0271
Motion-Corrected Subspace Navigator Reconstruction for High Resolution Spiral First-pass Myocardial Perfusion Imaging at 3 Tesla1Cardiovascular medicine, Stanford University, Palo Alto, CA, United States
Synopsis
Keywords: Myocardium, Cardiovascular, Myocardial Perfusion Imaging
Motivation: As perfusion images are typically acquired over 60 heart beats, respiratory motion is unavoidable. Motion compromises spatio-temporal reconstructions.
Goal(s): Residual undersampling artifacts and contrast variation make deformation field estimation challenging. This work aims to get an accurate deformation field from the auxiliary reconstruction and incorporate it into the forward reconstruction model to improve perfusion images.
Approach: To obtain high-quality images for motion estimation, the fixed-angle spiral navigator is used to extract temporal basis. The rigid and non-rigid motion corrections are jointly incorporated into the subspace reconstruction.
Results: Motion-corrected whole-heart first-pass spiral myocardial perfusion imaging with a high resolution of 1.3 mm2 is achieved.
Impact: The proposed navigator-guided subspace motion correction reconstruction pipeline substantially improves the image quality, sharpness, and alignment of the 1.3mm² high-resolution spiral myocardial perfusion imaging, benefiting voxel-wise perfusion quantification crucial for assessing ischemic heart disease.
Introduction
High-quality whole heart first-pass myocardial perfusion imaging can be achieved by using four 5 ms spiral interleaves acquisition1,2 and L1-SENSE reconstruction3. However, respiratory motion due to poor breath-holding will blur the images. Incorporating deformation fields determined from an auxiliary reconstruction into the final reconstruction could mitigate this motion blurring4. Subspace reconstructions can produce high quality images for the highly-undersampled datasets by incorporating informative temporal priors5,6. Respiratory motion can only be partially mitigated by rigid registration7, but residual motion can only be reasonably compensated by non-rigid registration8. To address the motion issues, the rigid motion information and the non-rigid deformation field from axillary reconstructions are jointly incorporated into the k-space and the forward model of subspace reconstruction respectively. This work aims to obtain motion-corrected high-quality images for high-resolution whole heart spiral perfusion imaging by optimizing the spiral acquisitions, extracting temporal basis from fixed navigators, and jointly incorporating rigid and non-rigid motion corrections into the subspace reconstruction.Methods
Acquisition: Images were obtained from 5 subjects undergoing clinical CMR studies on a 3T Siemens scanner. Seven spiral interleaves with 3 ms readouts were rotating contentiously by the golden angle along time. To obtain the temporal basis, one additional fixed-angle navigator spiral interleave is acquired. The acquisition parameters were: resolution=1.3×1.3mm2, slice thickness=10mm, TR=6ms, temporal footprint=90ms, saturation time=60, FA=35. Whole-heart spiral perfusion with 6 slices was acquired using a slice-interleaved acquisition.Reconstruction pipeline: Figure 1 shows the motion correction (MOCO) reconstruction pipeline. Firstly, the temporal basis is extracted from the navigators. Images with motion are reconstructed using subspace reconstruction. Secondly, the reconstructed images were registered using pairwise translation registration centered on the automatically selected heart region. The estimated rigid motion is corrected in k-space. Next, the new temporal basis is extracted from the corrected navigator and applied in the second reconstruction. Then, a multi-scale pairwise non-rigid registration is applied to the rigid-motion corrected images for deformation field estimation. Finally, the rigid-motion corrected images are wrapped and then used to estimate the temporal basis without motion. The final temporal basis and the deformation field are both incorporated into the forward model of the final subspace reconstruction.
Analysis: Images were reconstructed with the proposed joint rigid and nonrigid motion-corrected subspace reconstruction. The L1-SENSE reconstruction was used for comparison and motion corrections were incorporated following the same pipeline. The estimated rigid and non-rigid motion from subspace and L1-SENSE reconstruction pipelines were also incorporated into SENSE reconstruction to assess the temporal fidelity. Retrospective undersampling of breath-hold failure dataset was used to compare the performance of different algorithms. For a fair comparison, the subspace reconstruction of 7 interleaves and 1 navigator (7+1) trajectory was compared to the L1-SENSE reconstruction of 8 continuous k-t rotating trajectory. Perspective reconstructed images were compared visually on a 5-point scale (1 poor to 5 excellent) by a cardiologist. The temporal fidelity of the reconstructions was assessed in the ventricular cavities.
