0220
Setting the stage for a clinical translation of hyperpolarized 13C-fumarate1Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 2Cancer Research UK Cambridge Centre, Cambridge, United Kingdom, 3Cancer Research UK Cambridge Institute, University of Cambridge, Cambridge, United Kingdom, 4Division of Experimental Medicine & Immunotherapeutics, Department of Medicine, University of Cambridge, Cambridge, United Kingdom, 5Cambridge Clinical Trials Unit, Cambridge University Hospitals NHS Trust, Cambridge, United Kingdom
Synopsis
Keywords: Hyperpolarized MR (Non-Gas), Non-Proton, Fumarate, Necrosis, Treatment Response
Motivation: Clinical translation of hyperpolarized 13C-fumarate has the potential to enable early, non-invasive assessment of treatment response in cancer.
Goal(s): To advance a novel hyperpolarized probe from the laboratory to the clinic.
Approach: Translation involved optimizing clinical scale hyperpolarization, establishing an imaging protocol at clinical field strength (3T), preclinical toxicology and first in-human injections.
Results: 13C-fumarate showed good hyperpolarization properties and the imaging protocol achieved sufficient spectral separation of peaks and spatial separation of phantoms respectively. Toxicological assessment demonstrated the safety of 13C-fumarate, no adverse events observed in rodents and humans have so far been observed.
Impact: While promising preclinical molecules exist, clinical hyperpolarized 13C MRI lacks probe versatility due to a complex, unclear translation process. This study on fumarate narrows the gap between preclinical and clinical utility and fosters transparent clinical translation pipelines for the field.
Introduction
Early, non-invasive assessment of treatment response is critical in oncology1. 13C-imaging with hyperpolarized (HP) [1-13C]pyruvate has shown promise in preclinical2 and clinical3 studies to address this need. As well as pyruvate, several HP molecules have been introduced preclinically to detect biomarkers such as pH or redox state4,5,6. However, the steps required for clinical translation remain challenging and opaque7. We thus present a pathway for clinical translation of HP [1,4-13C2,2,3-d2]fumarate (13C-fumarate), which preclinically has been shown to detect early treatment induced tumour cell necrosis through the fumarase-catalysed conversion to HP [1,4-13C2,2,3-d2]malate (13C-malate)8.Methods
Hyperpolarization: 0.38g 13C-fumarate was dissolved in 0.66g DMSO and mixed for 2h. 0.019g electronic paramagnetic agent (EPA) was added, the mixture stirred for 2h and then transferred to a SPINlab hyperpolarizer. After dissolution (in 51g H2O), it was neutralized in 29.7g H2O mixed with 7.3g buffer (333mM TRIS, 600mM NaOH, 333mg/L Na2EDTA). The final concentration of dissoluted 13C-fumarate was 35mM.Polarization level (Phyp) and T1: The relative signal enhancement of the hyperpolarized (Shyp, TR=1s, αhyp=3°) vs. thermally polarized (Stherm, αtherm=60°) magnitude spectrum was acquired at 3T (MR750) and using a dual-tuned 1H/13C head coil. The signal was back-calculated to the time of dissolution and flip angle corrected (eq.1). T1 was fitted by a monoexponential decay and corrected for repeated RF-excitation (eq.2).
Eq.1: $$P_{\text{hyp}}=\frac{S_{\text{hyp}}}{S_{\text{therm}}}\cdot \frac{\sin(\alpha_{\text{therm}})}{\sin(\alpha_{\text{hyp}})}$$
Eq.2: $$T_{\text{1,corr}}=\frac{1}{\frac{1}{T_{1}}+\frac{\ln \cos(\alpha_{\text{hyp}})}{\text{TR}}}$$
Fumarate to malate conversion: Approximately 15ml HP 13C-fumarate were added to three phantoms with varying fumarase concentrations (0, 3.3, 7.7U/ml). Slice-localized spectroscopy (3min, TR=10s, FA=3°) was followed by FID-CSI (FOV=20cm, FA=10°, TR=116ms, BW=5kHz, grid size=20x20, total duration=7s).
