0262
Assessment of Radiomic Features of Metabolism in Advanced Prostate Cancer using Hyperpolarized 13C MRI with Whole Abdominopelvic Coverage1Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Helen Diller Family Comprehensive Cancer Center, University of California, San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Prostate, Prostate, Hyperpolarized 13C MRI
Motivation: Hyperpolarized (HP) 13C-pyruvate MRI can address limitations of PSMA-PET for monitoring therapy and evaluating treatment-emergent, lethal subtypes of prostate cancer.
Goal(s): To establish and characterize a novel radiomics framework of tumor metabolism in advanced prostate cancer based on whole abdominopelvic HP MRI.
Approach: We extracted 316 metabolic features from 16 patients. Following feature selection and classification, their prognostic values were evaluated using uni- and multivariate survival analyses.
Results: Metabolic feature kPL,median (pyruvate-to-lactate conversion rate) significantly predicted both progression-free (p<0.01) and overall (p<0.05) survivals with longer median PFS (11.2 vs 0.5 months) and OS (NR vs 18.4 months) in the lower- vs higher-kPL subgroups.
Impact: A novel radiomics framework based on whole abdominopelvic hyperpolarized 13C-pyruvate MRI extracted and evaluated 316 metabolic features of advanced prostate cancer. Selected features significantly predicted clinical outcome measures (PFS and OS), strongly supporting further investigation of their prognostic values.
Purpose
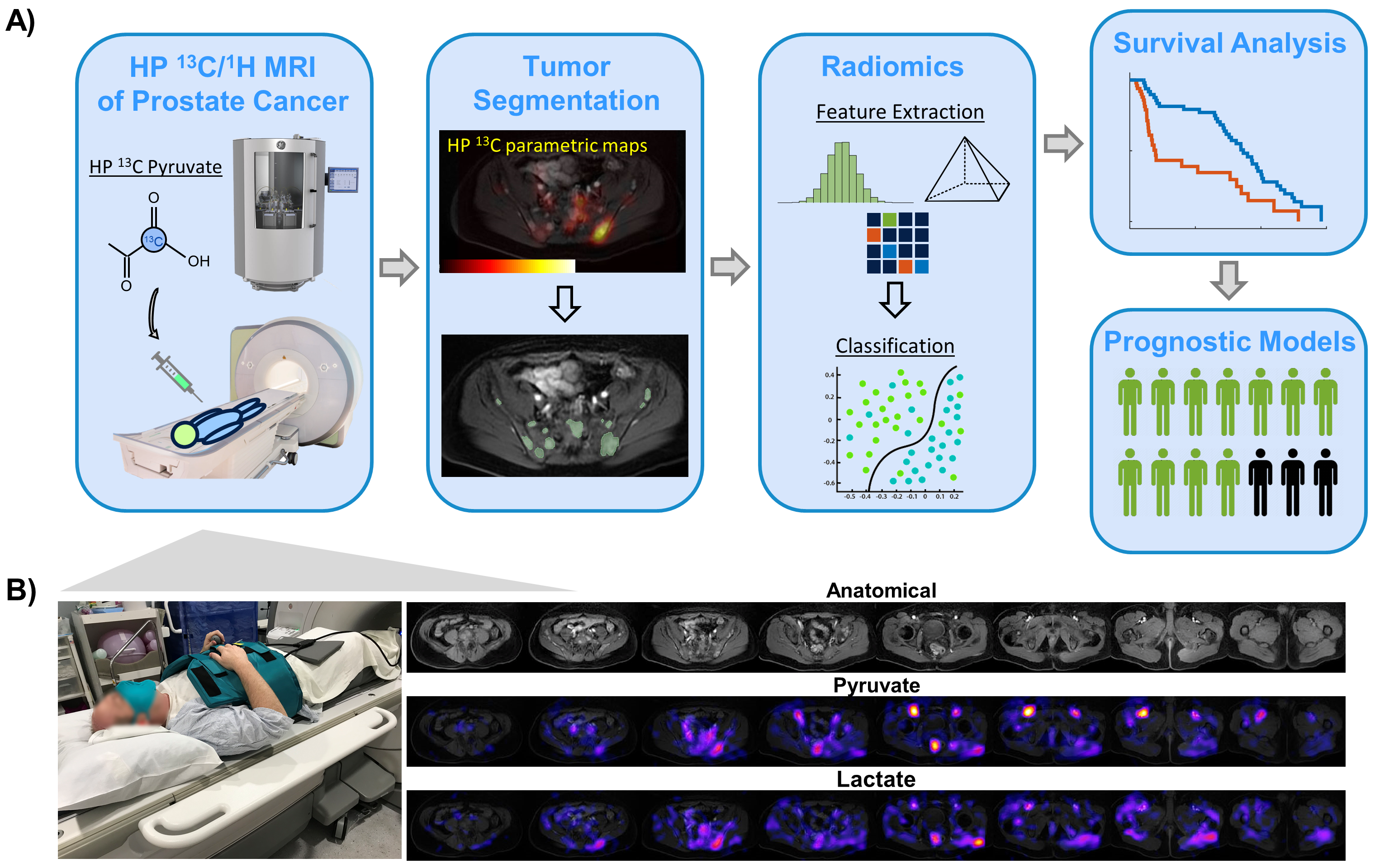
Whereas PSMA-PET is now commonly used in the settings of intermediate- to high-risk localized prostate cancer and biochemical recurrence1-3, it has shown limited utility for response assessment4. Moreover, the small-cell neuroendocrine subtype (NEPC), often arising from prolonged hormone therapy, is hallmarked by downregulation of PSMA expression, yet rapid proliferation and poor prognosis5. Hyperpolarized(HP) 13C MRI, as a 2-minute addition to an MRI exam, can detect aberrantly elevated metabolic pathways in aggressive prostate tumors, and is sensitive to early response to therapy, making it valuable for staging and restaging of advanced prostate cancer6-8. This study evaluated a new framework (Figure 1A) to extract and characterize radiomic features of metabolism (RFM) in advanced prostate cancer using novel abdominopelvic HP 13C MRI techniques, and conducted preliminary correlative analyses with clinical outcome measures.Methods