Results
Figure 2 demonstrates the higher performance of the subspace reconstruction with (7+1) interleaves over the L1-SENSE reconstructions with 8 rotating-interleaves in the retrospective undersampling breath-hold failure dataset. Visually, the subspace reconstructions have less motion blurring and lower differences with reference. The high SSIM and low RMSE of the subspace reconstruction demonstrate the high consistency with the ground truth over the L1-SENSE reconstructions.Figure 3 shows the advantages of the subspace reconstruction pipeline over the L1-SENSE reconstruction pipeline with less deformation distortion and better recovery of fine tissue structures.
Figure 4 demonstrates the excellent alignment of the subspace and L1-SENSE MOCO reconstruction in datasets with significant respiratory motion. The aligned SENSE reconstructions demonstrate the accuracy of motion estimation. The reduced blurring of the projected subspace reconstruction would suggest a better alignment over the L1-SENSE reconstruction.
Figure 5 shows the high temporal fidelity of subspace and L1-SENSE motion correction pipelines in the ventricles when compared with the SENSE motion correction reconstructions in both pipelines.
The visual scores for the SENSE-MOCO (L1-SENSE pipeline), SENSE-MOCO (subspace pipeline), L1-SENSE-MOCO and subspace-MOCO were 2.0 ± 0.0, 2.0 ± 0.0, 3.2 ± 0.3 and 4.0 ± 0.5, respectively.
Discussion and Conclusion
Motion-corrected whole-heart first-pass myocardial perfusion imaging with a high resolution of 1.3 mm2 could be achieved by optimizing the navigator-guided k-t golden angle rotating spiral acquisition and jointly incorporating rigid and non-rigid motion correction into the subspace reconstruction. Substantially improved image quality, sharpness and alignment compared with SENSE and L1-SENSE reconstructions could be achieved using the proposed subspace motion correction reconstruction pipeline, which will further benefit voxel-wise perfusion quantification.Acknowledgements
This work is supported by R01 HL131919-01A1 and R01 HL155962-01.References
1. Wang J, Yang Y, Weller DS, et al. High spatial resolution spiral first-pass myocardial perfusion imaging with whole-heart coverage at 3 T. Magnetic Resonance in Medicine 2021;86:648–662.
2. Yang Y, Kramer CM, Shaw PW, Meyer CH, Salerno M. First-pass myocardial perfusion imaging with whole-heart coverage using L1- SPIRiT accelerated variable density spiral trajectories: whole heart spiral myocardial perfusion imaging. Magnetic Resonance in Medicine 2016;76:1375- 1387.
3. Otazo R, Kim D, Axel L, Sodickson DK. Combination of compressed sensing and parallel imaging for highly accelerated first-pass cardiac perfusion MRI. Magnetic Resonance in Medicine 2010;64:767–776.
4. Hoh T, Vishnevskiy V, Polacin M, Manka R, Fuetterer M, Kozerke S. Free-breathing motion-informed locally low‐rank quantitative 3D myocardial perfusion imaging. Magnetic Resonance in Medicine 2022 ;88(4):1575-91.
5. Zhao B, Setsompop K, Adalsteinsson E, Gagoski B, Ye H, Ma D, Jiang Y, Ellen Grant P, Griswold MA, Wald LL. Improved magnetic resonance fingerprinting reconstruction with low‐rank and subspace modeling. Magnetic Resonance in Medicine 2018;79(2):933-42.
6. Cao X, Liao C, Iyer SS, Wang Z, Zhou Z, Dai E, Liberman G, Dong Z, Gong T, He H, Zhong J. Optimized multi‐axis spiral projection MR fingerprinting with subspace reconstruction for rapid whole‐brain high‐isotropic‐resolution quantitative imaging. Magnetic Resonance in Medicine 2022;88(1):133-50.
