0231
Assessing Ventilation and Gas Exchange of Lung Transplant Recipients with Hyperpolarized Xenon-1291University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Keywords: Hyperpolarized MR (Gas), Hyperpolarized MR (Gas)
Motivation: Improving the diagnosis and monitoring of chronic lung allograft dysfunction (CLAD) post-lung transplantation may lead to improved long-term patient outcomes.
Goal(s): To identify hyperpolarized xenon-129 imaging markers for more comprehensively evaluating lung function in transplant recipients.
Approach: A multi-breath xenon-polarization transfer contrast (XTC) technique was used to quantify ventilation and gas exchange longitudinally in lung transplant patients.
Results: Correlations between the derived imaging metrics and current clinical standards for assessing lung function provided additional insight into the functional changes associated with post-transplant recovery or decline.
Impact: Hyperpolarized xenon-129 MRI enables more comprehensive assessments of the functional and physiological changes associated with recovery and/or deterioration after lung transplantation, potentially leading to earlier CLAD diagnosis and improved long-term outcomes.
Introduction
While short-term outcomes for lung transplantation (LTx) have improved, chronic lung allograft dysfunction (CLAD) continues to significantly lower long-term survival rates compared to other solid organ transplants. Despite the fact that pulmonary function typically recovers over the first post-LTx year, identifying factors associated with functional deterioration or suboptimal recovery during this period may provide insight into structural or functional aspects of graft health, improving our ability to predict CLAD. While current clinical lung function assessments are limited to global, effort-based measures, hyperpolarized xenon-129 (HXe) MRI is capable of quantifying regional ventilation and gas exchange to more thoroughly assess post-LTx lung function. Here, we compared HXe imaging metrics with spirometry to identify improved lung function markers and evaluated LTx recipients who appeared to either recover or decline one year post-surgery.Methods
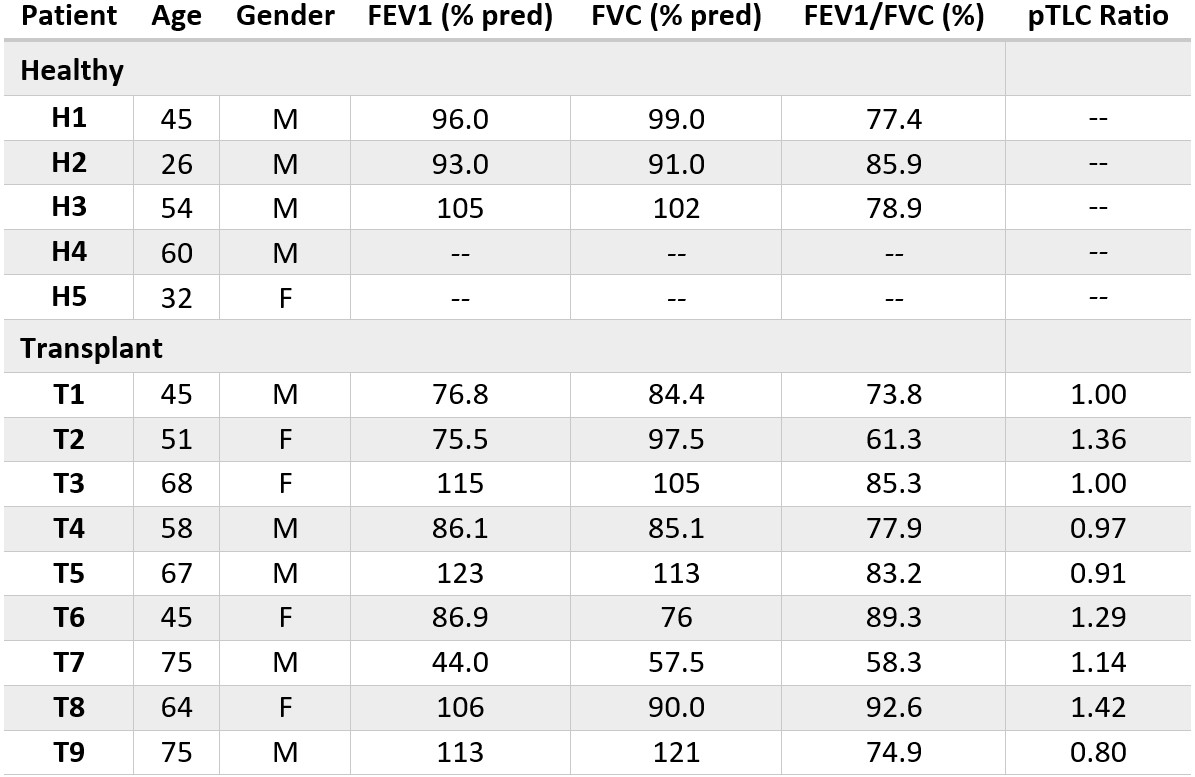
