0232
Cardiac Diffusion in Python (CarDpy): An Open-Source Toolbox for Cardiac Diffusion Tensor Data Processing1Department of Radiology, Stanford University, Stanford, CA, United States, 2Department of Bioengineering, Stanford University, Stanford, CA, United States, 3Division of Radiology, Veterans Administration Health Care System, Palo Alto, CA, United States, 4Cardiovascular Institute, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Software Tools, Tissue Characterization, Cardiac Diffusion Tensor Imaging, cDTI, Heart, Data Processing
Motivation: cDTI provides several new and useful MRI biomarkers, but robust and reliable data processing pipelines are still needed to adequately handle cDTI data.
Goal(s): Goal: To demonstrate the benefits of an open-source Python cDTI data processing toolbox and its impact on measurement accuracy and precision.
Approach: A direct averaging and tensor-fitting data processing technique was compared to our open-source data processing pipeline. Data from healthy subjects was used to demonstrate improvements in the accuracy and uncertainty of cDTI metrics.
Results: Our open-source cDTI data processing toolbox provides smoother parametric maps that are more accurate with less uncertainty compared to direct averaging and tensor-fitting.
Impact: Development of Cardiac Diffusion in Python (CarDpy), an open-source python toolbox for cardiac diffusion tensor imaging (cDTI) data processing to facilitate reproducible cDTI research for new and established researchers. A strong foundation, plus software modularity encourages contributions from the community.
Introduction
Cardiac diffusion tensor imaging (cDTI) is a versatile MRI technique used to estimate myocardial microstructural organization [1]. In vivo cDTI exams require custom pulse sequences that account for bulk-physiologic motion to obtain meaningful data [2,3]. Additionally, image imperfections, such as motion-induced signal loss, respiratory motion, and poor ECG triggers can corrupt data, leading to poor-quality results. Careful data processing can correct several of these problems. The objective of this work was to create an open-source Python-based cDTI data processing framework and evaluate its performance.Software Overview
Our Python-based open-source software package, Cardiac Diffusion in Python (CarDpy), supports both DICOMs and NifTis. The framework incorporates several modules (Gibbs ringing correction, image registration, denoising, and DTI reconstruction) from the Diffusion Imaging in Python toolbox, an open-source software developed for neuro diffusion [4]. The remaining modules (shot-rejection, respiratory