HP 13C Pyruvate MRI:Sixteen patients with advanced prostate cancer with various disease states and treatment regimens were studied using HP 13C+1H standard MRI on a clinical 3T system following injection of 250mM HP 13C pyruvate (Figure 1). Combination of novel MRI coils including a 13C QTAR ergonomic 8-channel array (Clinical MR Solutions) and 1H AIR coil (GE Healthcare) enabled coverage of either the whole abdomen or pelvis to assess the often widespread metastases.
Extraction of Radiomic Features of Metabolism (RFM):
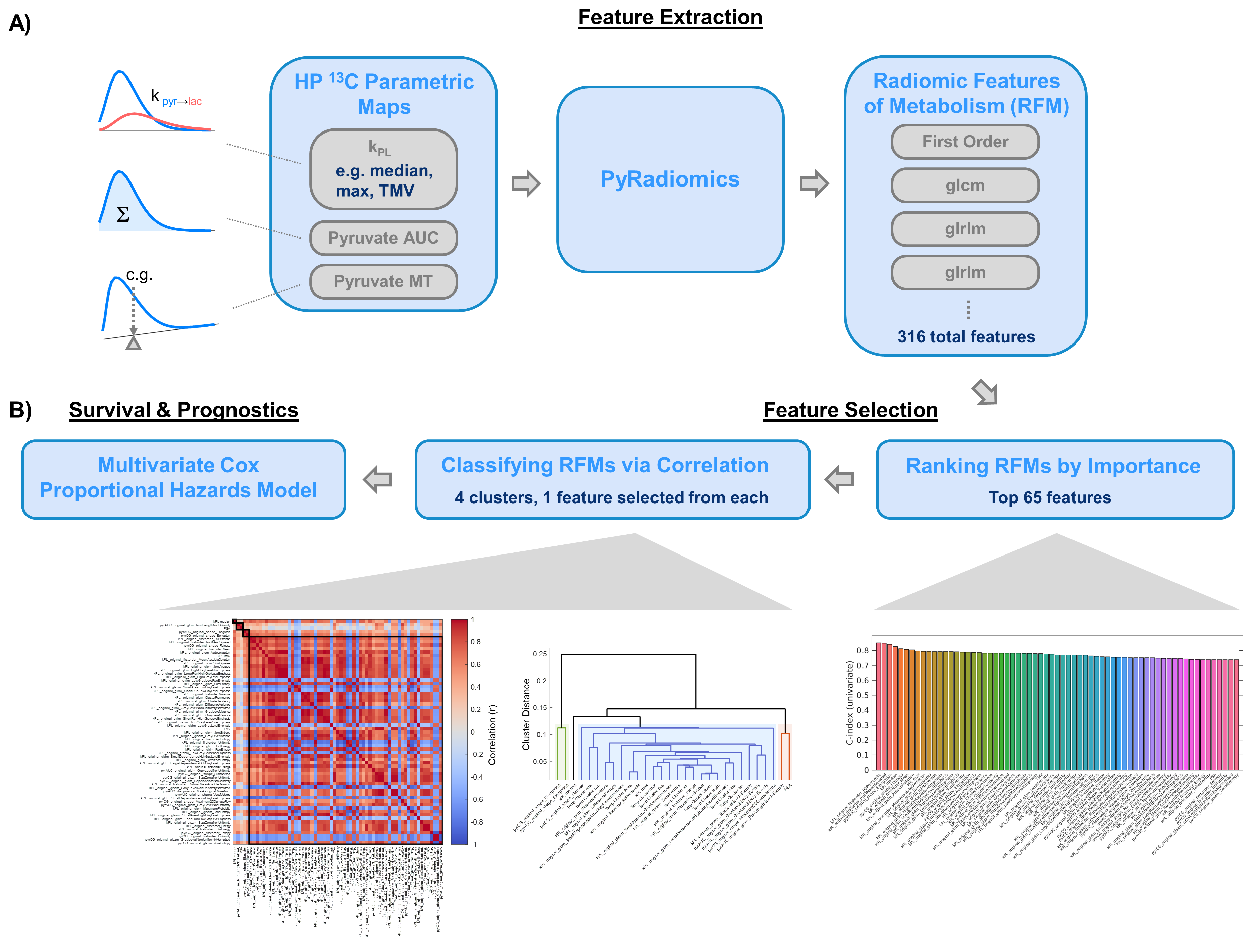
PyRadiomics9, an open-source IBSI-compliant software package, extracted a total of 316 RFMs from three source HP parametric maps, namely the pyruvate-to-lactate conversion rate(kPL)10, pyruvate signal summed-over-time (AUC, analogous to SUV in PET), and mean pyruvate time10 (Figure 4A) over ROIs drawn on metastatic & primary tumors.
RFM Selection and Classification for Uni- and Multivariate Survival Models:
Survival analyses using uni- and multivariate Cox proportional hazards models11 evaluated the prognostic values of these RFMs. Feature selection consisted of ranking their importance by Harrell’s C-index12, followed by agglomerative clustering13 classifiers to eliminate highly correlated (redundant) features(Figure 4B).