Dose escalation: Sprague Dawley rats (n=18) received two single doses (either 5, 30 or 60mg/kg) of 13C-fumarate on day 1 and 8. Three rats were assessed per sex and dose, to give a total of 18. The study was outsourced to Covance Laboratories.
Healthy volunteers: Five healthy volunteers received 13C-fumarate outside the scanner at increasing injection rates (0.04, 0.4, 5mL/s) and doses (0.96 and 1.92mg/kg). Physiological parameters were monitored pre-and 1h post-injection with safety bloods pre-and post-dosing.
Results
The hyperpolarization process was optimized varying EPA concentrations, microwave frequencies and attenuation until optimal conditions found at 20mM EPA, 140.055GHz and 8dB attenuation (Fig.1). The hyperpolarized signal decayed with a T1 of 76s (Fig.2). The solid-state polarization level (t=0) was determined to be 19%. Adding HP 13C-fumarate to phantoms (Fig.3) with varying fumarase concentrations allowed spectroscopic detection of HP 13C-malate. Subsequently acquired FID-CSI data enabled calculation of a 13C-malate/13C-fumarate ratio map. The 13C-malate-to-13C-fumarate ratio increased linearly over time. Dose escalation in rats (Fig.4) showed an increasing plasma concentration of 13C-fumarate. No increase in plasma concentration after administration of the second daily dose compared to the first dose was observed, indicating rapid return to baseline plasma levels. Similarly, no accumulation in plasma could be observed between day 1 and day 8. Preliminary data from ongoing healthy volunteer injections (so far: n=5, planned total: n=9, Fig.5) have so far revealed stable vital