sorting, averaging, interpolation, cDTI angular projections, and a novel helix angle filter) were all developed for this framework. Most of the framework is automated, but several interactive graphical user interfaces have also been developed to provide insight during processing and fine-tuning as needed. CarDpy is available on GitHub (https://github.com/tecork/CarDpy).Methods
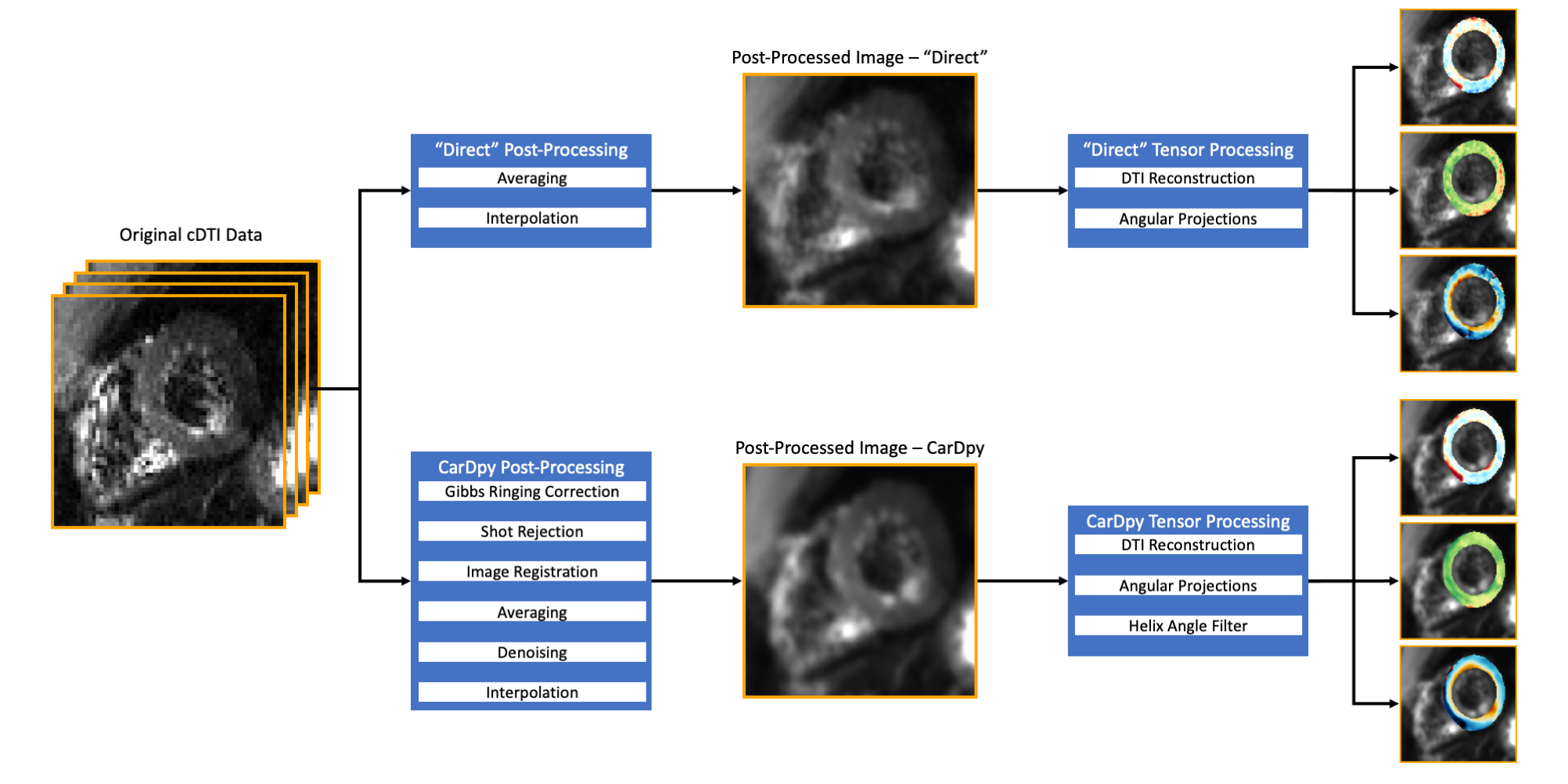
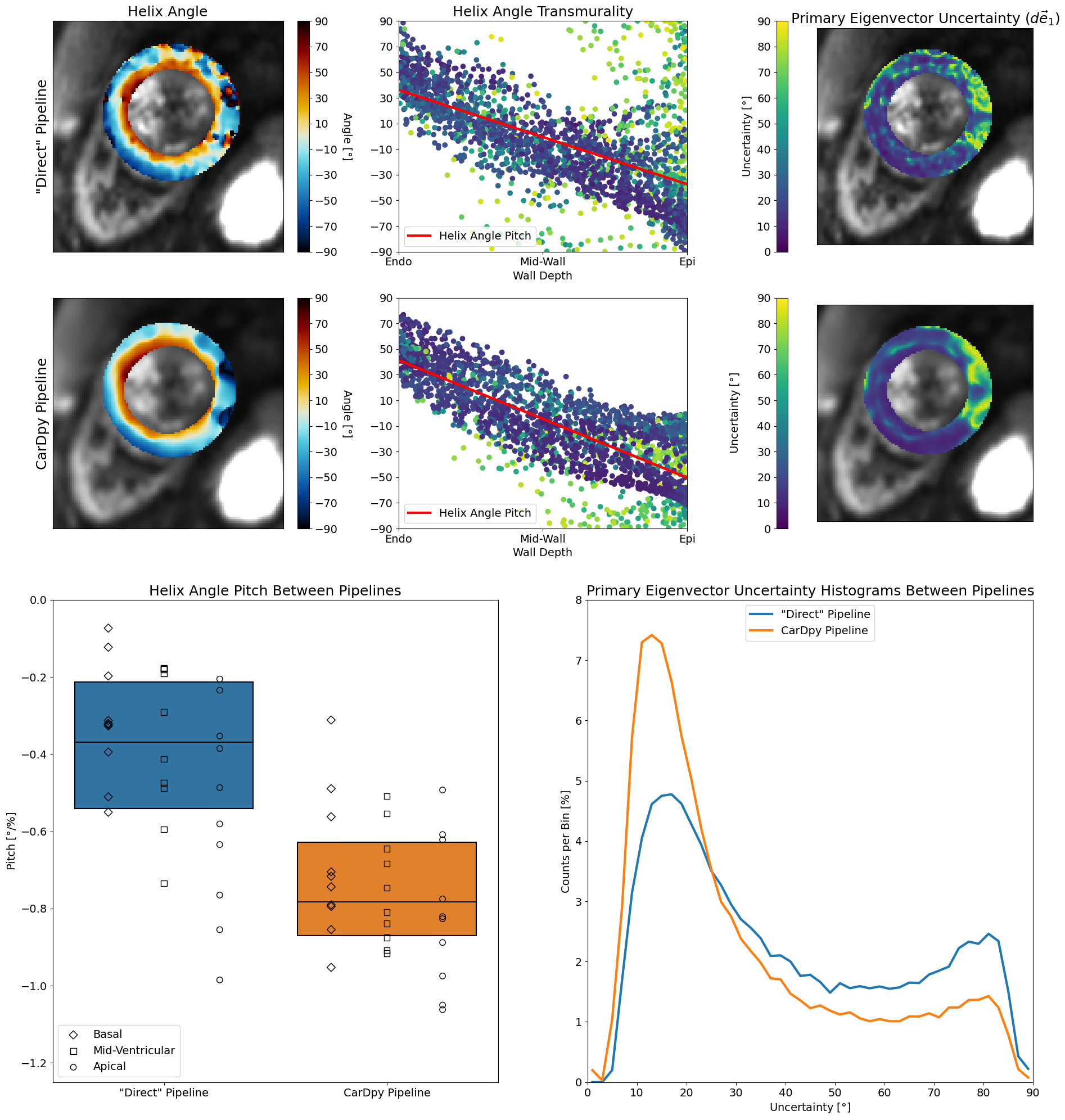
cDTI data was acquired in healthy volunteers (N=10, IRB, consent) using a 3T MRI (Vida Fit, Siemens), an 18-channel body coil, and a 32-channel spine coil. Each volunteer was scanned using an ECG-gated, free-breathing, M0M1M2 motion-compensated spin-echo diffusion sequence with slice-following [5] for basal, mid-ventricular, and apical slices. Protocol: resolution=2×2×8mm3, b-values=[0, 350]s/mm2, diffusion directions=15, TE/TR=91ms/3×R-R interval, 2× parallel imaging (GRAPPA), partial Fourier=6/8, averages=4, 64 seconds/slice. The images then underwent two different data processing pipelines: direct averaging and tensor-fitting data processing technique (“direct”) and our open-source pipeline, CarDpy. In the "direct" pipeline the data was only averaged and interpolated. In the CarDpy pipeline, the data underwent: Gibbs ringing correction [6], shot-rejection, affine