7. Zhou R, Huang W, Yang Y, Chen X, Weller DS, Kramer CM, Kozerke S, Salerno M. Simple motion correction strategy reduces respiratory-induced motion artifacts for kt accelerated and compressed-sensing cardiovascular magnetic resonance perfusion imaging. Journal of Cardiovascular Magnetic Resonance 2018;20:1-3.
8. Scannell CM, Villa AD, Lee J, Breeuwer M, Chiribiri A. Robust non-rigid motion compensation of free-breathing myocardial perfusion MRI data. IEEE Transactions on Medical Imaging 2019;38(8):1812-20.
Figures
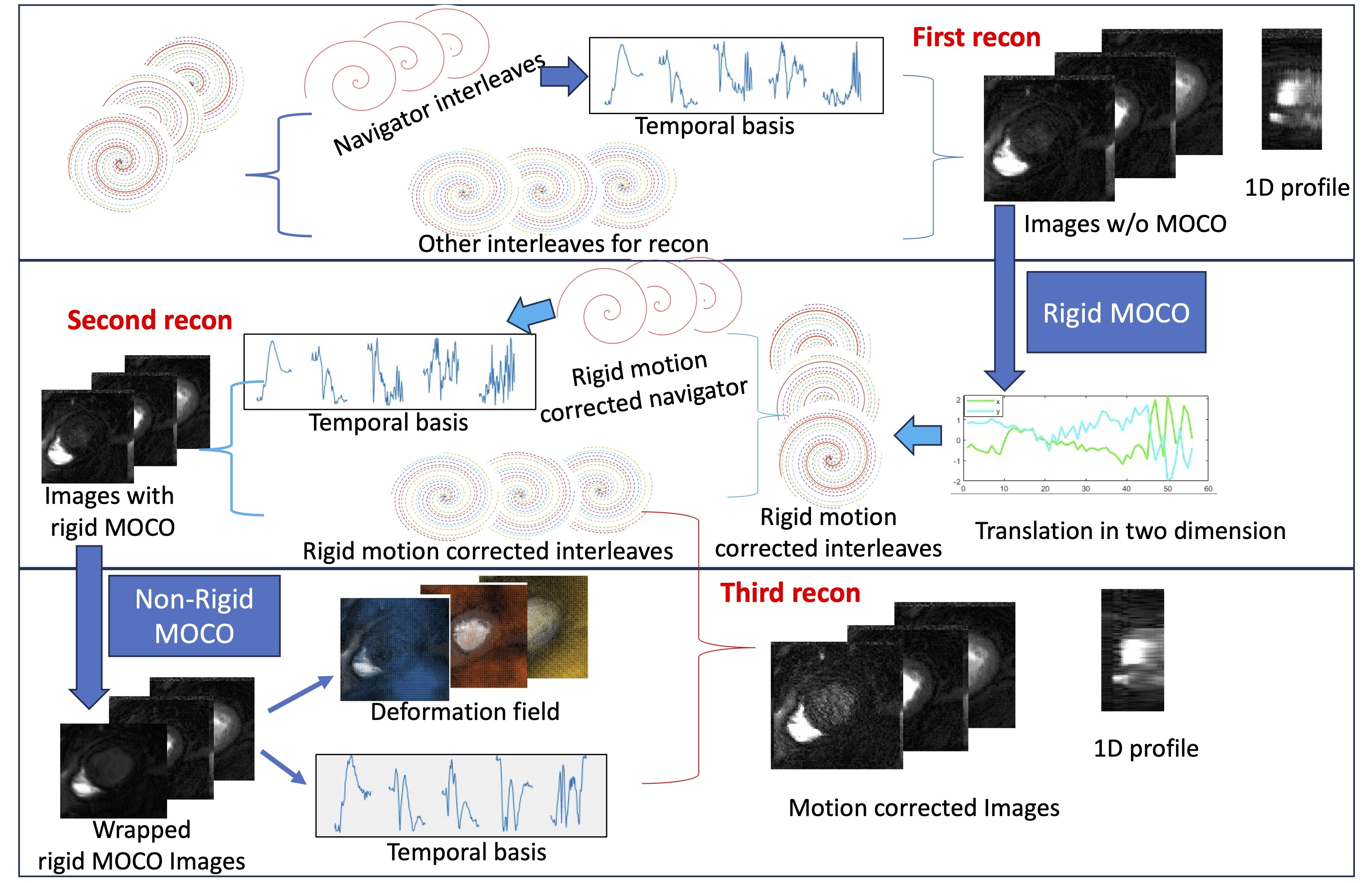
Figure 1 shows the navigator-guided motion-corrected subspace reconstruction pipeline. The pipeline includes 3 steps. Firstly, the temporal basis was extracted from navigators and combined with the left 7 interleaves for the first subspace reconstruction. Secondly, the estimated rigid motion was applied to the k-space. A new temporal basis was extracted for the second reconstruction. Thirdly, the estimated deformation field from rigid MOCO images and temporal basis estimation from wrapped images were both incorporated in the forward model of the last reconstruction.