Results and Discussions
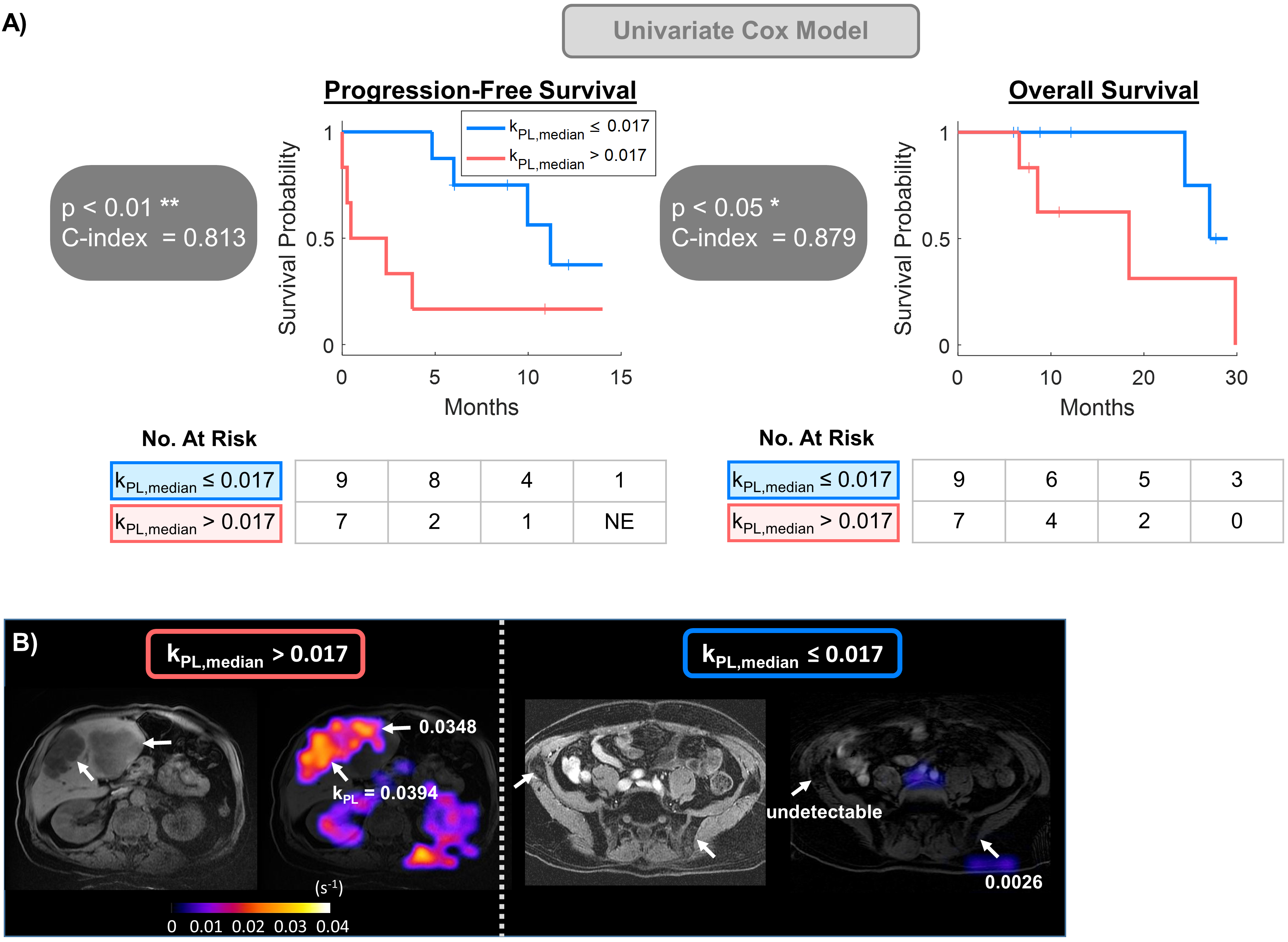
At the time of scans, 10 patients had castration-resistance PCa (CRPC) and 6 had hormone-sensitive PCa (HSPC). Staging-wise, 4 patients with metastases were M1c, 8 were M1b, one was M1a. Of the locally advanced subgroup, 2 were T4, and one was T3b.kPL was selected for the univariate analysis due to its clear biological rationale(Warburg effect)14. At the interim analysis, the univariate Cox model (Figure 2A) using kPL,median significantly predicted PFS(p<0.01) and OS(p<0.05). Kaplan-Meier statistics revealed longer median PFS(11.2 vs 0.5 months) and OS(NR vs 18.4 months) in the lower- vs higher-kPL subgroup, dichotomized by cutoff value kPL,median= 0.017s-1. Figure 2B illustrates a patient with extensive, metabolically active (i.e. high kPL) liver metastases, in contrast to a patient having osseous pelvic metastases with low/undetectable kPL across all the visualized tumor sites.
