0267
Is MR-visible Gleason 6 prostate cancer clinically insignificant?1Body MRI, Stanford University, Stanford, CA, United States, 2Radiology, Stanford University, Stanford, CA, United States, 3Urology, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Prostate, Prostate
Motivation: The clinical course of MR-visible Gleason 6 prostate cancer is unclear.
Goal(s): We studied patients with MR-visible prostate lesions scored as Gleason 6 after MR-guided and systematic biopsy.
Approach: We retrospectively analyzed the rate of Gleason grade upgrading in 95 men initially diagnosed with Gleason 6 prostate cancer in an MR-visible lesion who later underwent a second biopsy or prostatectomy.
Results: Over half of MR-visible Gleason 6 lesions were upgraded to Gleason 7 with a median time to upgrade of ~2 years. Neither PSA density nor ADC value predicted subsequent upgrade.
Impact: Gleason 6 prostate cancer that is MR-visible often harbors higher grade cancer. This argues for more aggressive monitoring or earlier intervention in these patients.
INTRODUCTION
Men with prostate cancer are stratified into risk categories primarily based on histopathological Gleason scoring, with Grade 7 or above representing more aggressive cancer1,2, typically managed with prostatectomy or radiation. Men with low grade, Gleason 6 cancer are increasingly offered active surveillance (AS) instead of treatment, but half of men in AS progress to treatment within 10 years3. Predicting those destined to progress is an important clinical challenge. We analyzed the clinical course of a cohort of men with MR-visible lesions initially graded as Gleason 6 after MR-guided and systematic biopsy. We hypothesized that men with MR-visible Gleason 6 prostate cancer have a high risk of progression to Gleason 7.METHODS
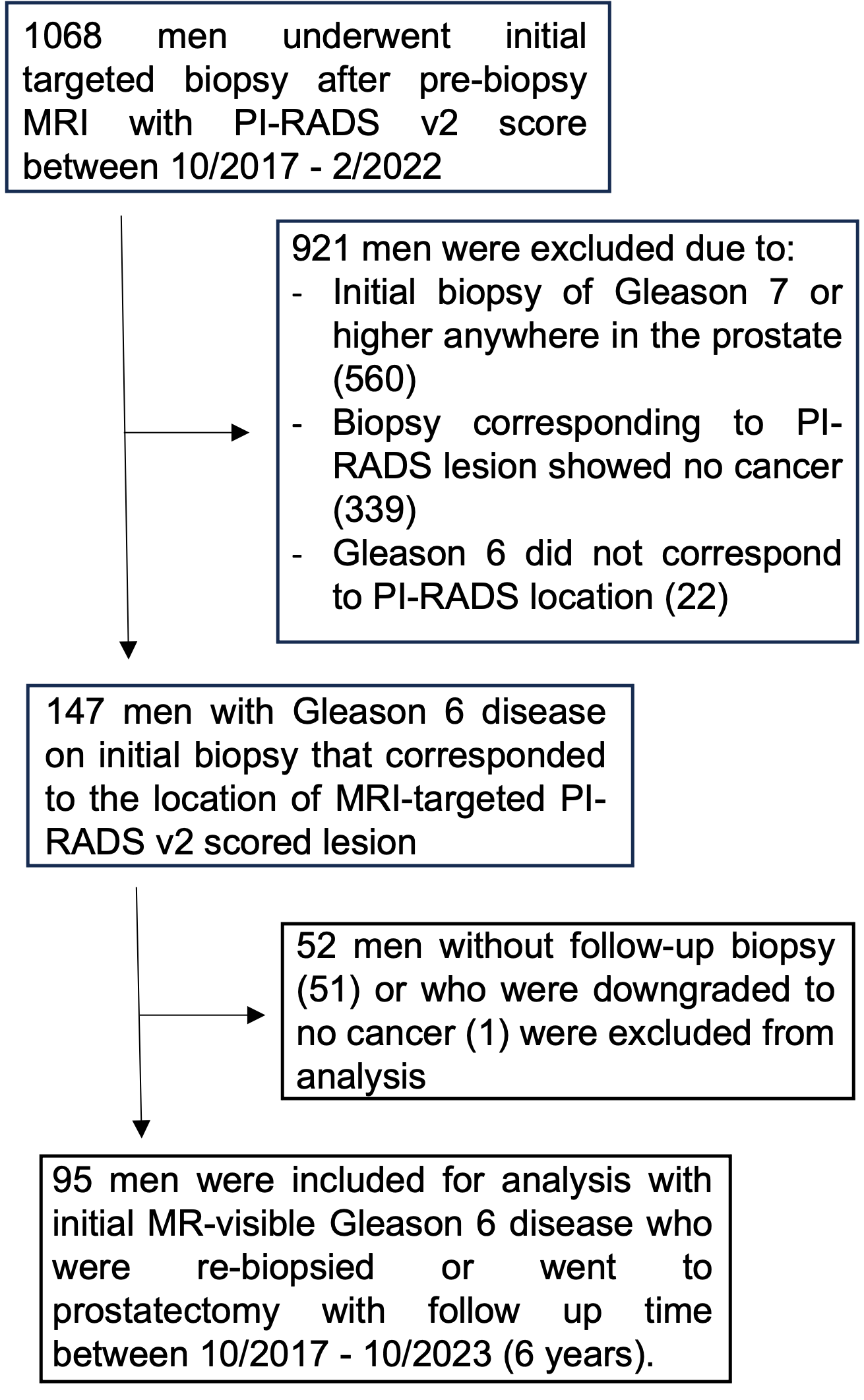
We retrospectively analyzed a cohort of 1068 men who underwent pre-biopsy prostate MRI at our referral center between 10/2017 and 02/2022 (IRB 24850). Men with prostate lesions scored as PIRADS v2 3-5 underwent both MRI-targeted and systematic biopsy. 147 men with MR-visible lesions graded as Gleason 6 on biopsy histopathology, and without higher grade cancer elsewhere in the prostate, were identified. Of those, 95 underwent rebiopsy or prostatectomy during follow-up between 10/2017 and 10/2023 (Figure 1). The primary outcome was upgrading to Gleason ≥7 cancer. Fisher’s exact test was used to compare categorical values. Wilcoxon rank sum test and two tailed t-test were used to compare nonparametric data.RESULTS
