0272
Cardiac and respiratory motion extraction at 0.55T with high-amplitude Pilot Tone1Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States
Synopsis
Keywords: Motion Correction, New Devices, Pilot Tone, Low Field
Motivation: With Pilot Tone, it is challenging to extract weak modulations, specifically those related to cardiac motion, at lower B0 field strengths (<1.5T).
Goal(s): To enable the use of cardiac Pilot Tone at low-fields (0.55T).
Approach: We utilize high-amplitude pilot tone transmission in conjunction with interference mitigation to eliminate ensuing image artifacts.
Results: We demonstrate robust extraction of cardiac pilot-tone signals at 0.55T. We demonstrate ability to track motion with real-time MRI, and demonstrate the ability to separate cardiac and respiratory phases with retrospective binning. Compared to ECG, the measured timing standard deviation was 36ms for Cartesian and 47ms for spiral acquisitions.
Impact: This work makes it possible to extract cardiac motion from Pilot Tone at 0.55T, which was not possible before. Pilot Tone could potentially replace ECG gating, simplify the clinical workflow, and serve for scanners that do not employ ECG.
Introduction
Pilot Tone (PT) is a novel way of capturing cardiac and respiratory motion remotely[1-3]. When PT is employed, ECG and bellow placement or imaging navigator may be avoided for gating purposes. This can greatly simplify patient preparation, increase patient comfort, and simplifies scan planning. PT also makes it possible to do cardiac gating for the scanners that does not come with an integrated ECG.One known caveat is that the PT navigator quality is B0 field-dependent. Specifically, the modulation from motion is proportional to the resonance frequency and therefore the B0 field strength. It is challenging to extract weaker motion, e.g. cardiac motion, on mid- and low-field systems[4].
Here, we use a high-amplitude pilot tone in combination with External Dynamic InTerference Estimation and Removal (EDITER) [6] to obtain cardiac and respiratory signals at 0.55T. We demonstrate this enables extraction of reliable cardiac and respiratory motion at 0.55T, without compromising image quality. The only added cost is enabling additional receiver coils distant to the imaging volume for interference measurement (a.k.a. sniffer coils).
Methods
To generate PT signal, we used a general-purpose signal generator (AFG3252, Tektronix), with a 27MHz dipole antenna. The antenna was positioned 1m away from back of the scanner. PT frequency was placed approximately 200kHz away from the center frequency.We used the EDITER algorithm for passive interference removal[6]. EDITER estimates the interference on the imaging coils using multiple sniffer coils, and subtracts it to get corrected MRI signal. For the sniffer antennas, we used the 3 most distant elements from the table-integrated spine coil (Figure 1a). PT extracted from sniffer coils were fitted to the PT from imaging coils and subtracted to further remove interference from PT signal. For comparison, similar to literature, model subtraction of PT was done as described in Solomon et al [4].
Experiments were performed using a whole-body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers). Real-time spiral images acquired with RTHawk (Vista.ai, Palo Alto, California) system. PT was tested using a spiral golden-angle bSSFP sequence, with a TR of 5.3ms, which also dictates the temporal resolution of PT navigators. PT was also tested with a product real-time Cartesian bSSFP sequence (BEAT-Interactive, Siemens Healthineers).
PT estimation and image reconstruction was performed offline MATLAB (Mathworks, Inc., Natick, MA). Figure 1c contains the PT processing pipeline. Image reconstruction was performed with BART[7]. View-Sharing (VS) reconstruction used 72 arms/frame (374ms) and Temporal Finite Difference (TFD) reconstruction used 17 arms/frame (88.4ms). For XD-GRASP reconstruction, spiral arms were binned into 6 respiratory and 20 cardiac phases.
