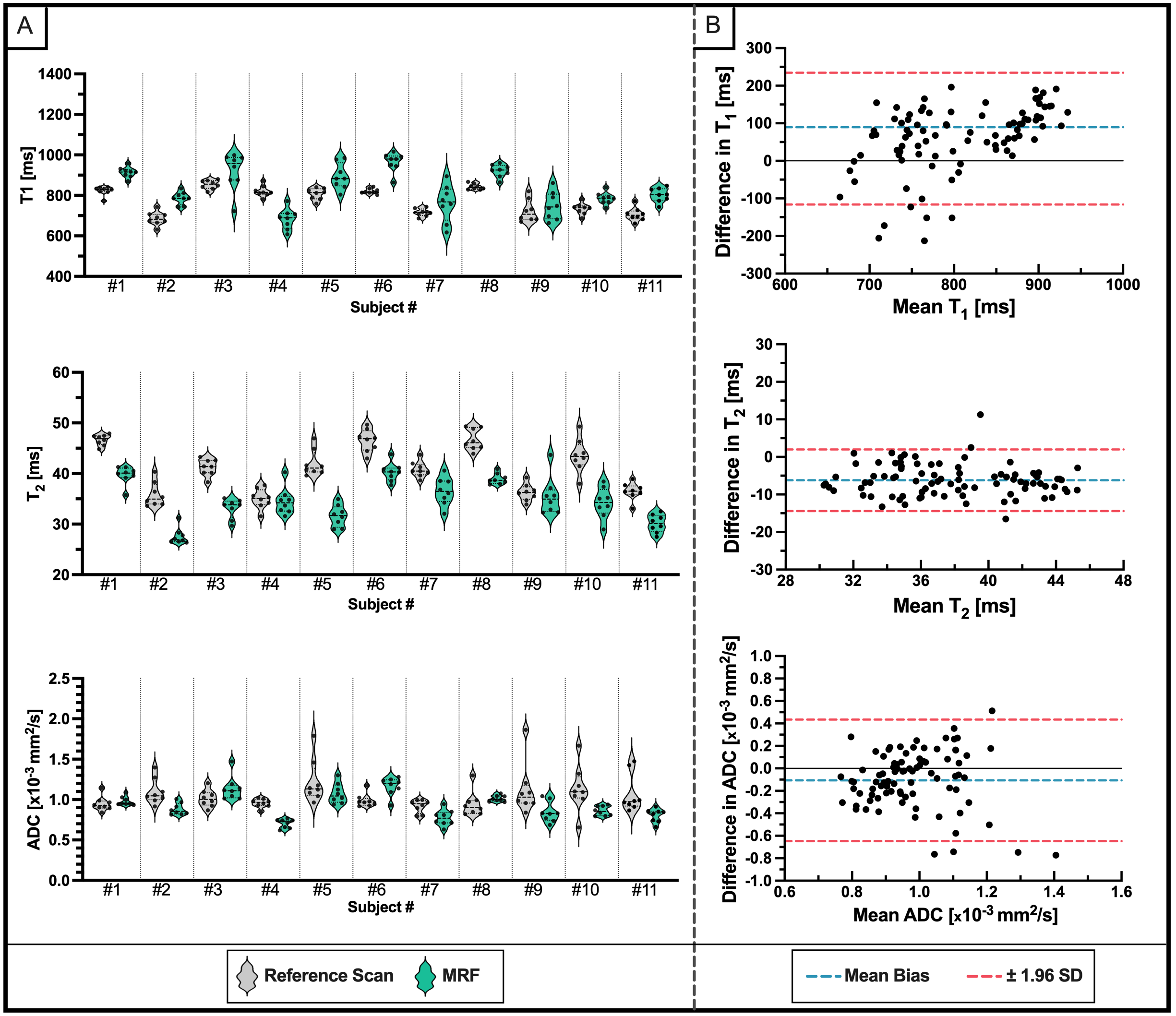
Phantom evaluation of T1-MRF, T2-MRF and ADC-MRF maps against their respective references is shown in Fig.2. Pearson r2 coefficients are excellent (r2>0.90 for all cases). A comparison between MRF-derived maps and their respective references for in vivo liver quantification is shown in Fig.3. For each subject, the co-registered MRF maps were obtained from a single breath-held acquisition of ~16s. The corresponding reference maps were obtained in 14s, 18s and 45s respectively. Fig. 4A shows the Quantitative evaluation of all healthy subjects on a per-subject basis, and Bland-Altman analysis of agreement between MRF and their corresponding clinical sequences are shown in Fig.4.Discussion
MRF-derived T1, T2 and ADC quantification is in good agreement with their respective reference measurements in phantom and healthy subjects. Bland-Altman plots showed a small negative bias in T2 and a significative T1 underestimation in comparison to T2-GRaSE and T1-MOLLI, which has been previously reported11-13. Several overestimated ADC-SE measurements are observed in some subjects. This corresponds always to ROIs within the left lobe (see yellow arrows inf Figure 3), where cardiac motion leads to incorrect diffusion preparation and introduces a positive bias in ADC quantification. This bias is not observed in the proposed ADC-MRF, demonstrating more robustness of the proposed technique against this type of artefacts. Multi-echo readouts will be explored as future work to enable water-fat estimation and a more comprehensive liver tissue characterization. Future work will also evaluate this technique in a larger cohort of healthy volunteers and patients with hepatic disease.Acknowledgements
This work was supported by the following grants: (1) EPSRC P/V044087/1,(2) BHF programme grant RG/20/1/34802, (3) Wellcome/EPSRC Centre for Medical Engineering (WT 203148/Z/16/Z), (4) Millennium Institute for Intelligent Healthcare Engineering ICN2021_004, (5) FONDECYT 121074, 1210637 and 1210638, (6) IMPACT, Center of Interventional Medicine for Precision and Advanced Cellular Therapy, ANID FB210024, (7) PhD program in Biological and Medical Engineering of the Pontificia Universidad Católica de Chile.References
1Banerjee, R. et al., J Hepatol. 2014. 2Pavlides, M. et al., J Hepatol. 2016. 3Yu, A.C. et al., Radiology 2017. 4Cao, X. et al. ISMRM2022 Abs #0101. 5Afzali, M. et al., MRM 2022. 6Fan, H. et al., MRM 2023. 7Peña-Nogales, O., et al, MRM 2019. 8Assländer, J., et al, MRM 2018. 9Bustin, A., et al, MRM 2019. 10Wagner, F. et al., PLoS ONE 2016. 11Cruz, G. et al., NMR Biomed 2020. 12Hamilton, JI. et al., MRM 2018. 13Baeßler, B. et al., Eur J Radiol 2015.
Figures