0268
Investigating Quantitative Perfusion Characteristics of Prostate Cancer for African American and White Men1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Radiology, The First Affiliated Hospital of China Medical University, Shenyang City, China, 3Radiology, University of Alabama at Birmingham, Birmingham, AL, United States, 4Urology, University of California, Los Angeles, CA, United States
Synopsis
Keywords: Prostate, Prostate, Health disparity, perfusion analysis
Motivation: Race and ethnicity strongly impact the risk of prostate cancer, and understanding the impact of biological heterogeneity in patients from different racial/ethnic backgrounds is crucial for reducing the observed gaps in clinical outcomes.
Goal(s): To investigate potential differences in quantitative perfusion characteristics of prostate cancer between African American and White men.
Approach: After matching commonly known clinical risk factors, the quantitative DCE-MRI analysis was performed to assess differences in perfusion parameters of the pathology- and MRI-based lesions African American and White men.
Results: Notable differences between the two cohorts were observed in the Ktrans of tumors with csPCa.
Impact: Considering race-specific perfusion characteristics can help in understanding biological factors of health disparity in prostate cancer.
Introduction
African American (AA) men have been shown to have a higher likelihood of PCa-related death than White (W) men. Although socioeconomic factors and healthcare access may account for the difference [1], there exists a growing body of literature showing that genetic and biological