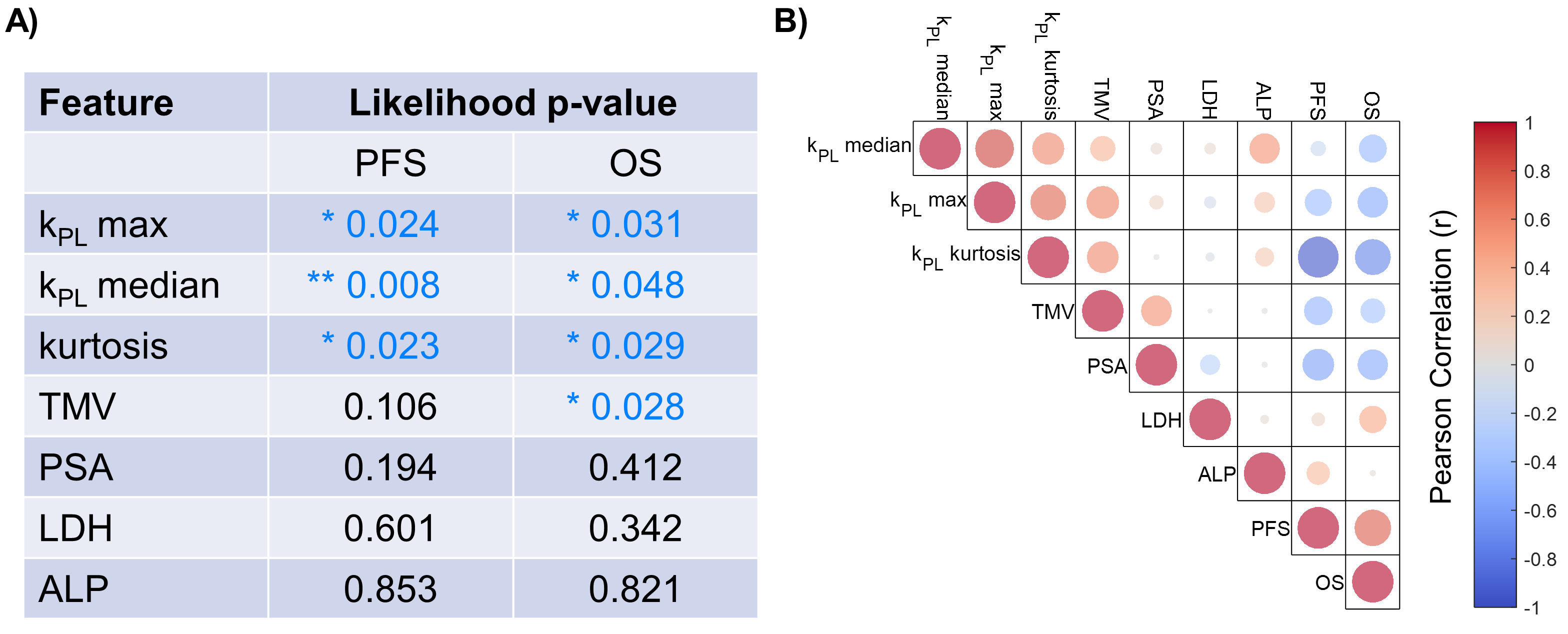
In the univariate analysis (Figure 3A), kPL max, median and kurtosis (i.e. the spread of kPL across the segmented tumors) each significantly predicted both PFS and OS, outperforming established clinical prognostic markers PSA15 and LDH16, suggesting these HP 13C-RFMs may possibly have stronger effect size to stand out in this small cohort. Preliminary statistics also identified a strongly negative correlation (Figure 3B) between kPL kurtosis and OS (r = -0.75), and moderately negative correlations between kPL,median with OS (r = -0.45), kPL,max with both PFS (r = -0.48) and OS (r = -0.54), and kurtosis with PFS (r = -0.37). These findings underscore the key biological rationale that high kPL kurtosis reflected tumor metabolic heterogeneity resulting from treatment-induced clonal evolution17 and increased mutational burden. This in turn gives rise to aggressive, treatment resistant subtypes and therefore poor survival. The moderate correlation between metabolic tumor volume(MTV) and PSA (r=0.55) reflects these biomarkers’ role as estimators of the tumor burden.