signs, including heart rate (HR), body temperature, mean arterial pressure (MAP) and blood oxygen level (SpO2) pre-and post-injection. Additionally, safety blood have demonstrated no adverse signals. There have been no adverse event reports to date.Discussion
The solid-state polarization level of 19% is acceptable for prospective human studies, as we commonly assume ~10% to be sufficient for most HP pyruvate studies. A T1 of 76s in solution results in a polarization level of 8-10% at the time of injection (assuming a transfer time of 50-60s). The in vivo T1 will be reduced, but can potentially be further increased by using D2O as a dissolution agent9. The imaging protocol effectively detected 13C-malate and differentiated it from the dominant fumarate peak. Phantoms with varying enzyme concentrations were distinguishable. Monitoring the 13C-malate/13C-fumarate ratio over time demonstrated the method’s sensitivity to ongoing conversion. The rat dose escalation study used up to >10x the planned maximum dose for humans for single injections and there were no signs of acute systemic toxicity, thus setting the no-observed-adverse-effect-level (NOAEL)10 at 120mg/kg/day. Additional stability, mutagenic potential and hemocompatibility tests (not shown) and the first five human administrations further confirmed the compound’s preliminary safety.Conclusion
We have demonstrated a process that yields sufficient hyperpolarization at the required volume for clinical use and established an imaging protocol suitable for clinical magnetic field strengths. Preclinical toxicology showed the safety of this new probe and we have now undertaken first-in-human injections of 13C-fumarate. Similar approaches can be used for the clinical translation of other novel, promising hyperpolarized 13C-labeled molecules.Acknowledgements