Results
Figure 2 shows the effectiveness of EDITER for removing the artifacts induced by high-amplitude PT. Residual artifacts were further suppressed with combination of EDITER and TFD constraint reconstruction.Figure 3 illustrates validation of extracted respiratory and cardiac PT waveforms. Respiratory PT showed an excellent match with liver dome movement. Similarly, cardiac PT shows high correlation with both cardiac motion on the real-time image and the ECG reference. The standard deviation of the delay between the ECG R-wave and the PT peak was measured as 47ms for spiral and 36ms for Cartesian acquisition, which corresponds to approximately 9 PT samples.
Figure 4 demonstrates XD-GRASP reconstruction where the cardiac and respiratory motion states were separated using high-amplitude PT. Figure 4a shows the motion of the chest wall (A-P) and vessels (S-I). Figure 4b shows one heartbeat and the contrast change in the vessels.
Discussion
Similar to conventional PT at conventional B0 field strengths, high-amplitude PT at 0.55T is effective for cardiac and respiratory navigation. We demonstrate that EDITER can significantly reduce the residual high-amplitude PT artifacts, and that constrained reconstruction further reduces any residuals.We have used a dipole antenna away from the bore to transmit the PT signal. A typical PT transmitter uses a non-resonant loop coil. Further improvement of PT and reduced artifacts can be expected by adjusting the experiment setup.
EDITER assumes no change in the system within a predetermined duration, thus is less effective in removing artifacts related with changing PT signals, which may explain residual PT artifacts. The extracted per-coil motion information can be incorporated with EDITER to improve the interference mitigation further.
This study is designed to demonstrate feasibility of high-amplitude PT for reliable respiratory and cardiac signal extraction. Further study is needed to evaluate the trade-off between artifact severity due to PT amplitude and navigator quality.
Conclusion
High-amplitude PT enables reliable cardiac motion extraction at low-field 0.55T, which was not possible before. The arising image artifacts due to increased PT amplitude are mitigated by the EDITER technique, using three additional sniffer coils.Acknowledgements
We acknowledge grant support from the National Institutes of Health (U01-HL167613), National Science Foundation (#1828736), and USC Provost (Strategic Directions in Research Award), and research support from Siemens Healthineers. We thank Peter Speier for helpful discussions.
References
Speier P, Fenchel M, Rehner R, PT-Nav: A Novel Respiratory Navigation Method for Continuous Acquisition Based on Modulation of a Pilot Tone on the MR-Receiver. Proc. ESMRMB 2015.
Speier P. Skip the Electrodes, But Not A Beat: The Engineering Behind the Beat Sensor. MAGNETOM Flash. 2023;83:16-26.
Falcão MBL, Di Sopra L, Ma L, Bacher M, Yerly J, Speier P, Rutz T, Prša M, Markl M, Stuber M, Roy CW. Pilot tone navigation for respiratory and cardiac motion-resolved free-running 5D flow MRI. Magn Reson Med. 2022 Feb;87(2):718-732. Doi: 10.1002/mrm.29023. Epub 2021 Oct 5. PMID: 34611923; PMCID: PMC8627452.