9 bilateral LTx recipients were imaged longitudinally at multiple time points between 3 and 24 months post-surgery. Pulmonary function testing was performed the day of imaging and baseline values, calculated as the averages of FEV1, FVC, and FEV1/FVC associated with the two highest post-LTx FEV1s, are shown in Table 1. Total lung capacities were estimated from the ages, heights, and genders of the donors and recipients1; the ratio of donor-to-recipient predicted total lung capacities (pTLCs) are also shown in Table 1. A previous cohort of 5 healthy volunteers and their available spirometry were included for reference. All imaging was performed with an Institutional Review Board (IRB) approved protocol in a 1.5T scanner (Magnetom Avanto, Siemens) using an 8-channel xenon-129 coil (Stark Contrast, Germany). A prototype commercial system (XeBox-E10, Xemed LLC) was used to polarize 87% enriched xenon-129.Imaging was performed with a multi-breath xenon-polarization transfer contrast (XTC) technique2, repeated for reproducibility. Subjects were administered a series of 6 wash-in (room air supplemented with 50 ml HXe) and 4 wash-out (room air without HXe) breaths, repeated with and without selective-saturation of red blood cell (RBC) or tissue membrane (Mem) resonances. Each image was manually triggered at end-exhalation and acquired with a 3D stack-of-spirals. For the sets of RBC and Mem saturations, a series of 40 and 20 Gaussian RF pulses, respectively, were applied immediately preceding the image acquisition. These RF pulses had: 180° flip angle, 8 ms duration, 30 ms TR. Imaging parameters included: flip angle of 4°, TR/TE = 7.68/0.84 ms, 11 interleaves with 5.12 ms readouts, matrix size = 80x80x8, and FOV = 350x350x200 mm3. Signal buildup and decay during wash-in/wash-out were fit to a gas replacement model2 to derive maps of tidal volume (TV), functional residual capacity (FRC), fractional ventilation (FV), RBC-gas exchange (fRBC), membrane-gas exchange (fMem), and RBC-membrane exchange (fRBC:Mem).
Results and Discussion
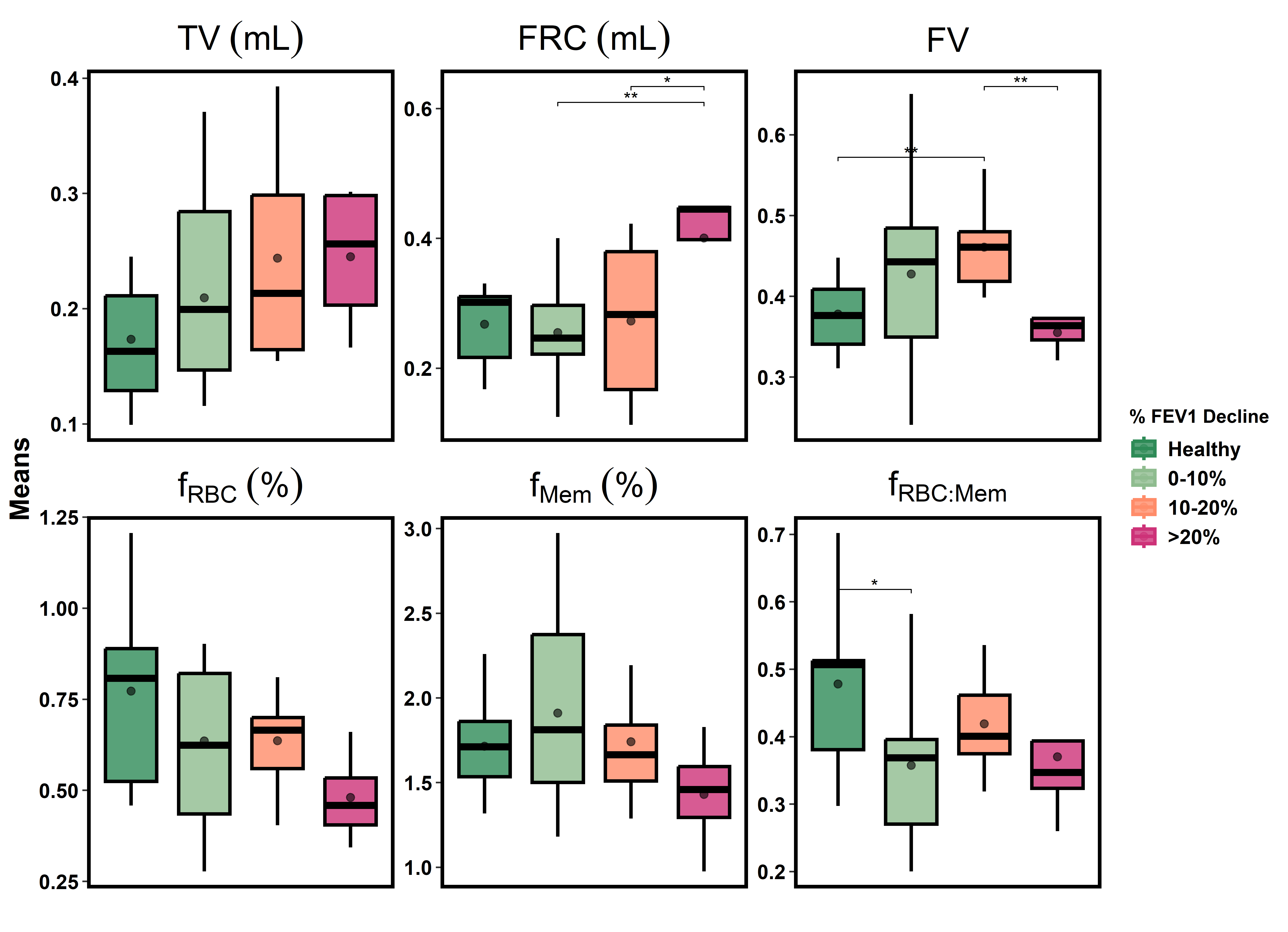
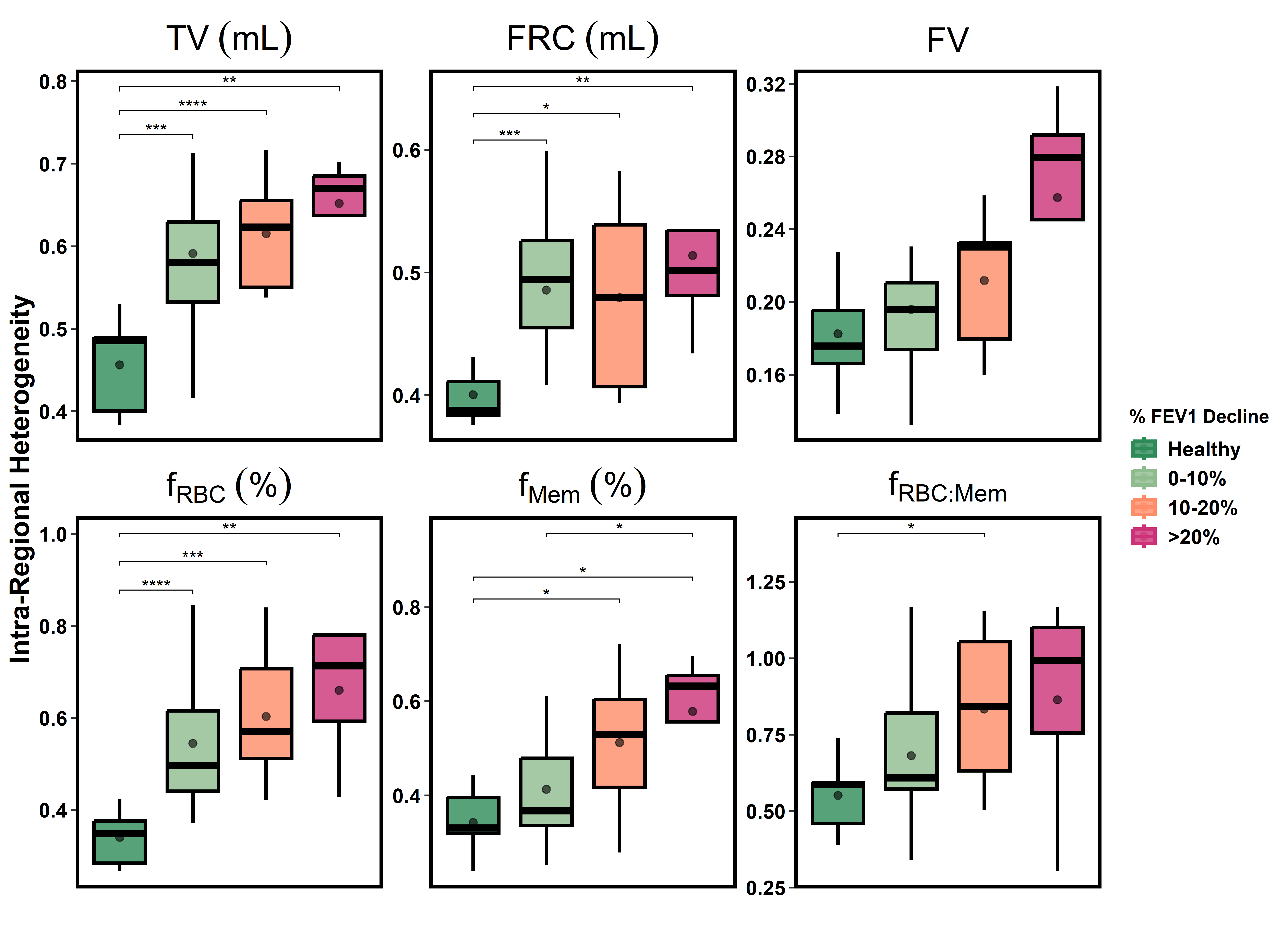
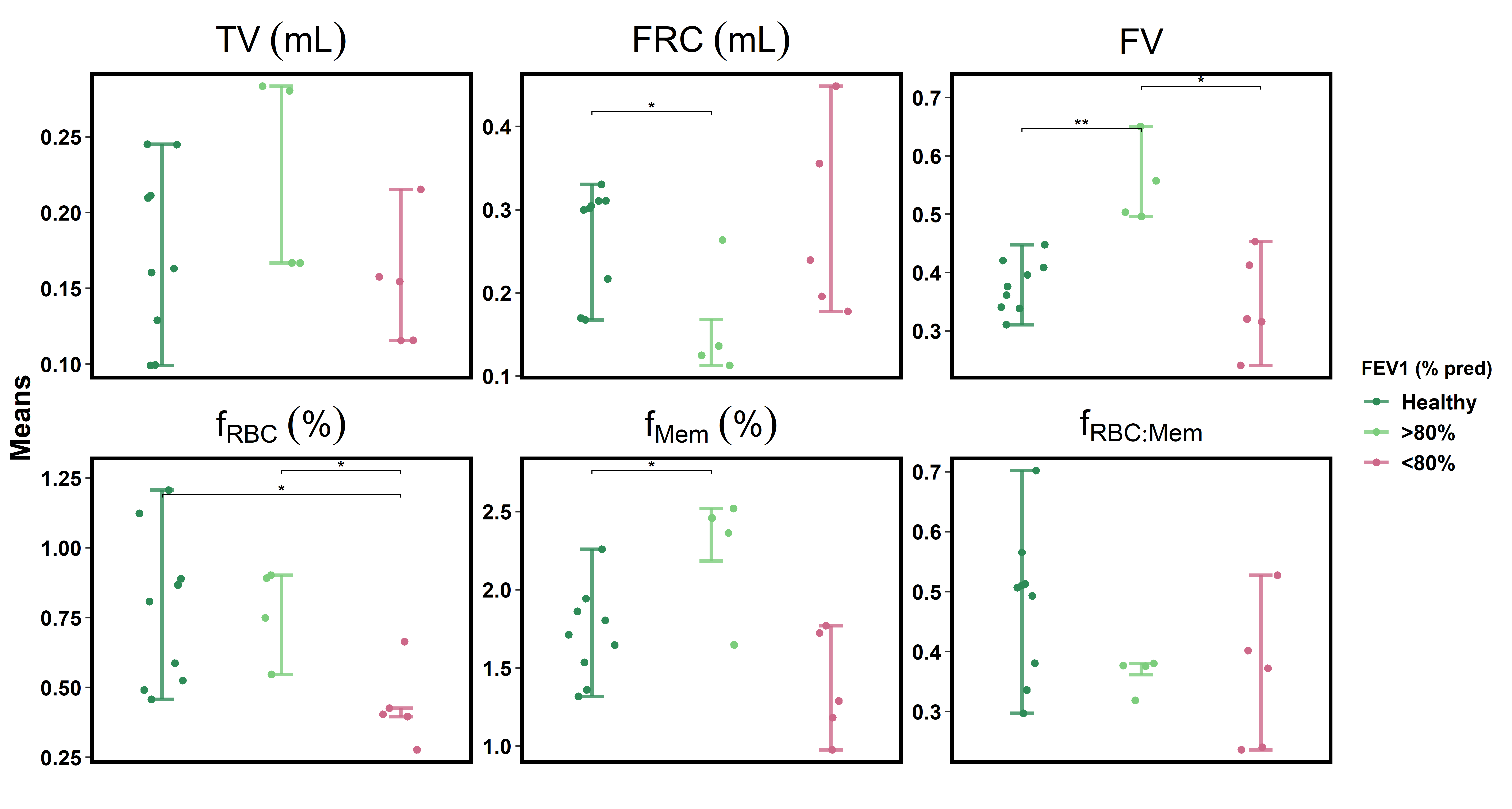
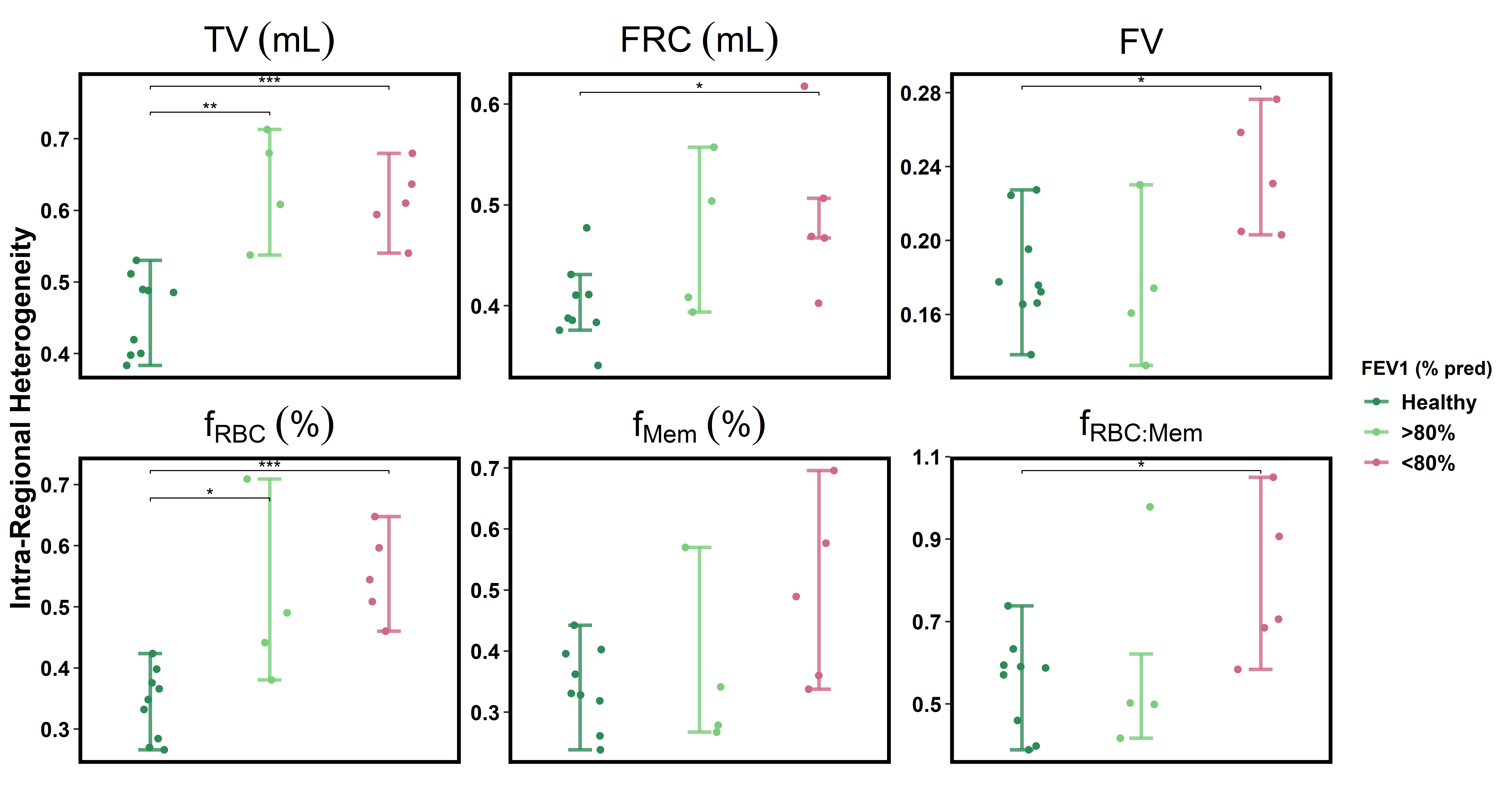
To better evaluate the HXe metrics given the high degree of inter-patient variability inherent with transplantation, each imaging session was independently consolidated into 3 groups based on percent decline from baseline FEV1: 0-10% decline, 10-20% decline, and >20% decline. Whole-lung averages for these 3 groups and the healthy