This research was supported by the NIHR Cambridge Biomedical Research Centre (NIHR203312). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. JB acknowledges support from the National Cancer Imaging Translational Accelerator (NCITA). MM acknowledges support from the Cambridge Experimental Cancer Medicine Centre and the Cancer Research UK Cambridge Centre. PW acknowledges support from the Gates Cambridge Trust (#OPP1144). FG and KMB acknowledge support from The Mark Foundation Institute for Integrated Cancer Medicine (MFICM).References
- Martens M et al. Tumor Response to Treatment: Prediction and Assessment. Curr Radiol Rep 2. 2014;62
- Day Sam E et al. Detecting tumor response to treatment using hyperpolarized 13C magnetic resonance imaging and spectroscopy. Nat Med. 2007 Nov;13(11):1382-7
- Woitek R et al. Hyperpolarized Carbon-13 MRI for Early Response Assessment of Neoadjuvant Chemotherapy in Breast Cancer Patients. Cancer Res. 2021;81(23):6004-6017
- Grashei M, Wodtke P et al. Simultaneous magnetic resonance imaging of pH, perfusion and renal filtration using hyperpolarized 13C-labelled Z-OMPD. Nat Commun 14, 5060 (2023)
- Bohndiek SE et al. Hyperpolarized [1-13C]-Ascorbic and Dehydroascorbic Acid: Vitamin C as a Probe for Imaging Redox Status in Vivo. J. Am. Chem. Soc. 2011 June;133(30): 11795–11801