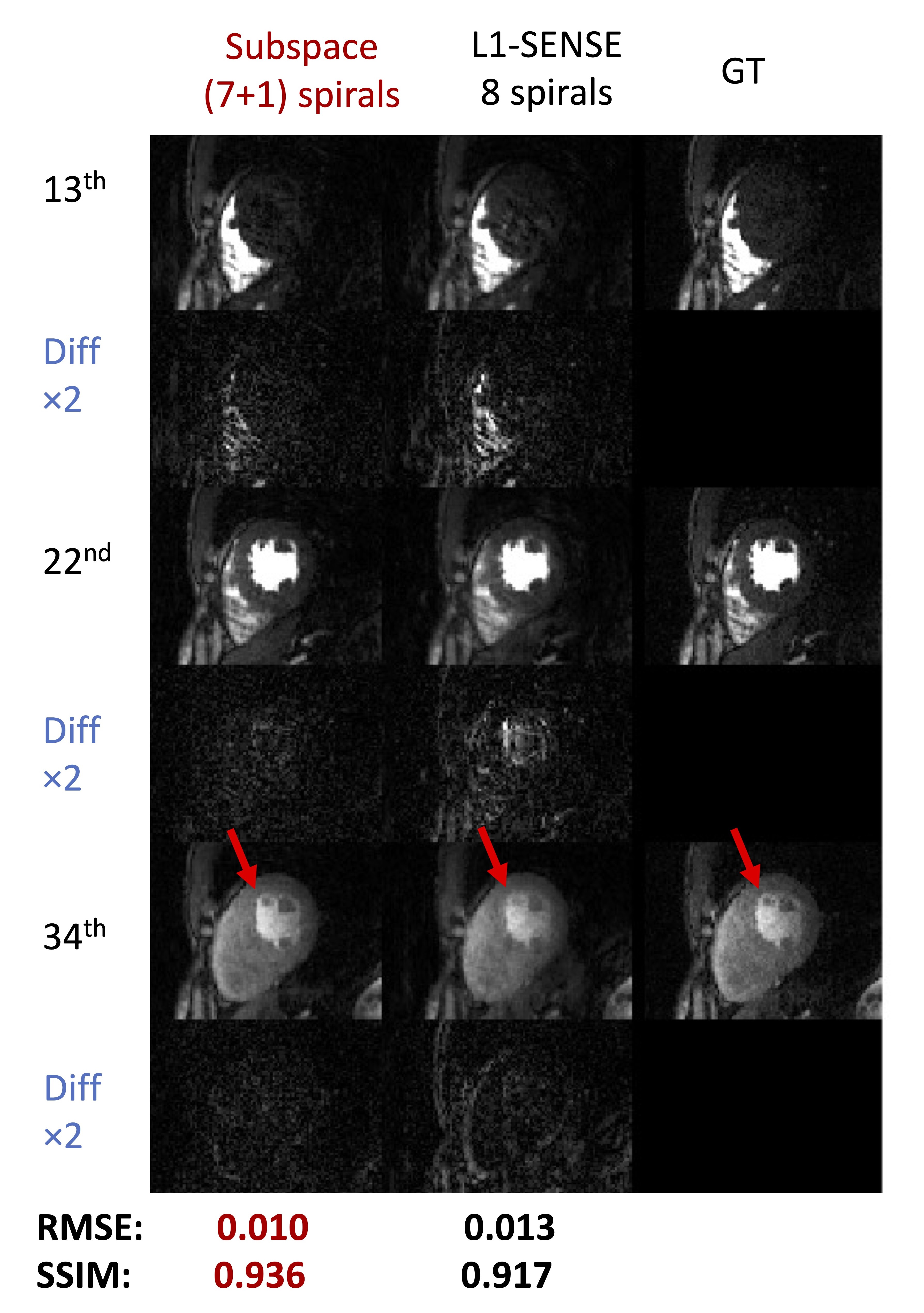
Figure 2 shows the high consistency of subspace reconstruction using the 7 k-t continuous rotating interleaves with 1 navigator trajectory with ground truth in the retrospective undersampling breath-hold failure dataset. L1-SENSE reconstruction was applied on 8 k-t continuous rotating interleaves trajectory for comparison. The difference map shows lower intensity in the result of subspace reconstruction. The red arrows show the blurring in the L1-SENSE reconstruction. The RMSE and SSIM are list below.