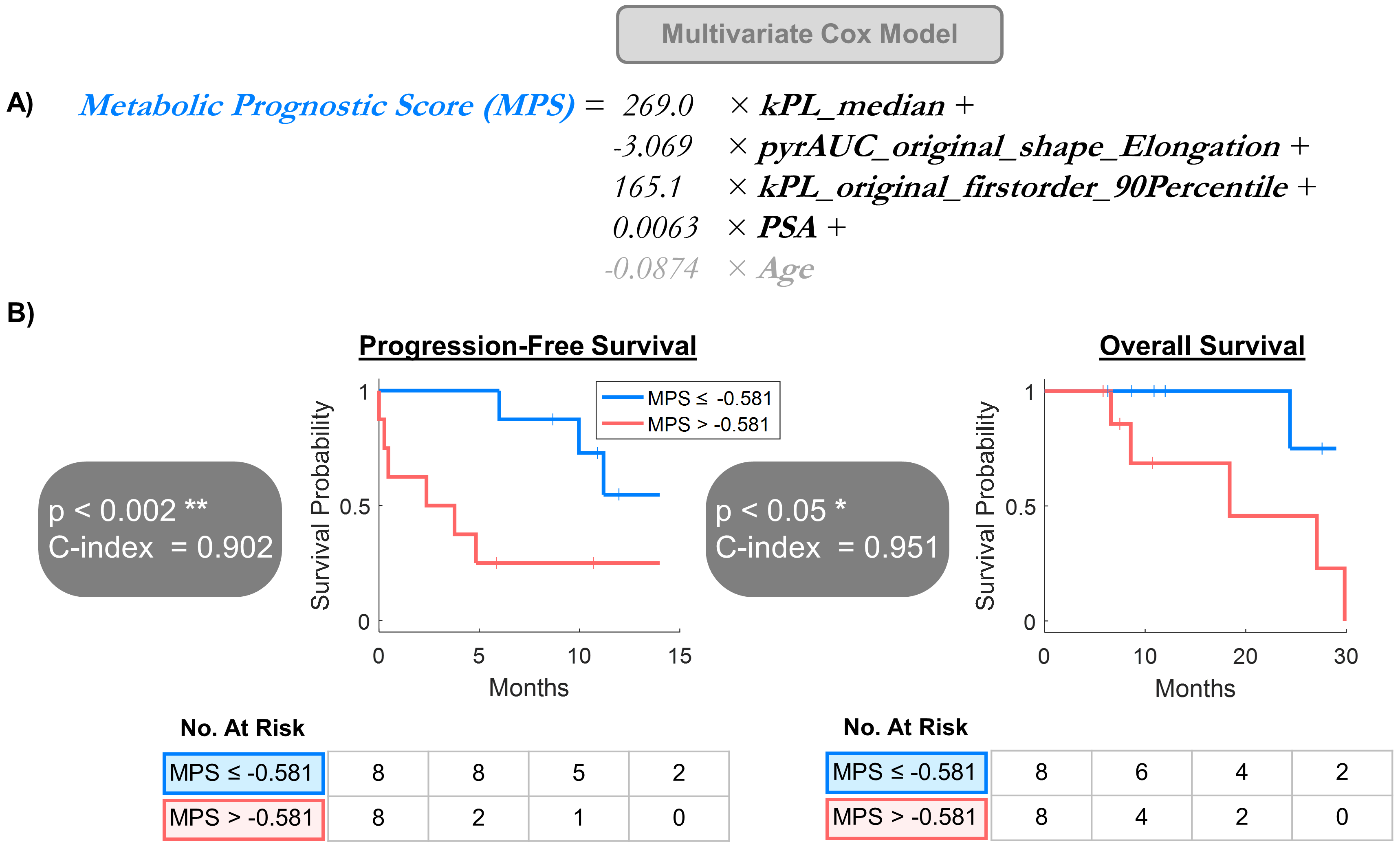
Multivariate Cox analysis (Figure 5) using metabolic prognostic score(MPS) combining the selected three RFMs and one serological feature significantly predicted PFS(p<0.002) and OS(p<0.05), with longer median PFS (NR vs 2.4 months) and OS (NR vs 18.4 months) in the lower- vs higher-risk subgroups, dichotomized by the cohort median MPS = -0.581. It should be noted this multivariate model is currently of exploratory nature given the limited sample size and will be refined once data from a larger cohort becomes available and survival endpoints mature.
