0207
The diagnostic performance of time-dependent diffusion MRI in differentiating benign and malignant breast tumors1Key Laboratory for Biomedical Engineering of Ministry of Education, Department of Biomedical Engineering, College of Biomedical Engineering & Instrument Science, Zhejiang University, Hangzhou, China, 2Department of Radiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, China, 3Graduate School of Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China
Synopsis
Keywords: Breast, Tumor, diffusion-time-dependence
Motivation: Diffusion-time-dependent diffusion MRI (td-dMRI) has potential in noninvasive mapping of breast tumor microstructure. However, its diagnostic value in differentiating benign and malignant tumors remains unclear, especially including transcytolemmal water exchange.
Goal(s): To investigate the clinical value of td-dMRI-based microstructural mapping for discriminating benign and malignant breast tumors.
Approach: Time-dependent dMRI data acquired with OGSE and PGSE sequences were estimated with the JOINT models.
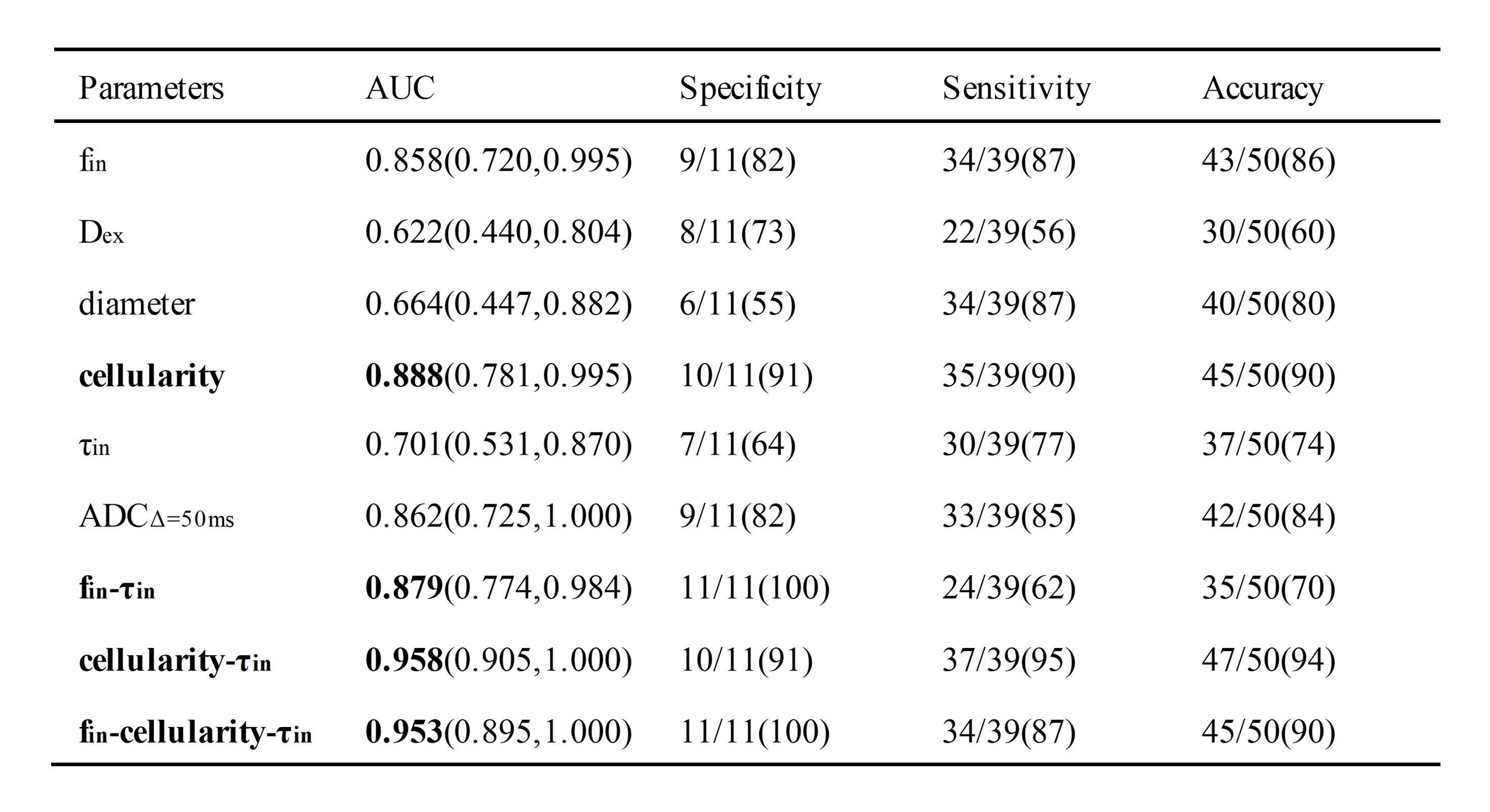
Results: The td-dMRI-based fin, cellularity and τin showed significant group differences between benign and malignant breast tumors. The combination of cellularity and τin indices achieved the highest diagnostic performance, with an accuracy of 94% and AUC of 0.958.
Impact: The diagnostic performance of cellularity-τin obtained from td-dMRI was comparable with or superior to previous studies. The 7.5-minute protocol is translatable to clinical diagnostics.
Introduction
Diffusion MRI (dMRI) based microstructural mapping of tumor microstructure provides a way for non-invasive biopsies[1]. By incorporating the diffusion time dependency with multi-compartment models, we can estimate cellular microstructures such as cell size, cell volume fraction, and transcytolemmal water exchange[2-4]. Previous studies have shown that the td-dMRI-based IMPULSED model can be used to quantify breast tumor microstructures[4], but its diagnostic value is largely