image registration, averaging, local PCA denoising [7], and interpolation. Both pipelines then underwent a non-linear least squares tensor reconstruction [8] and the CarDpy pipeline applied a novel filter to the helix angle (HA) maps. A general overview of the two pipelines can be seen in Figure 1. Manual segmentation of the left ventricle (LV) was used to generate cDTI parametric maps of mean diffusivity (MD), fractional anisotropy (FA), and HA for all volunteers across all slices. Parametric map precision was evaluated by bootstrapping (Nboot = 400 [9]) the data and then using the bootstrapped data to estimate parameter uncertainty [10] for MD (dMD), FA (dFA), and the primary eigenvector (de1, “cone of uncertainty”). Boxplots were generated for MD, FA, and HA pitch (HAP) across all volunteers for all slices. HAP was calculated by computing the linear fit of HA data transmurally across the myocardium. Histograms were generated for dMD, dFA, and de1 by pooling all the LV voxels across all volunteers for all slices. Medians and 95% confidence intervals (using a bootstrapping approach) were computed for MD, FA, and HAP. Medians and maximum likelihoods were computed for dMD, dFA, and de1.Results
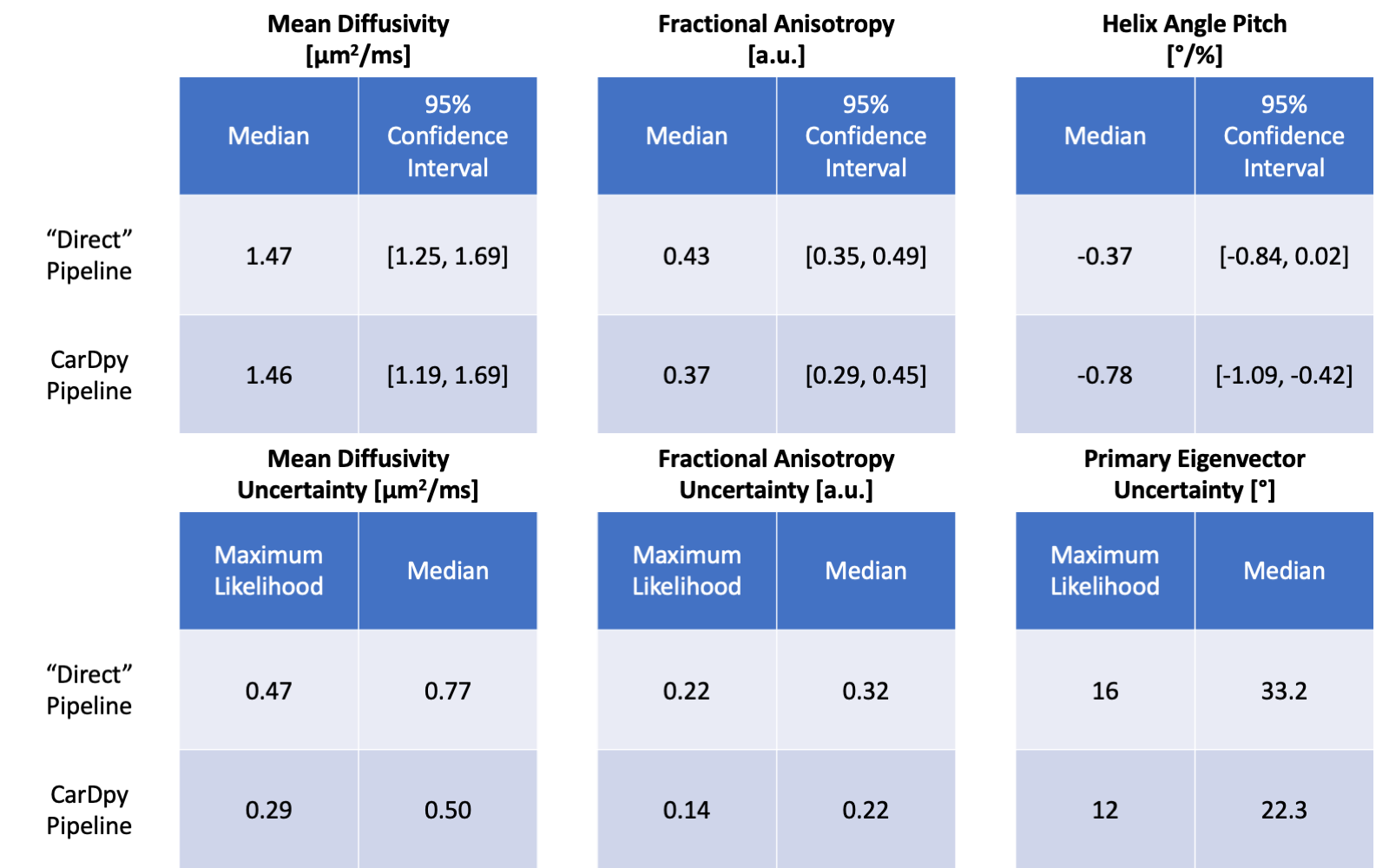
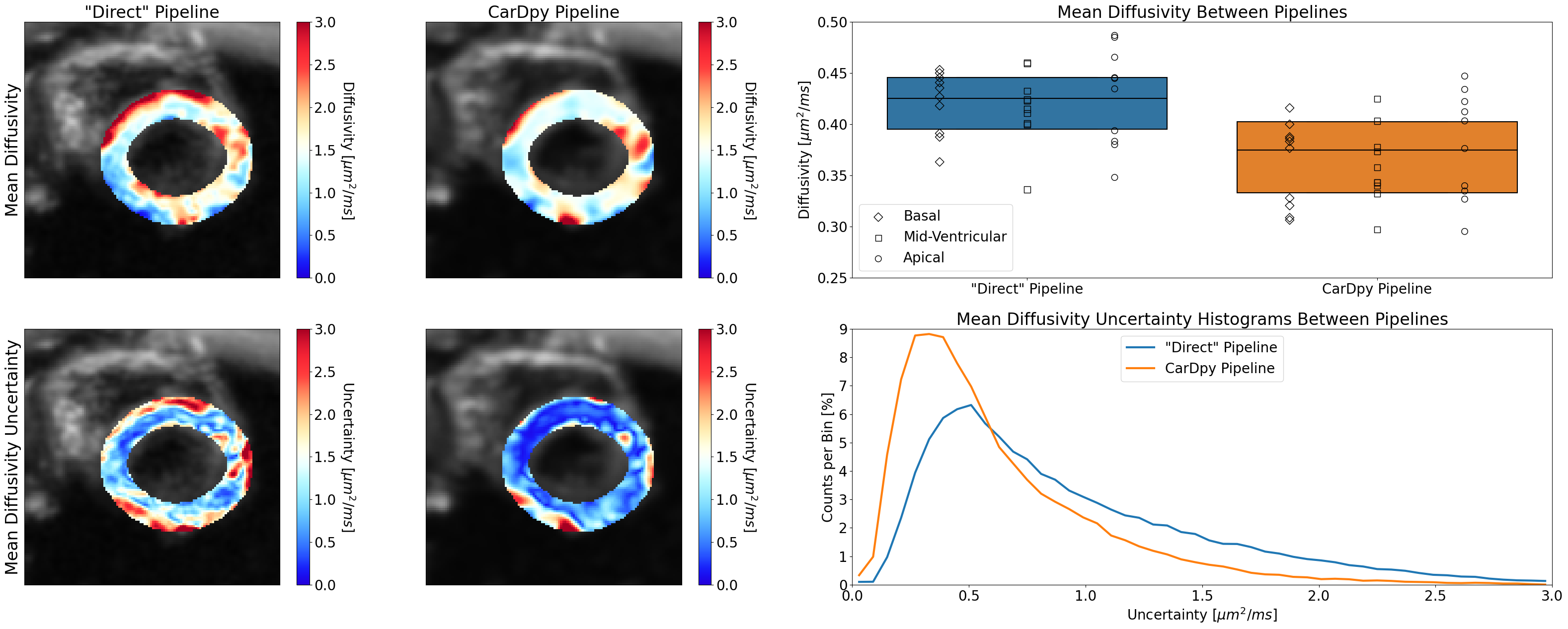
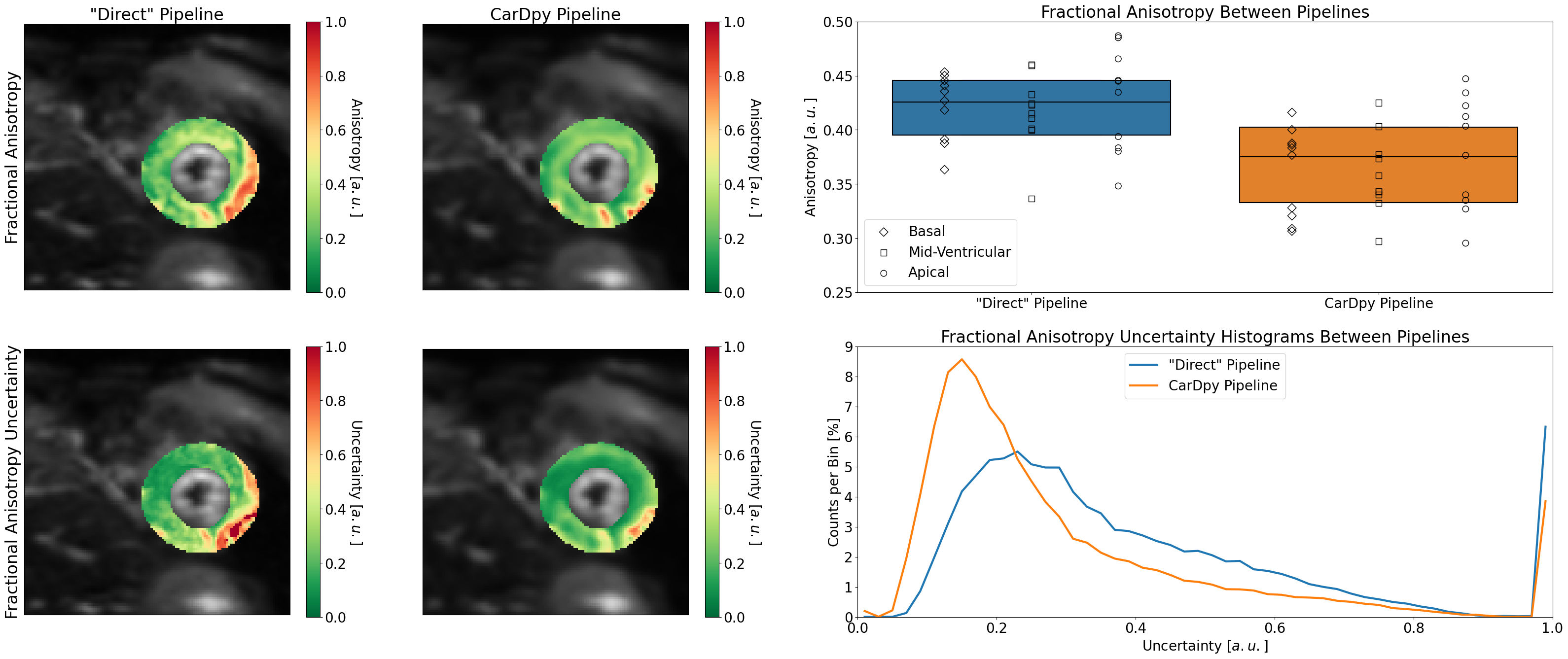