Conclusions
Combination of novel HP 13C and 1H MRI coils and imaging techniques greatly increased spatial coverage across the whole abdomen or pelvis, enabling more comprehensive extraction and evaluation of RFMs in patients with metastatic and locally advanced prostate cancers. Preliminary analyses found that RFMs including kPL significantly predicted patient outcomes. These data strongly support further investigating the prognostic values of HP 13C MRI-derived metabolic features.Acknowledgements
This work was supported by grants from the NIH (R01CA256740, R01CA215694, R01CA238379, U01EB026412, P41EB013598). We would like to thank Dr. Duy Dang, Heather Daniel, Nikhil Deveshwar, Evelyn Escobar, Mary Frost, Dr. Yaewon Kim, Dr. Philip Lee, Louise Magat, Kimberly Okamoto, and Dr. James Slater for their help with this research.References
[1] Calais J et al., 18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: a prospective, single-centre, single-arm, comparative imaging trial. Lancet Oncol. 2019; 20(9), 1286-1294
[2] Fendler WP et al., Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer. JAMA Oncol. 2019; 5(6), 856-863
[3] Emmett L et al., The Additive Diagnostic Value of Prostate-specific Membrane Antigen Positron Emission Tomography Computed Tomography to Multiparametric Magnetic Resonance Imaging Triage in the Diagnosis of Prostate Cancer (PRIMARY): A Prospective Multicentre Study. Eur Urol. 2021; 80(6), 682-689
[4] Aggarwal R et al., Heterogeneous Flare in Prostate-specific Membrane Antigen Positron Emission Tomography Tracer Uptake with Initiation of Androgen Pathway Blockade in Metastatic Prostate Cancer. Eur. Urol. Oncol. 2018; 1(1), 78-82
[5] Aggarwal R et al., Clinical and Genomic Characterization of Treatment-Emergent Small-Cell Neuroendocrine Prostate Cancer: A Multi-institutional Prospective Study. Eur. Urol. Oncol. 2018; 36(24), 2492-2503
[6] Nelson SJ et al., Metabolic imaging of patients with prostate cancer using hyperpolarized [1-13C]pyruvate. Sci Transl Med 2013; 5(198), 198ra108
[7] Ardenkjaer-Larsen JH et al., Increase in signal-to-noise ratio of> 10,000 times in liquid-state NMR. PNAS. 2003; 100(18), 10158-10163
[8] Chen HY et al., Hyperpolarized 13C-pyruvate MRI detects real-time metabolic flux in prostate cancer metastases to bone and liver: a clinical feasibility study. Prostate Cancer Prostatic Dis. 2020; 23(2), 269-276
[9] Van Griethuysen JJM et al., Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017; 77(21), e104-e107
[10] Larson PEZ et al., Investigation of analysis methods for hyperpolarized 13C‐pyruvate metabolic MRI in prostate cancer patients. NMR Biomed. 2018; 31(11), e3997.
[11] Bradburn MJ et al., Survival analysis part II: multivariate data analysis–an introduction to concepts and methods. Br. J. Cancer. 2003; 89(3), 431-436.
[12] Harrell FE et al., Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996; 15(4), 361-387.
[13] Parmer C et al., Radiomic feature clusters and prognostic signatures specific for lung and head & neck cancer. Sci. Rep. 2015; 5(1), 11044.
[14] Vander Heiden MG et al., Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009; 324(5930), 1029-1033.
[15] Moreina D et al., Predicting Time From Metastasis to Overall Survival in Castration-Resistant Prostate Cancer: Results From SEARCH. Clin. Genitourin. Cancer. 2015; 15(1), 60-66.
[16] Mori K et al., Prognostic Value of Lactate Dehydrogenase in Metastatic Prostate Cancer: A Systematic Review and Meta-analysis. Clin. Genitourin. Cancer. 2015; 17(6), 409-418.
[17] Greaves M et al., Clonal evolution in cancer. Nature. 2012; 481(7381), 306-313.Figures