- Moreno KX et al. Real-time Detection of Hepatic Gluconeogenic and Glycogenolytic States Using Hyperpolarized [2-13C]Dihydroxyacetone. J Biol Chem. 2014;289(52):35859–67
- Kurhanewicz J et al. Hyperpolarized 13C MRI: Path to Clinical Translation in Oncology. Neoplasia. 2019 Jan;21(1):1-16.
- Gallagher AF et al. Production of hyperpolarized [1,4-13C2]malate from [1,4-13C2]fumarate is a marker of cell necrosis and treatment response in tumors. Proc Natl Acad Sci. 2009;106(47):19801-6
- Keshari KR, Wilson DM. Chemistry and biochemistry of 13C hyperpolarized magnetic resonance using dynamic nuclear polarization. Chem Soc Rev. 2014 Mar; 43(5): 1627–1659
- Dorato M, Engelhardt JA. The no-observed-adverse-effect-level in drug safety evaluations: Use, issues, and definition(s). Regulatory Toxicology and Pharmacology. 2005;42(3):265-274
Figures
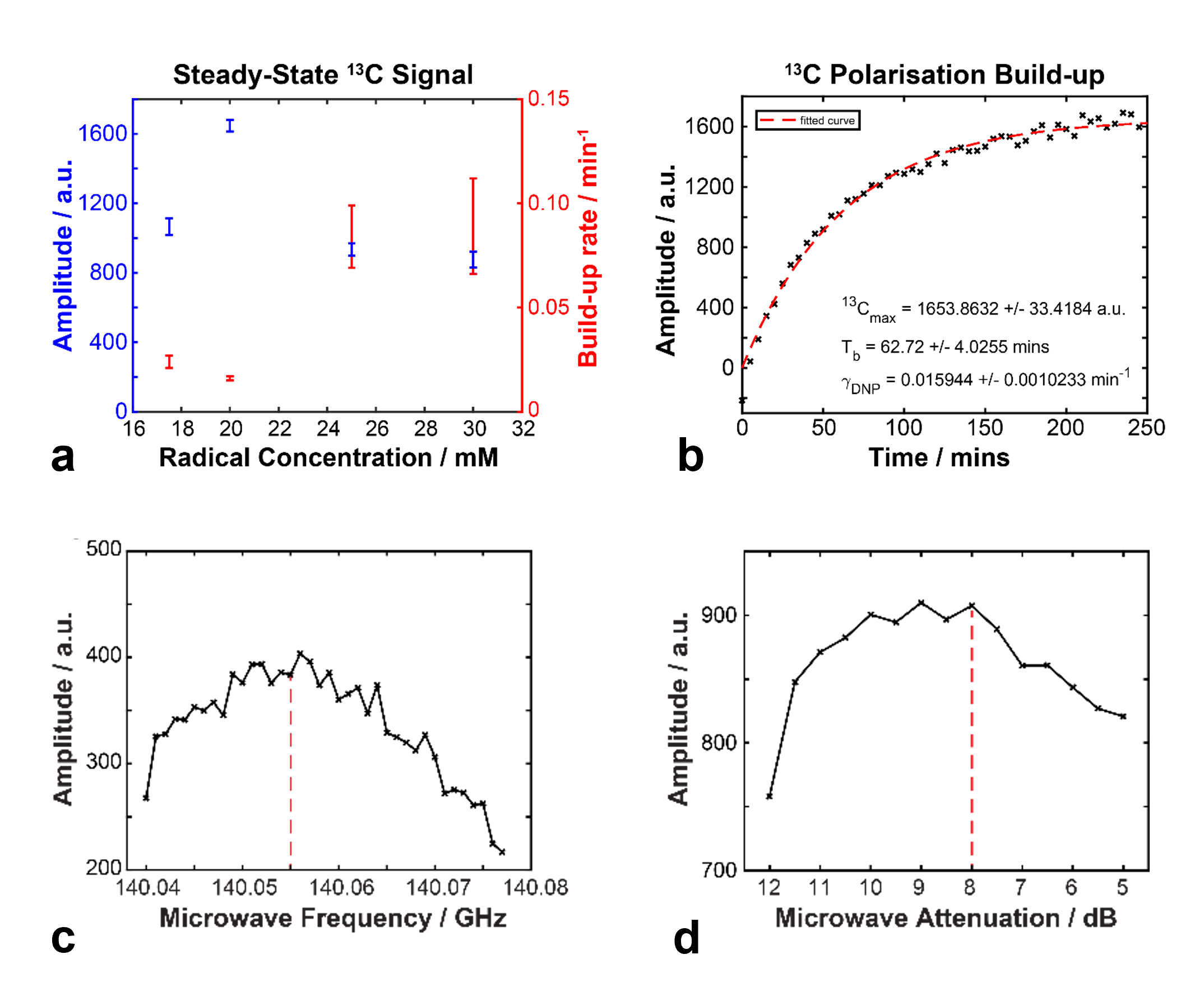
Figure 1
(a) Optimization of EPA (radical) concentration by assessment of the hyperpolarized amplitude and build-up rate.
(b) Exemplary build-up of hyperpolarized state at the optimal found conditions ([EPA] = 20mM, frequency = 140.055GHz, attenuation = 8dB).
(c) Sweep to find the optimal hyperpolarization microwave frequency.
(d) Sweep to find the optimal microwave attenuation.
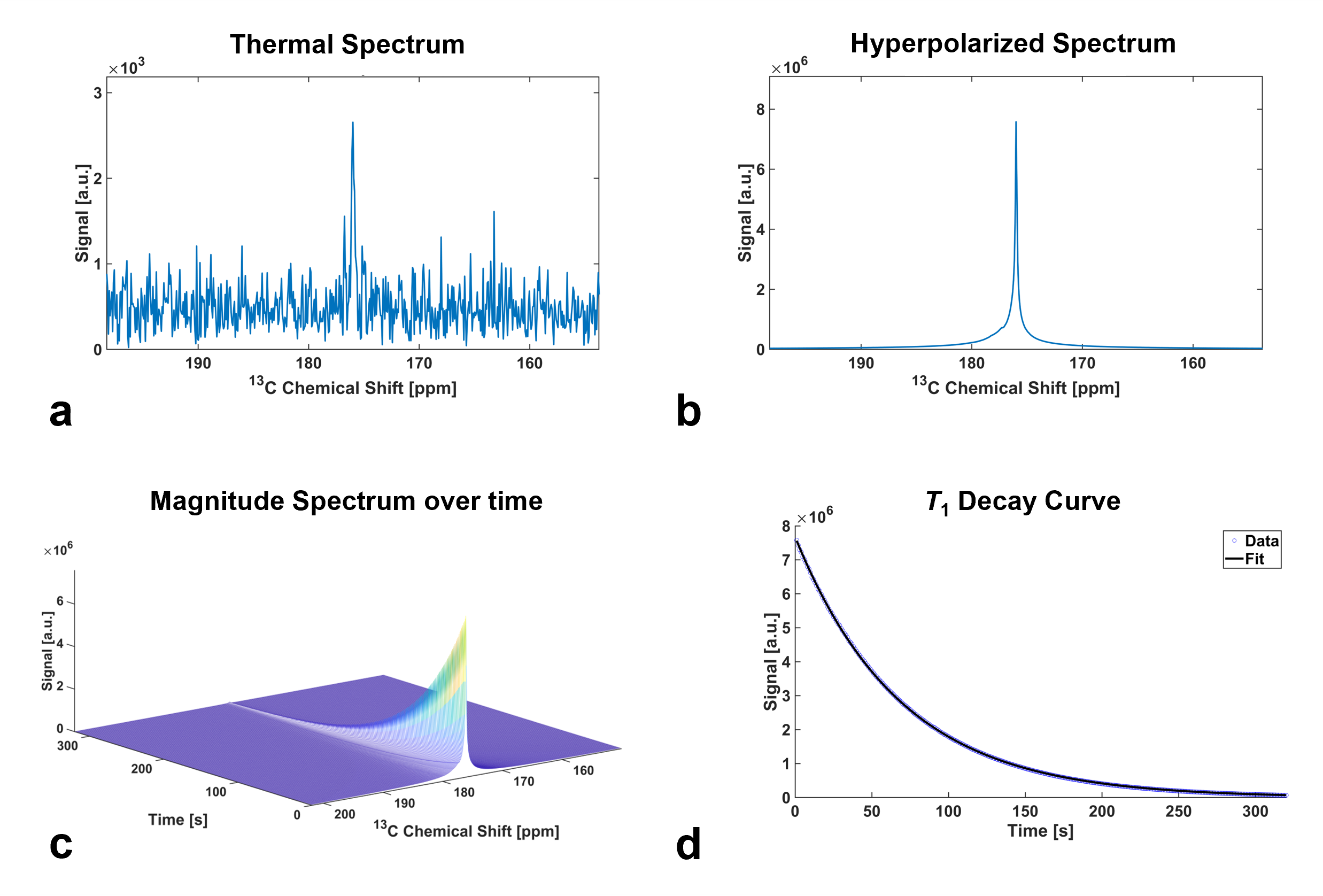
Figure 2
(a) Thermally polarized spectrum of 13C-fumarate acquired after decay of the hyperpolarized state.
(b) Hyperpolarized spectrum of 13C-fumarate after dissolution (time between dissolution and acquisition = 36s).
(c) Exponential decay of hyperpolarized state over time.
(d) Peak data from (c), fitted by a monoexponential decay to yield the T1 relaxation time constant (76s).