factors may be equally implicated in these discrepancies [2,3]. As such, understanding the impact of biological heterogeneity in patients from different racial/ethnic backgrounds is crucial to further reducing health disparity in prostate cancer.Multi-parametric MRI (mpMRI) is a non-invasive imaging tool for detecting high-grade and larger tumors and allows for exploring the biological and molecular characteristics of PCa. In particular, dynamic contrast-enhanced (DCE) MRI, as part of mpMRI, measures microvascular perfusion by quantitatively characterizing contrast uptakes of dynamic MRI signals [refs]. Increased perfusion is associated with a higher grade of PCa, requiring more aggressive management. Differences in quantitative DCE-MRI (qDCE) parameters can potentially explain the biological differences noted among AA and W men and ultimately improve the characterization of clinically significant PCa (csPCa) in patients with different ethnic backgrounds when correctly accounted for the interpretation of mpMRI [4,5]. In this study, we aimed to retrospectively investigate the performance of 3T mpMRI and assess differences in quantitative perfusion parameters of the pathology- and MRI-based lesions between AA and W men who underwent 3T mpMRI before radical prostatectomy.
Methods
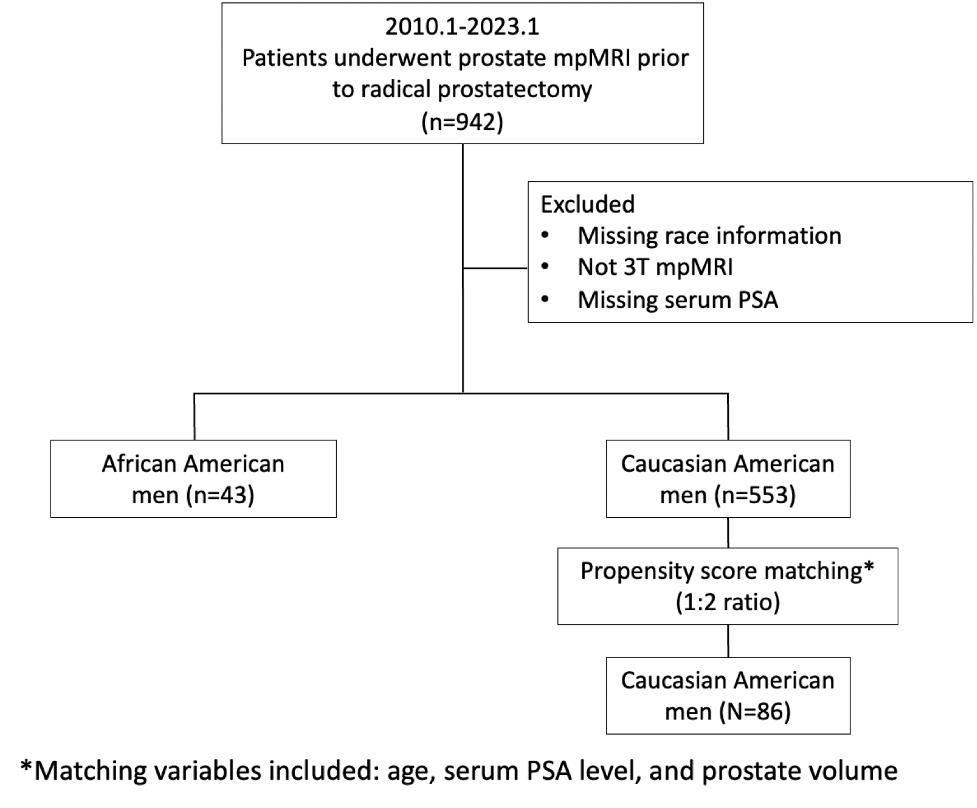
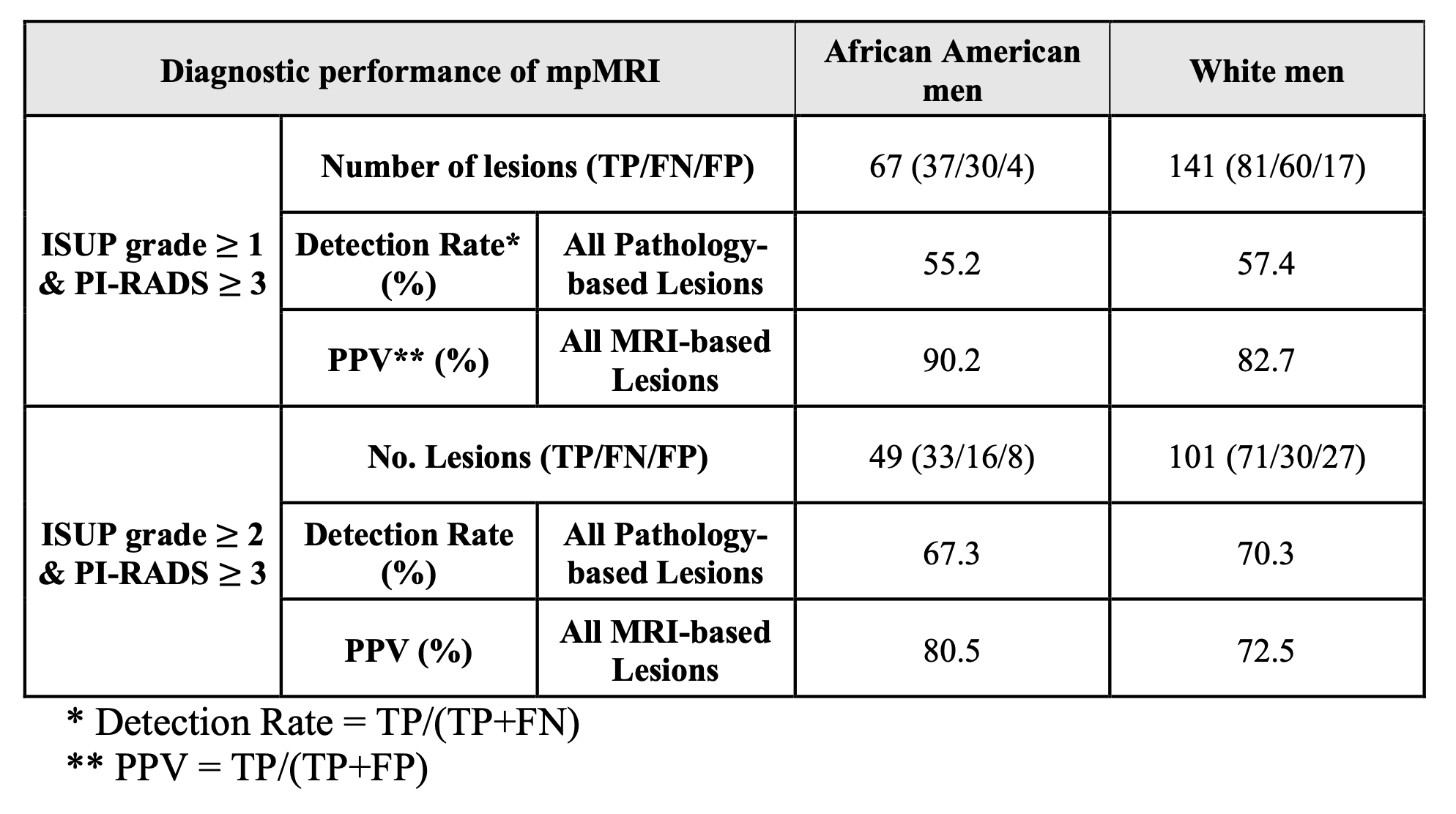
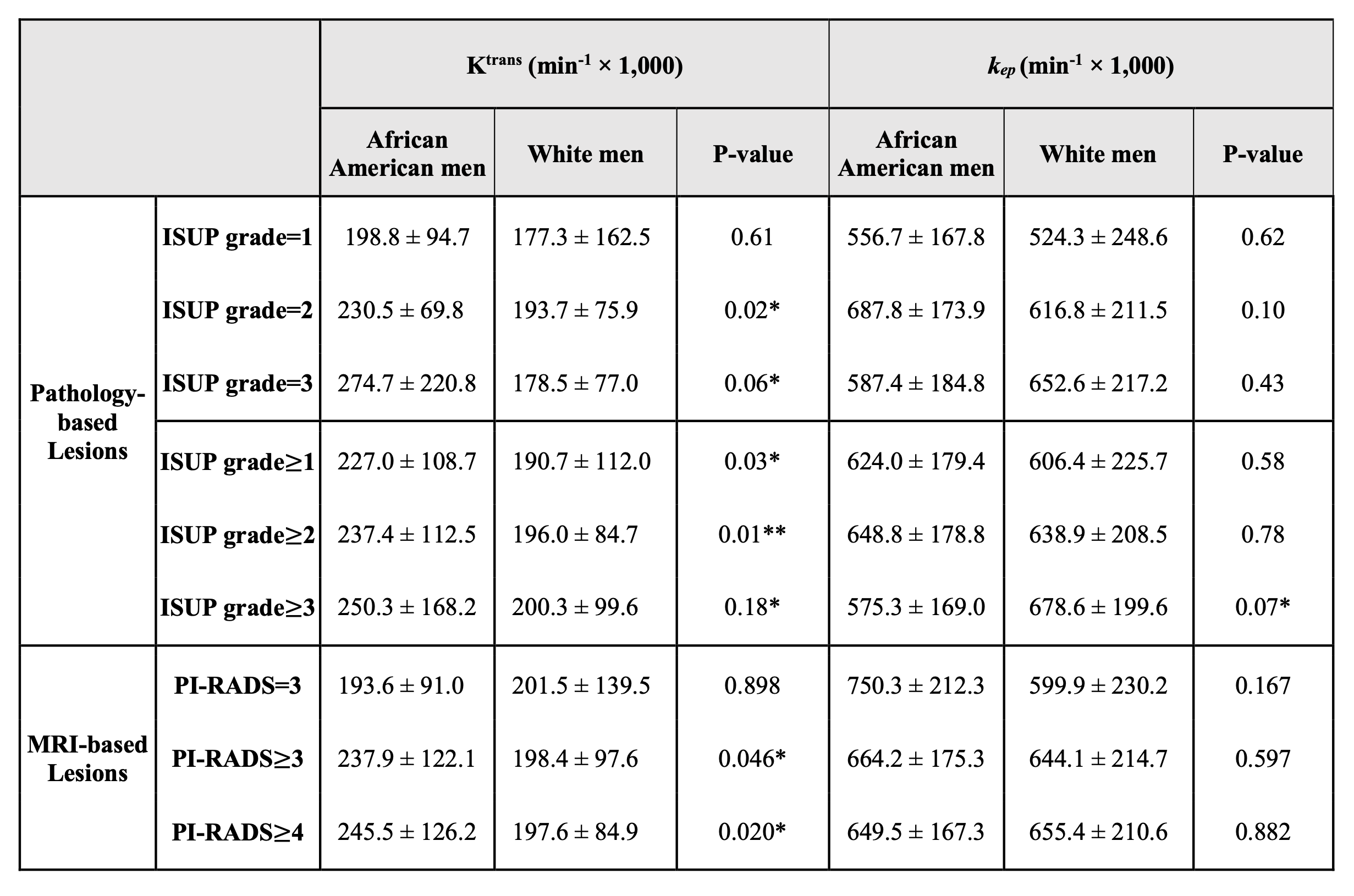