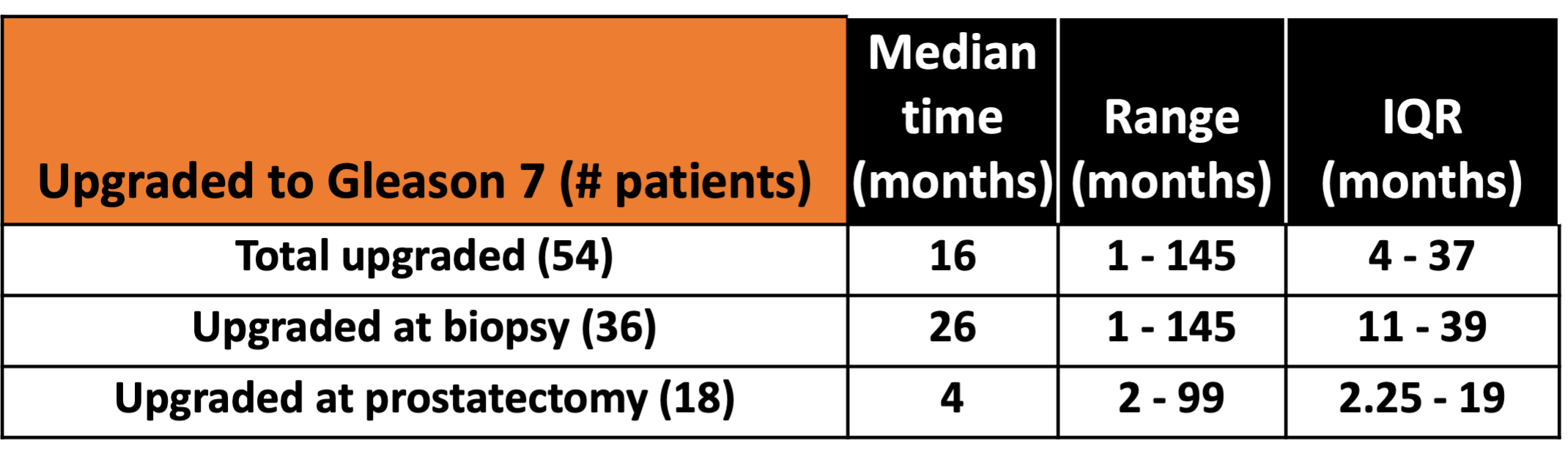
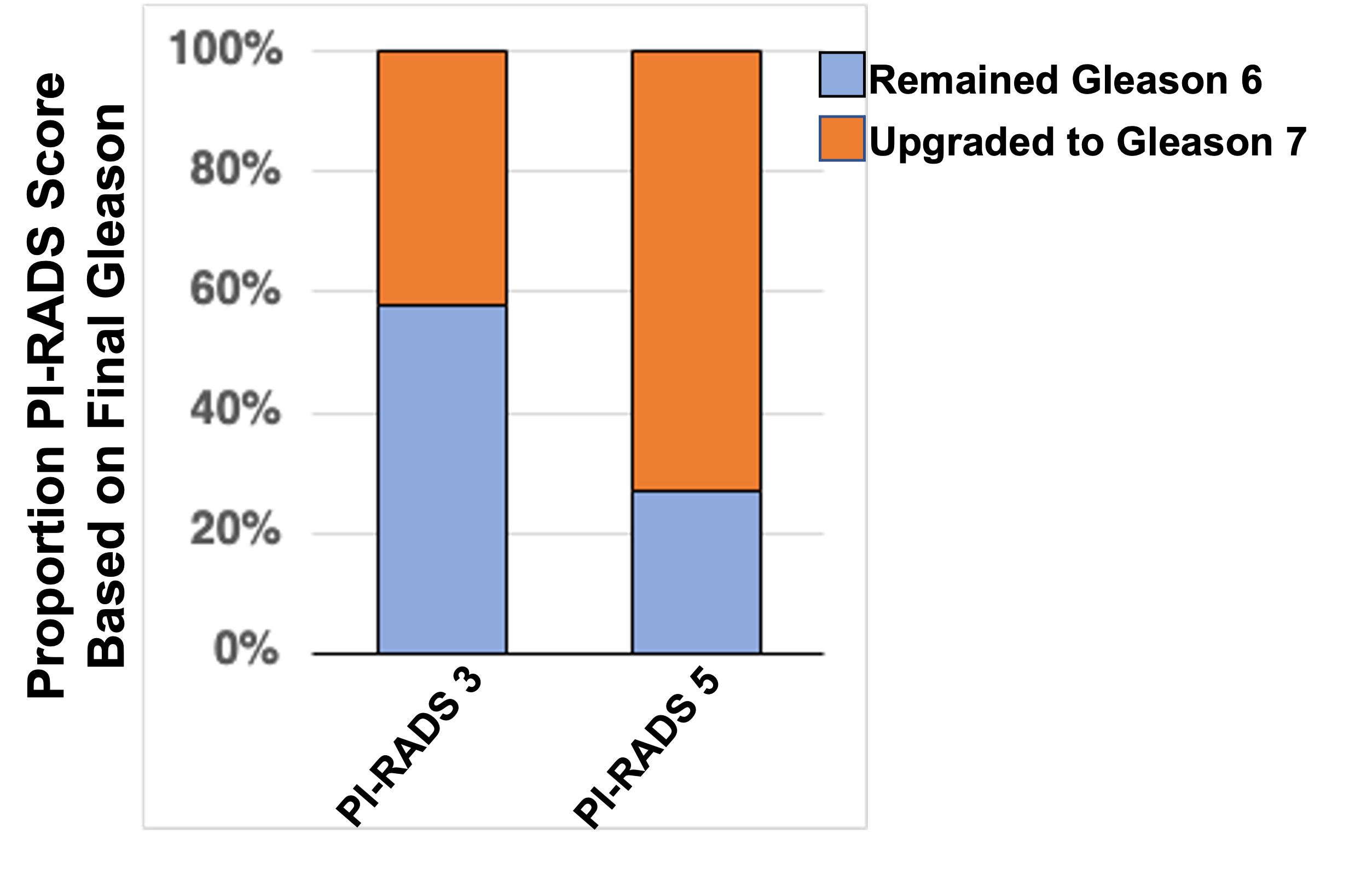
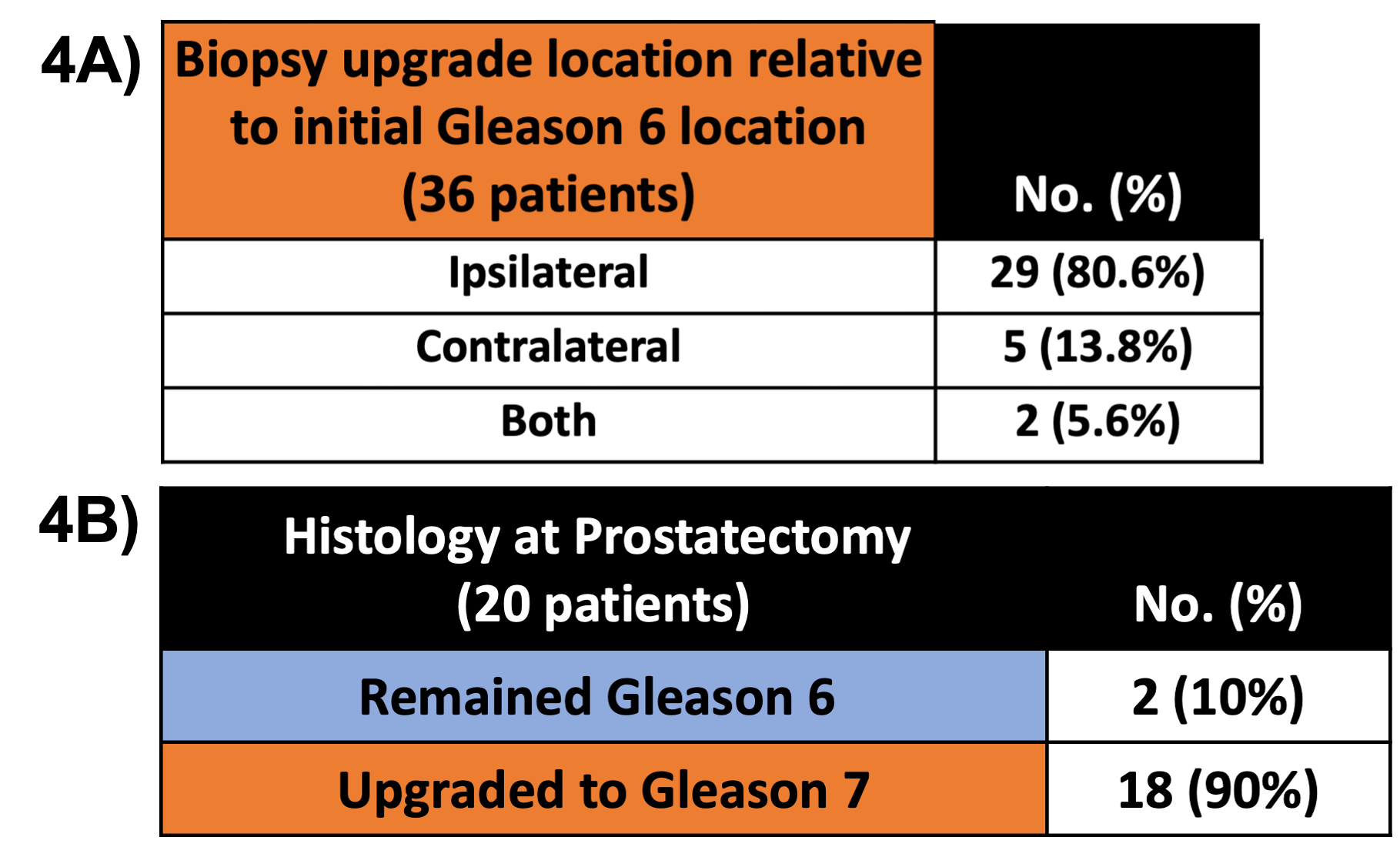
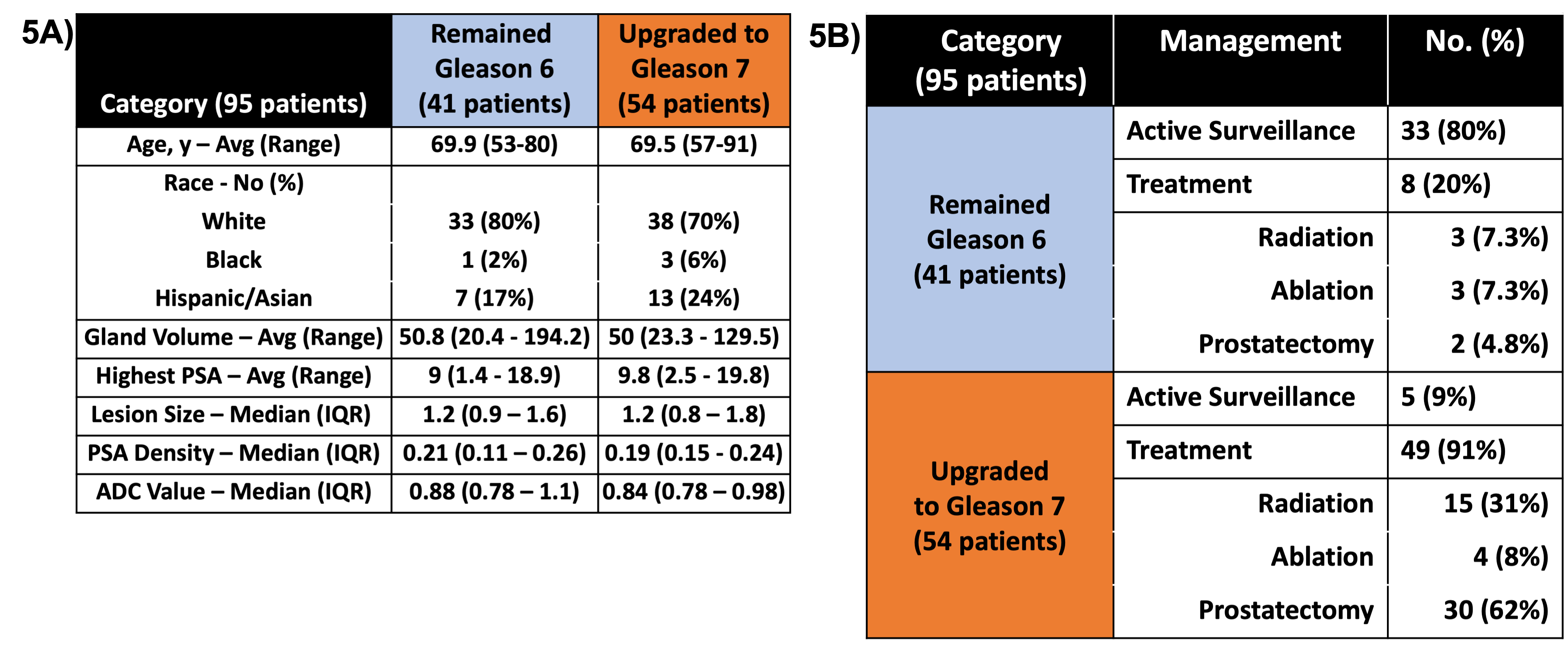
54 of 95 men (57%) initially diagnosed with Gleason 6 prostate cancer were upgraded to Gleason 7 at a median time of 26 months (Figure 2). 73% of Gleason 6 cancers that were reported as PI-RADS 5 lesions on initial MRI were upgraded to Gleason 7 cancer at follow up, compared to 27% of those initially reported as PI-RADS 3 lesions (p=0.047, Figure 3). In 80.6%, Gleason 7 cancer found on subsequent biopsy is ipsilateral to the lesion initially diagnosed as Gleason 6 (Figure 4A). Of 20 men with Gleason 6 cancer who opted for prostatectomy within a median of 4 months after diagnosis, 90% were found to harbor Gleason 7 cancer (Figure 4B). No difference in age, race, gland volume, highest recorded PSA, or lesion volume were identified between men with or without upgrading (Figure 5A). Median PSA density between those who remain Gleason 6 (0.21, IQR 0.11-0.26) and those upgraded to Gleason 7 (0.19, IQR 0.15-0.24) are not statistically different (p=0.704) (Figure 5A). Additionally, ADC values on diffusion weighted imaging between those who remain Gleason 