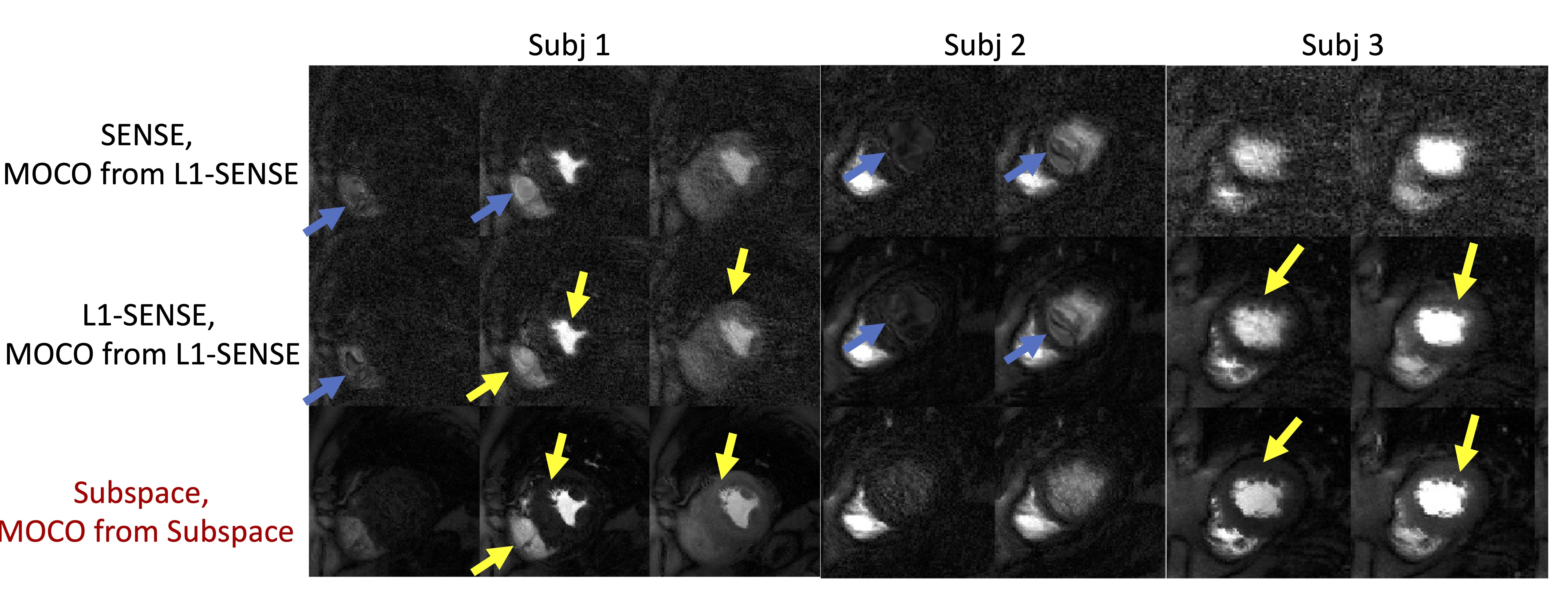
Figure 3 shows the mere deformation distortion and reduced blurring of subspace reconstruction over the L1-SENSE reconstruction and SENSE reconstruction in 3 datasets. The blue arrows show the deformation distortion in the SENSE and L1-SENSE MOCO reconstructions (motion information from the L1-SENSE pipeline). The yellow arrows show the good recovery of slight tissues in the subspace MOCO pipeline and the blurring in the L1-SENSE MOCO pipeline.