This single institutional retrospective HIPAA-compliant study was approved by our institutional review board (IRB). We had an initial study cohort of 942 consecutive patients who underwent mpMRI prior to prostatectomy from 2010 to 2023. All preoperative mpMRIs were interpreted by an abdominal imaging fellow and then reviewed by one of three board-certified attending radiologists with 5-20 years of experience. PI-RADS v2.1 guidelines were used to interpret all mpMRI scans.We applied the propensity score caliper matching algorithm to minimize the bias between AA and W men in a 1:2 ratio with the covariates (Figure 1), including patient age, PSA, and prostate volume, which are known to be associated with the risk factors for PCa diagnosis [9,14]. An MRI-positive and pathology-positive lesion was labeled as true positive (TP). An MRI-positive but pathology-negative lesion was labeled as false positive (FP), while an MRI-negative but pathology-positive lesion was labeled as false negative (FN). The per-lesion diagnostic performance of mpMRI was characterized by calculating cancer prevalence, detection rates (DR=TP/(TP+FN), and positive predictive values PPV=TP/(TP+FP)) between matched CA and AA men. Quantitative DCE-MRI analysis blinded to race/ethnicity, using a lab-made software package with MATLAB (MathWorks, Natick, MA), compliant with the Quantitative Imaging Biomarkers Alliance (QIBA) DCE-MRI quantitation profile [6]. The standard Tofts model was used to estimate Ktrans (volume transfer constant; min-1) and kep (blood influx rate; min-1) [15,16]. Ktrans and kep values were averaged over a lesion annotation, and the average Ktrans and kep were used to assess differences in perfusion characteristics between matched AA and W men for the pathology- and MRI-based lesions. The Mann-Whitney U test was used to analyze continuous variables.