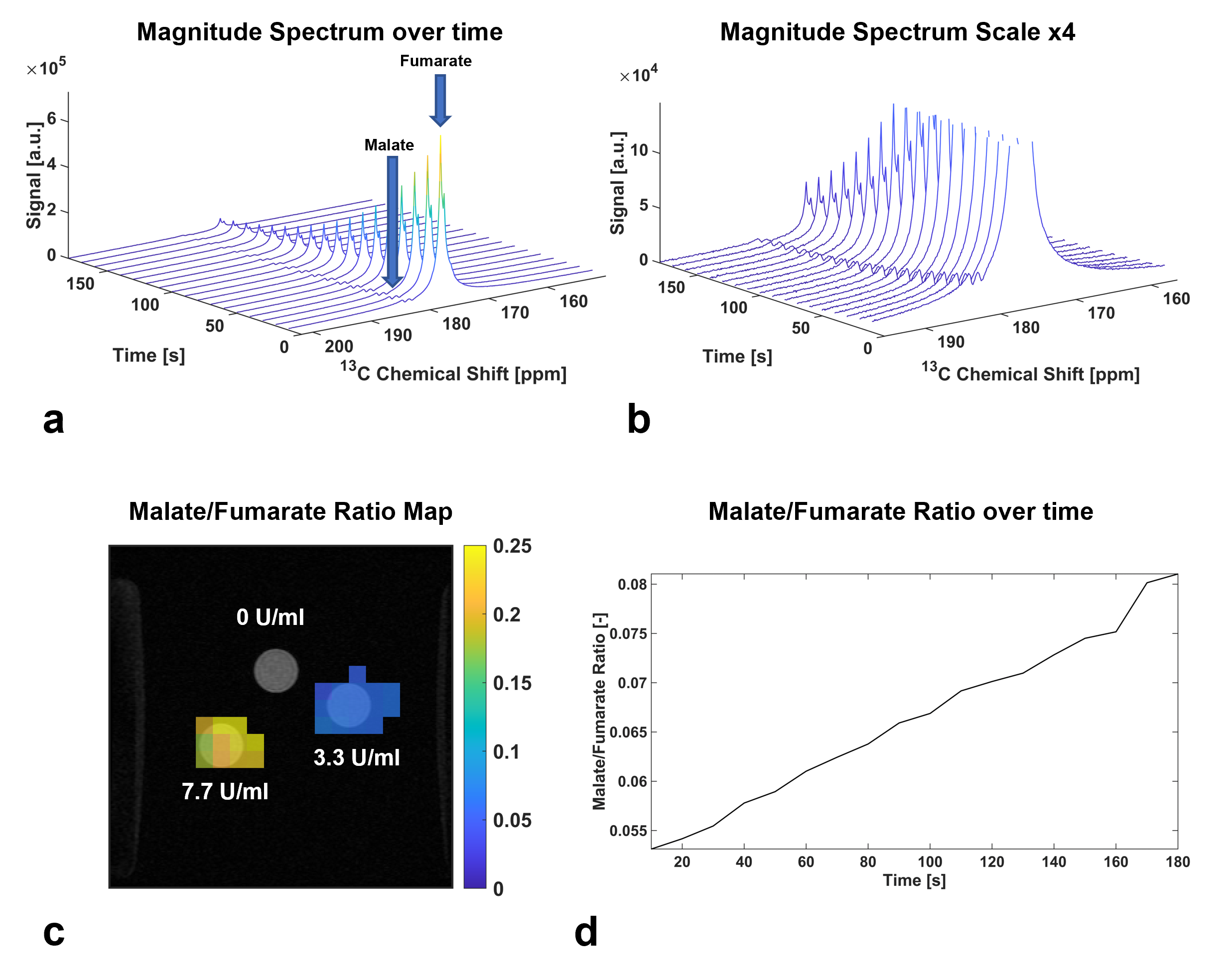
Figure 3
(a) Detection of 13C-fumarate and 13C-malate after adding the converting enzyme fumarase.
(b) Data from (a), scaled up by a factor of 4 for better visibility of the 13C-malate peaks.
(c) A 13C-malate/13C-fumarate ratio map, calculated using Matlab, enables spatial separation of phantoms based on their fumarase content.
(d) An increasing 13C-malate/13C-fumarate ratio during spectroscopy verifies ongoing conversion in the phantoms.