cohort can be seen in Figure 1. While sample sizes were limited, fRBC, and particularly fMem, decreased noticeably with greater FEV1 decline. The most significant changes observed in the >20% FEV1 decline group, however, were for FRC and FV. The intra-regional heterogeneities, calculated as the average of the standard deviations of each slice normalized by the whole-lung mean, are shown in Figure 2—more clearly correlating with declining FEV1 across each metric.As pulmonary function typically recovers over the first year post-transplant, poor recovery or deteriorating lung function during this period could be an early CLAD indicator. Available LTx recipients were therefore separated into two groups based on their percent-predicted FEV1 one year post-LTx. No trends were observed based on pTLCs, with recovering patients (>80% FEV1) and decliners (<80% FEV1) exhibiting similar average graft size ratios (0.94 and 1.05, respectively). Figures 3 and 4 show whole-lung averages and intra-regional heterogeneities for each parameter in the available transplant subjects and healthy cohort. Compared to the recovering patients, decliners displayed decreased FV, fRBC, and fMem, consistent with reduced lung function. Recovering patients also presented significantly elevated FV and fMem, as well as reduced FRC, compared to both healthy subjects and declining patients. These changes, particularly for FRC, are expected effects of oversized allografts and increased elastic recoil. The fact that recovering patients each received similar-sized grafts to their native lungs suggests that increased recoil via surfactant production may play a crucial role in graft health, providing a potential marker for CLAD onset and/or progression.
Conclusion
HXe MRI identified ventilation and gas exchange markers capable of more comprehensively evaluating functional differences among lung transplant recipients.Acknowledgements
No acknowledgement found.References
[1] Mason D P, Batizy L H, Wu J, et al. Matching donor to recipient in lung transplantation: how much does size matter? The Journal of thoracic and cardiovascular surgery. 2009; 137:1234-1240.
[2] Amzajerdian F, Hamedani H, Baron R, et al. Simultaneous quantification of hyperpolarized xenon-129 ventilation and gas exchange with multi-breath xenon-polarization transfer contrast (XTC) MRI. Magn Reson Med. 2023; 90:2334-2347.
Figures