In Table 1, a list of the medians and 95% confidence intervals for MD, FA, and HAP can be seen in addition to the maximum likelihood and median for dMD, dFA, and de1. The median MD (Figure 2) for the “direct” and CarDpy pipelines were nearly identical at 1.47 μm2/ms and 1.46 μm2/ms, respectively. The median dMD for the CarDpy pipeline (0.50 μm2/ms) was lower than the “direct” pipeline (0.77 μm2/ms). In Figure 3, the median FA for the CarDpy pipeline (0.37) was lower than the “direct” pipeline (0.43). The median dFA for the CarDpy pipeline (0.22) was also lower than the “direct” pipeline (0.32). The HAP (Figure 4) shows an increased steepness in the median pitch for the CarDpy pipeline (-0.78) compared to the “direct” pipeline (-0.37). Additionally, the median de1 displayed less uncertainty in the CarDpy pipeline (22.3°) compared to the “direct” pipeline (33.2°).Discussion/Conclusion
The CarDpy pipeline shows notable improvements across all cDTI parametric uncertainty while using the same data. This suggests that the additional careful data processing provides more reliable and more accurate results. An additional benefit that is apparent in the CarDpy results produce more uniform parametric maps, which makes it easier to interpret the results for clinical applications. Lastly, the addition of the novel helix angle filter creates a notable difference in HAP between the “direct” and the CarDpy pipeline. The increased steepness in HAP from the CarDpy pipeline is more on par with what prior literature suggests. Overall, this open-source toolbox provides researchers with a reproducible approach to processing cDTI data, with demonstrated improvements in accuracy and decreases in measurement variability.Acknowledgements
We would like to acknowledge our funding sources which include NSF 2205103 to DBE, NIH R01 HL131823 to DBE, NIH R01 HL152256 to DBE, and AHA 23PRE1018442 to AJH.References
1. Nielles-Vallespin Sonia, Scott Andrew, Ferreira Pedro, Khalique Zohya, Pennell Dudley, Firmin David. Cardiac diffusion: technique and practical applications. Journal of Magnetic Resonance Imaging. 2020;52(2):348–368.
2. Stoeck Christian T, Scott Andrew D, Ferreira Pedro F, et al. Motion-induced signal loss in in vivo cardiac diffusion-weighted imaging. Journal of Magnetic Resonance Imaging. 2020;51(1):319.
3. Moulin Kevin, Stoeck Christian T, Axel Leon, et al. In Vivo Cardiac Diffusion Imaging Without Motion- Compensation Leads to Unreasonably High Diffusivity. Journal of Magnetic Resonance Imaging. 2023.
4. Garyfallidis Eleftherios, Brett Matthew, Amirbekian Bagrat, et al. Dipy, a library for the analysis of diffusion MRI data. Frontiers in Neuroinformatics. 2014;8:8.