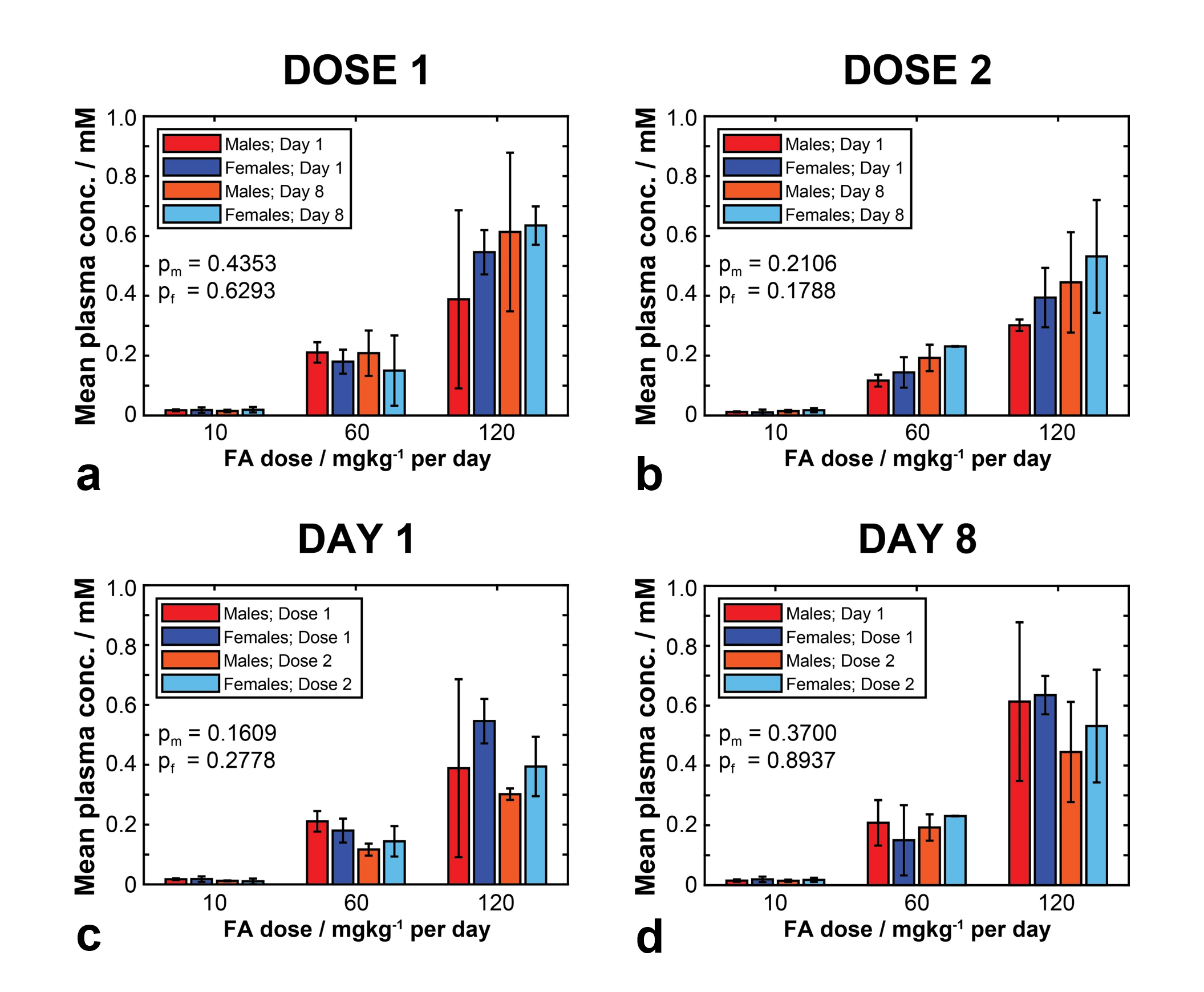
Figure 4
(a) Dose escalation study in rats. Displayed is the mean plasma concentration of 13C-fumarate, after receiving different doses (dose 1).
(b) Mean plasma concentration after receiving a second dose of 13C-fumarate 1h after dose 1. The data suggests rapid return to baseline after receiving dose 1.
(c) and (d) Data from (a), (b), displayed to compare the mean plasma concentration on day 1 and day 8. No significant increase can be seen, suggesting no accumulation of 13C-fumarate.