Solomon E, Rigie DS, Vahle T, et al. Free-breathing radial imaging using a pilot-tone radiofrequency transmitter for detection of respiratory motion. Magnetic Resonance in Medicine. 2021;85(5):2672-2685. doi:10.1002/mrm.28616
Anand S, Lustig M. Beat Pilot Tone: Versatile, Contact-Free Motion Sensing in MRI with Radio Frequency Intermodulation. Published online June 16, 2023. doi:10.48550/arXiv.2306.10236
Srinivas SA, Cauley SF, Stockmann JP, et al. External Dynamic InTerference Estimation and Removal (EDITER) for low field MRI. Magnetic Resonance in Medicine. 2022;87(2):614-628. doi:10.1002/mrm.28992
BART Toolbox for Computational Magnetic Resonance Imaging, DOI: 10.5281/zenodo.592960
Figures
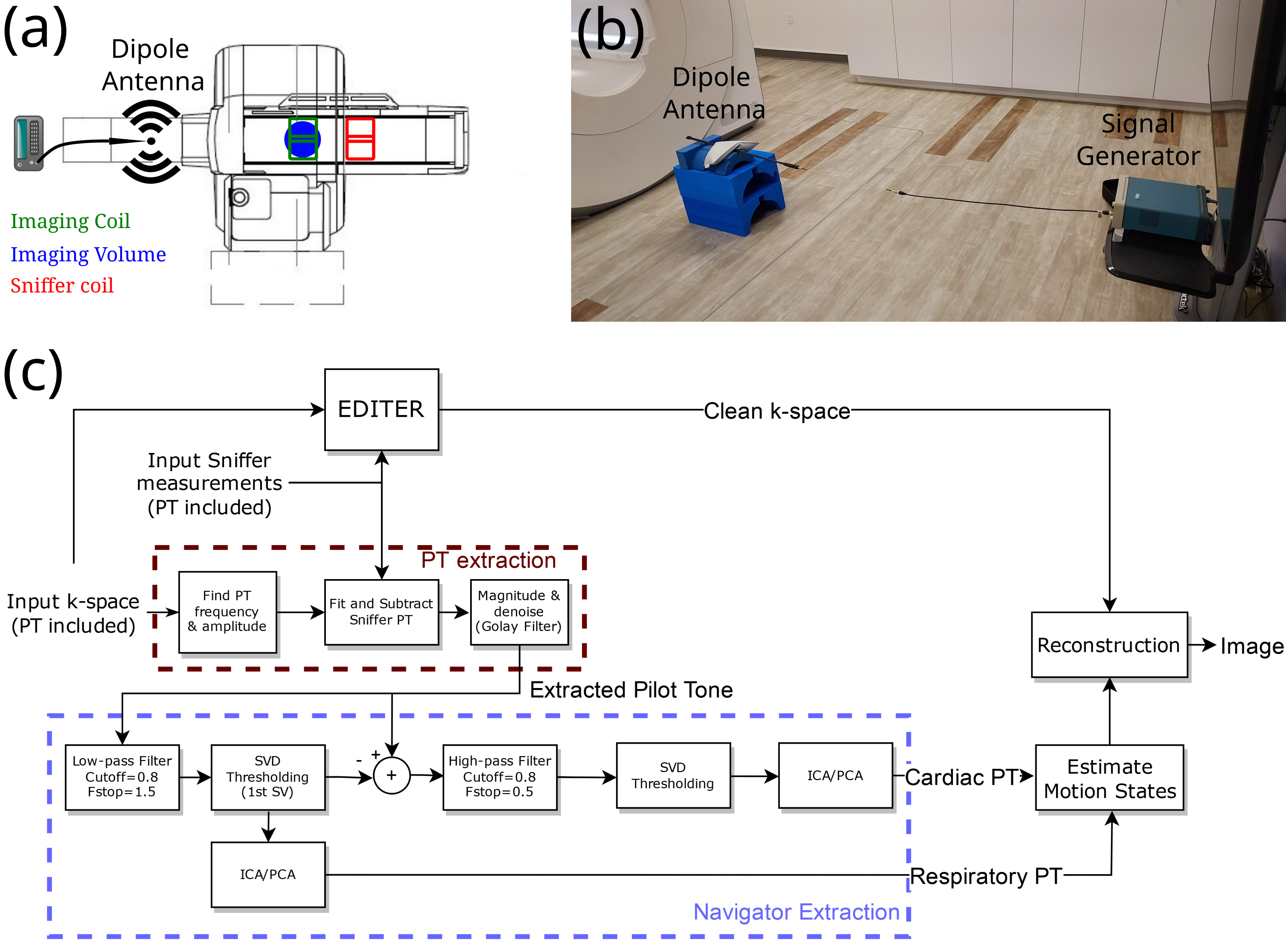
Figure1: (a) Sketch of the placement of signal generator and sniffer coils for the pilot tone experiment. (b) An image of the actual experiment setup. (c) Pilot tone reconstruction and EDITER correction pipeline.