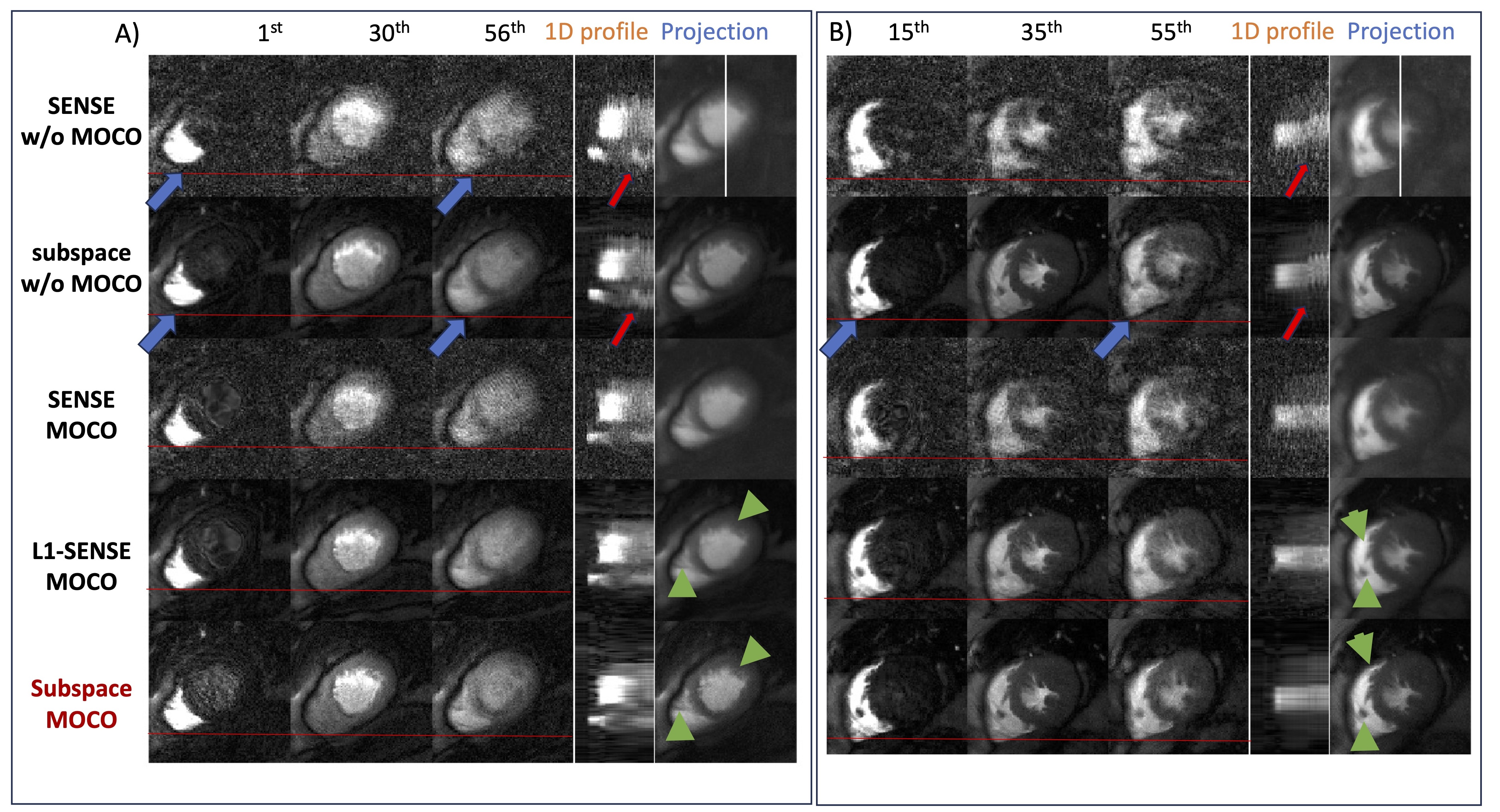
Figure 4 shows the alignment of subspace and L1-SENSE MOCO pipelines by comparing images at different time frames, the 1D profile, and the temporal projection images. The red lines are used as the reference and the blue arrows show the deviation from the baseline in the reconstructions without motion correction. The red arrows show the motion in the temporal 1D profile. The position of the 1D profile line is the white line in the SENSE w/o MOCO projection image. The green arrows show the reduced blurring in the subspace projection image when compared to the L1-SENSE projection image.