6 (0.88, IQR 0.78 – 1.1) and those upgraded to Gleason 7 (0.84, IQR 0.78 – 0.98) are not statistically different (p = 0.19) (Figure 5A). Once diagnosed with Gleason 7 cancer, patients were more likely to undergo treatment rather than active surveillance (p<0.001, Figure 5B).DISCUSSION
In our cohort, the majority (57%) of men with MR-visible prostate lesions that were initially graded as Gleason 6, harbored Gleason 7 cancer within the gland at radical prostatectomy or were upgraded on subsequent short-term surveillance biopsy. Studies prior to the advent of MRI diagnosis and targeted biopsy showed an upgrade rate to Gleason 7 cancer at prostatectomy of 12-60%4,5. A more recent study utilizing MR-guided and systematic biopsies reported a much lower upgrade rate of 14.4%6. Our higher upgrade rate (57% overall, 90% at prostatectomy) may be due inclusion of a relatively small cohort of men who had a prostatectomy or repeat biopsy. Presumably, these are patients who are at higher risk (e.g. greater cancer volume on biopsy, higher genomic risk score, etc.). However, even if we assume that men diagnosed with MR-visible Gleason 6 cancer who did not get repeat biopsy or prostatectomy still remain Gleason 6, the rate of upgrade remains high (52 of 147 (35%), data not shown). Interestingly, we found no difference between PSA density or ADC value in men that remained Gleason 6 and those that were upgraded to Gleason 7 on subsequent biopsy or at prostatectomy. This is supported by studies that show mixed association between Gleason score and PSA density above a certain threshold5,7,8. Overall, our results demonstrate that many men with initial MR-visible Gleason 6 prostate cancer will either be quickly upgraded and/or already harbor Gleason 7 cancer, which would ultimately prompt a change in their management. These data support continuing to carefully monitor patients with MR-visible Gleason 6 prostate cancer with the expectation that a large fraction will progress to a higher clinically significant cancer grade within a relatively short time frame.Acknowledgements
No acknowledgement found.References
1. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. Gleason DF, Mellinger GT. J Urol. 1974; 111:58–64.
2. A contemporary prostate grading system: a validated alternative to the Gleason score. Epstein J, Zelefsky M, Sjoberg D, Nelson J, et al. J. Uro Euro. 2016. 69(3).
3. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. Hamdy F, Donovan J, Lane A, Mason M et al. New Eng J Med. October 2016; 375.
4. Prostate cancers scored as Gleason 6 on prostate biopsy are frequently Gleason 7 tumors at radical prostatectomy: Implication on outcome. Pinthus J, Witkos M, Fleishner N, Sweet J, Evans A, Jewett M, Krahn M, Alibhai S, Trachtenberg J. The Journal of Urology. 2006. Vol 176; 979-984.
5. Factors predicting Gleason score 6 upgrading at radical prostatectomy. Milonas D, Grybas A, Auskalnis S, Gudinaviciene I, Baltrimavicius R, Kincius M, Jievaltas M. Cent European J Urol. 2011; 64(4) 205-208.
6. MRI-targeted, systematic, and combined biopsy for prostate cancer diagnosis. Ahdoot M, Reese W, Lebastchi A, Mehralivand S, Gomella P, Bloom J, Gurram S, Siddiqui M, Pinsky P, Parnes H, Linehan W, Merino M, Choyke P, Shih J, Turkbey B, Wood B, Pinto P. New Eng J Med. March 2020, 382;10.
7. MRI-Based Prostate-Specific Antigen Density Predicts Gleason Score Upgrade in an Active Surveillance Cohort. Washington S, Baskin A, Ameli N, Nguyen H, Westphalen A, Shinohara K, Carroll P. Am J Roentgenol. 2020. Vol. 214(3).
8. Utility of PSA Density in Predicting Upgraded Gleason Score in Men on Active Surveillance With Negative MRI. Press B, Khajir G, Ghabill K, Leung C, Fan R, Wang N, Leapman M, Sonn Geoffrey, Sprenkle P. J Urology. 2021. Vol 155.
Figures