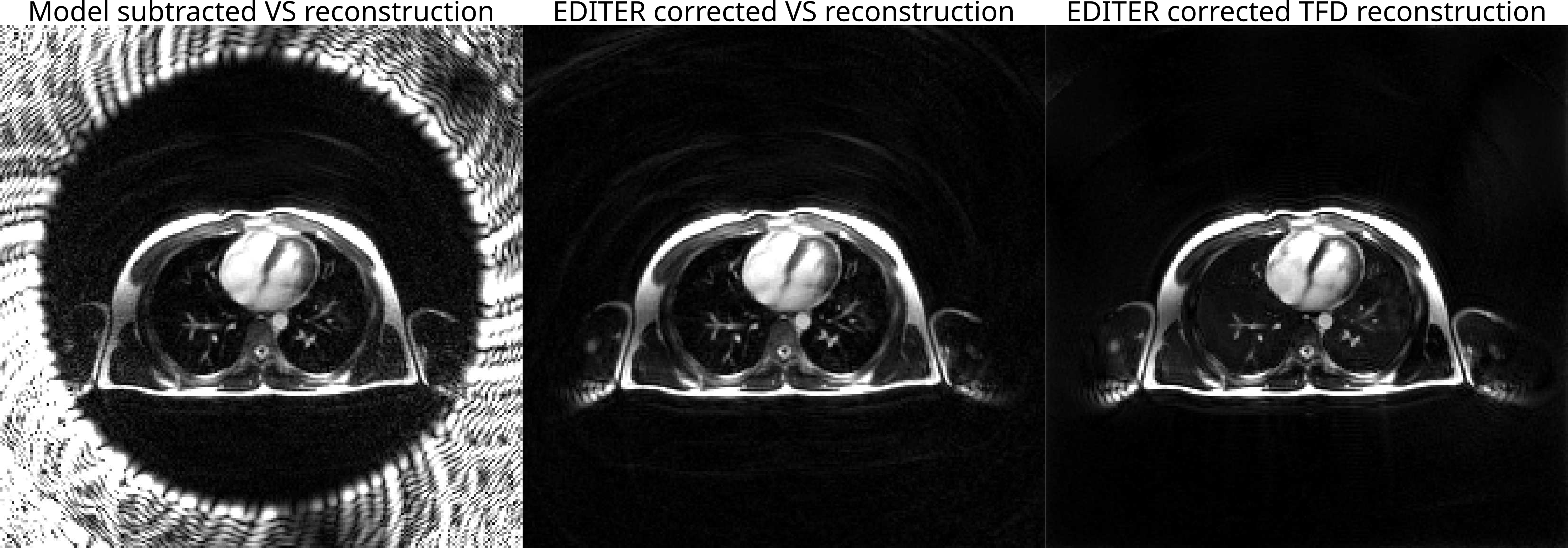
Figure 2: A still frame from real-time movies demonstrating the effect of high amplitude Pilot Tone, and its effective mitigation with EDITER in combination with a constrained reconstruction. The images show from left to right; view-sharing reconstruction with 374ms temporal resolution with only PT subtraction, same view-sharing reconstruction with EDITER
correction,
and an EDITER corrected temporal finite difference constrained
reconstruction with a temporal resolution of 88.4ms.
Figure 3: Comparison of Pilot Tone navigators with ECG for cardiac PT navigator and liver dome displacement with respiratory PT navigator. Liver dome displacement is estimated from real-time images using a line plot across the fat above the liver dome. The region used for line plot is shown with a red dashed line on the image. Both cardiac and respiratory PT show excellent match with the reference methods.
Figure 4: XD-GRASP reconstructed images. Binning into respiratory and cardiac phases are done using PT navigators. (a) shows respiratory motion at systolic phase. The motion of the chest wall (A-P) and vessels (S-I) can be observed. (b) shows one cardiac cycle at end inhalation. The cardiac motion and the contrast change in the vessels can be seen.