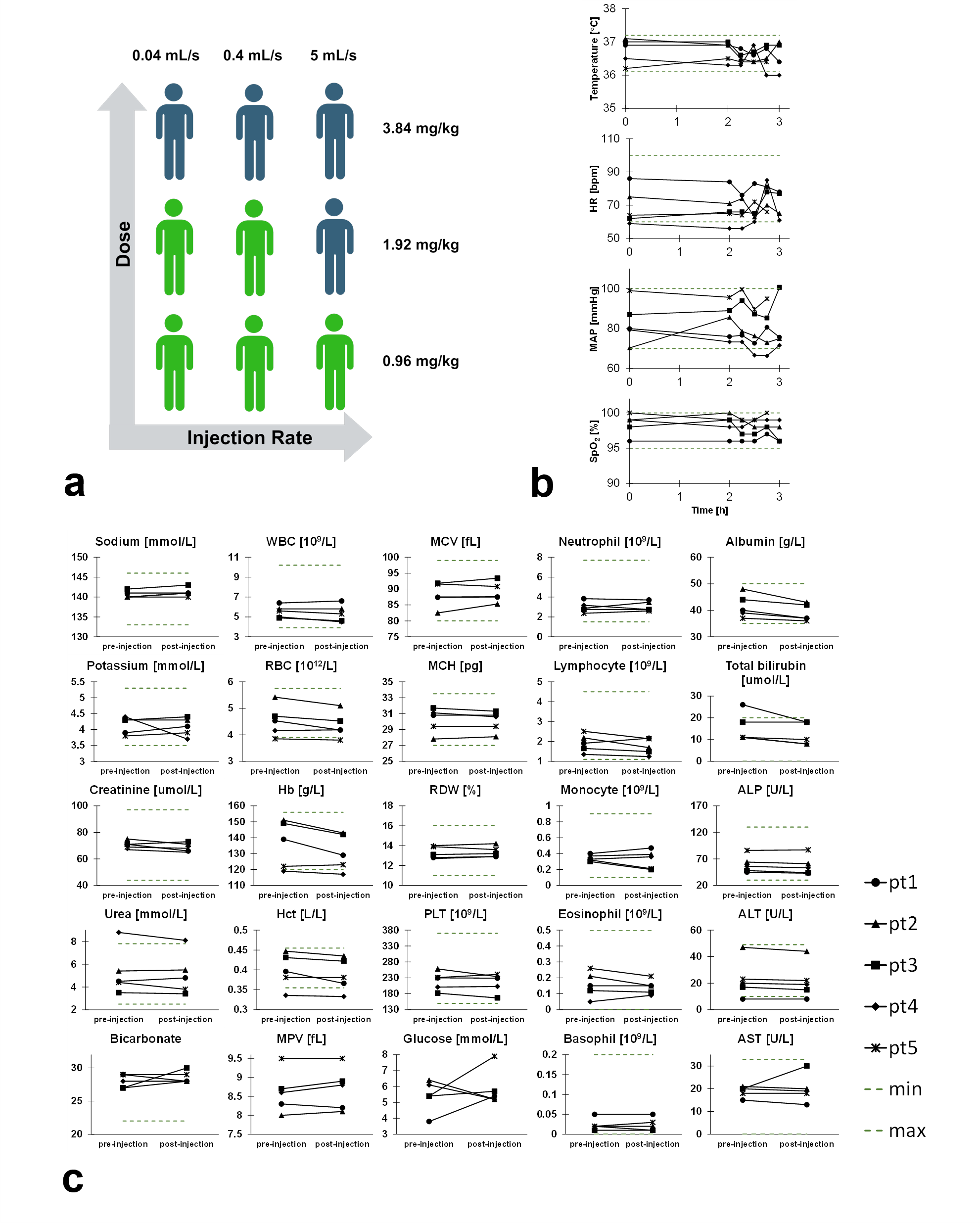
Figure 5
(a) Healthy volunteer injection plan outside of the scanner. Preliminary human administration data presented are indicated by the green human icons, as a proportion of the anticipated healthy human exposure.
(b) Monitored vital parameters pre-and post-injection.
(c) Blood results pre-and post-injection.