Results and Discussion
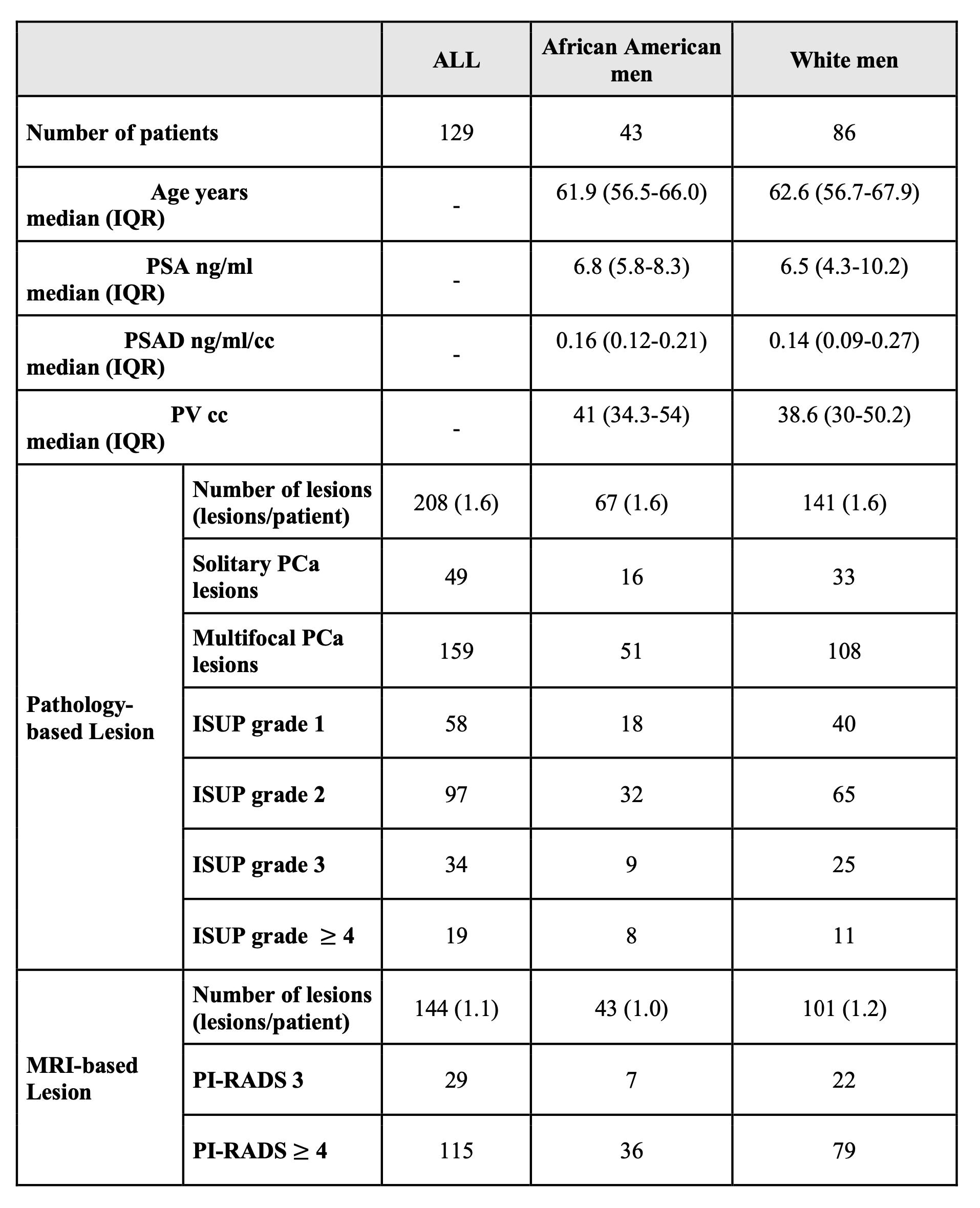
A total of 129 patients were identified for the matched study cohort (43/86 for AA/W men). Table 1 shows the patient and lesion characteristics between matched AA and W men. Diagnostic performances of mpMRI for detecting PCa lesions are summarized in Table 2. Quantitative DCE-MRI parameters in AA and W sub-cohorts are listed in Table 3. Notable differences between the two cohorts were observed in the Ktrans of tumors with ISUP grades 2 and 3 and for tumors with ISUP ≥ 1, 2 and 3 (p<0.05). Additionally, the tumors of AA men had significantly higher Ktrans than the W sub-cohort when the PI-RADS score was ≥ 3 or ≥ 4 (p<0.05). However, kep was not significantly different except for tumors with ISUP ≥ 3 between the two racial groups.The distinct characteristics of Ktrans between AA and W men could reflect biological tumor differences among men from different racial backgrounds, as suggested by several studies investigating genetic/epigenetic factors and the influence of the tumor microenvironment [7]. If present, any race-based parameters that reflect differences in tumor biology should be used to improve diagnosis in AA men, especially when interpreting mpMRI.
Conclusion
Our results demonstrated a significant difference in Ktrans of csPCa (p<0.01) for the pathology- and MRI-based lesions between AA and W cohorts after matching patient age, PSA, and prostate volume between the two groups. Considering race-specific perfusion characteristics can help in understanding biological factors of health disparity in prostate cancer.Acknowledgements