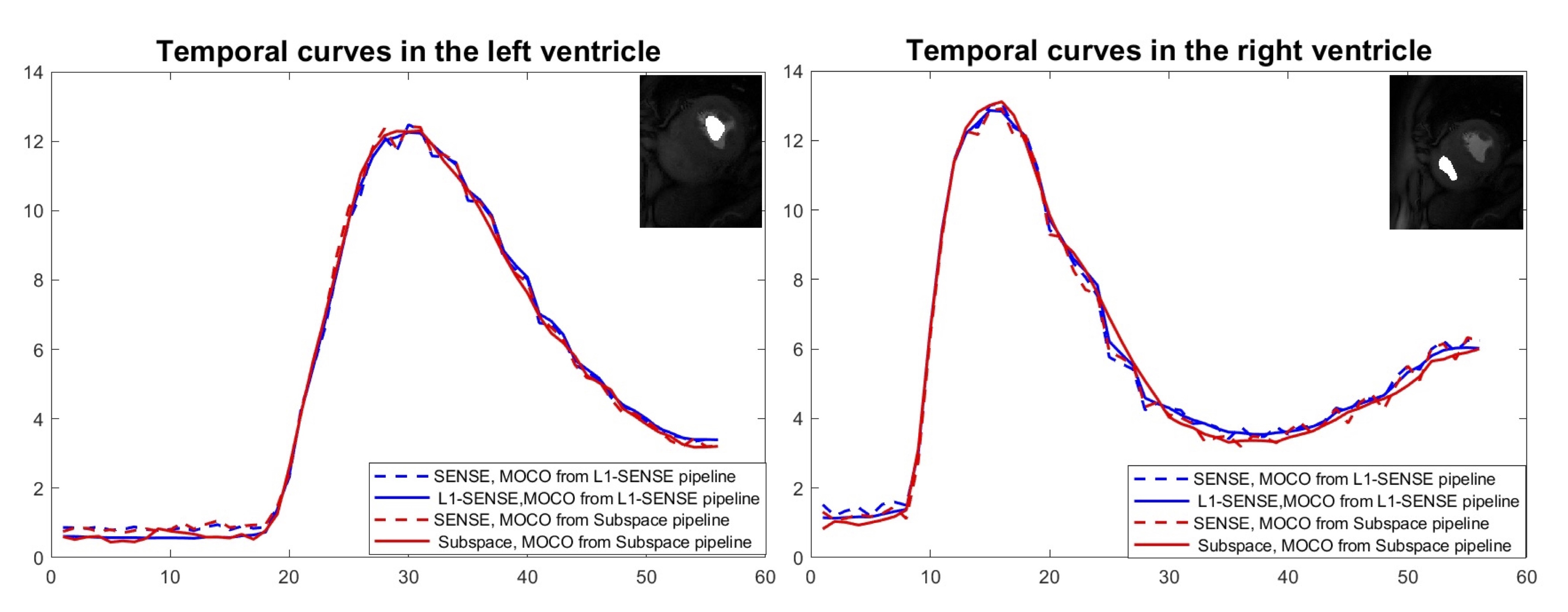
Figure 5 shows the high temporal fidelity of the subspace MOCO reconstruction and L1-SENSE MOCO reconstruction compared to the SENSE MOCO reconstruction in both pipelines. The red solid and dash lines refer to the temporal curves of subspace and SENSE reconstruction in the subspace pipeline, respectively. The blue solid and dash lines refer to the temporal curves of L1-SENSE and SENSE reconstruction in the L1-SENSE pipeline, respectively. The masks of the left and right ventricles are shown in the right upper corners.