5. Moulin Kévin, Croisille Pierre, Feiweier Thorsten, et al. In vivo free-breathing DTI and IVIM of the whole human heart using a real-time slice-followed SE-EPI navigator- based sequence: A reproducibility study in healthy volunteers. Magnetic Resonance in Medicine. 2016;76(1):70–82.
6. Kellner Elias, Dhital Bibek, Kiselev Valerij G, Reisert Marco. Gibbs-ringing artifact removal based on local subvoxel-shifts. Magnetic resonance in medicine. 2016;76(5):1574–1581.
7. Manjón José V, Coupé Pierrick, Concha Luis, Buades Antonio, Collins D Louis, Robles Montserrat. Diffusion weighted image denoising using overcomplete local PCA. PloS one. 2013;8(9):e73021
8. Kingsley Peter B. Introduction to diffusion tensor imaging mathematics: Part III. Tensor calculation, noise, simulations, and optimization. Concepts in magnetic resonance part A. 2006;28(2):155–179.
9. Davidson Russell, MacKinnon James G. Bootstrap tests: How many bootstraps? Econometric Reviews. 2000;19(1):55-68.
10. Aliotta Eric, Moulin Kévin, Magrath Patrick, Ennis Daniel B. Quantifying precision in cardiac diffusion tensor imaging with second-order motion-compensated convex optimized diffusion encoding. Magnetic Resonance in Medicine. 2018;80(3):1074–1087. [TEC1]Tyler Don’t forget this
Figures