This work was supported by the National Institutes of Health (NIH) R01-CA248506 and R01-CA272702, and funds from the Integrated Diagnostics Program, Departments of Radiological Sciences & Pathology, David Geffen School of Medicine at UCLA.References
[1] Riviere, P. et al. Survival of African American and non-Hispanic white men with prostate cancer in an equal-access health care system. Cancer. 2020;126:1683-1690. doi: 10.1002/cncr.32666
[2] Bhardwaj, A. et al. Racial disparities in prostate cancer: a molecular perspective. Front Biosci (Landmark Ed). 2017;22:772-782. doi: 10.2741/4515
[3] Wallace, T.A. et al. Tumor immunobiological differences in prostate cancer between African-American and European-American men. Cancer Res. 2008;68:927-936. doi: 10.1158/0008-5472.Can-07-2608
[4] Yuan, Q. et al. Quantitative diffusion-weighted imaging and dynamic contrast-enhanced characterization of the index lesion with multiparametric MRI in prostate cancer patients. Journal of magnetic resonance imaging : JMRI. 2016. doi: 10.1002/jmri.25391
[5] Futterer, J.J. et al. Staging prostate cancer with dynamic contrast-enhanced endorectal MR imaging prior to radical prostatectomy: experienced versus less experienced readers. Radiology. 2005;237:541-549. doi: 10.1148/radiol.2372041724
[6] Chao, S.L., Metens, T., Lemort. M. TumourMetrics: a comprehensive clinical solution for the standardization of DCE-MRI analysis in research and routine use. Quant Imaging Med Surg. 2017; 7:496–510. doi: 10.21037/qims.2017.09.02.
[7] Bhardwaj, A. et al. Racial disparities in prostate cancer: a molecular perspective. Front Biosci (Landmark Ed). 2017;22:772-782. doi: 10.2741/4515
Figures