unknown. Here we targeted an important clinical task of discriminating benign and malignant breast tumors, in which previous studies using apparent diffusion coefficient only showed moderate accuracy [5-8]. We employed the recently developed JOINT model that improved the IMPULSED model by incorporating water exchange based on a modified Kärger model[9], and characterized the change of cell morphology and transmembrane water exchange in malignant breast tumors.Methods
Study Participants: A total of 50 female patients (11 benign and 39 malignant) with a clinical suspicion of breast lesions were prospectively recruited at the Beijing Hospital from March 2023 to August 2023. Written informed consent was obtained from all participants to undergo td-dMRI in addition to standard-of-care multiparametric MRI. All patients underwent biopsies for clinical diagnosis.Image Acquisition: Breast MRI was performed on a 3-T Siemens Prisma scanner (Skyra, Siemens Healthcare) with a high-performance gradient system (maximum gradient=80 mT/m per axis, maximum slew rate=200 mT/m). An in-house OGSE diffusion MRI sequence was implemented with trapezoid-cosine gradients and echo-planar imaging acquisition. OGSE data were acquired at oscillating frequencies of 50 Hz (tdiff=5 msec, two cycles, b=150 and 300 sec/mm2) and 25 Hz (tdiff=10 msec, one cycle, b=250, 500, 750, and 1000 sec/mm2). PGSE data were acquired at diffusion duration δ of 10 msec, and diffusion separation Δ of 30 msec (tdiff=26.7 msec, b = 250, 500, 750, and 1000 sec/mm2) and 50 msec (tdiff=46.7 msec, b=250, 500, 750, and 1000 sec/mm2). The following parameters were used for both sequences: six diffusion directions; TR/TE= 4500/116 ms; FOV=280×280 mm; in-plane resolution = 2.5×2.5 mm; 10 slices with slice thickness of 5 mm. The entire td-dMRI protocol took approximately 7.5 minutes.
Image Analysis: The td-dMRI data was fitted using the JOINT model in Matlab 2018a. For robust fitting of the intracellular volume fraction fin, extracellular diffusivity Dex, cell diameter d, and cellularity, we used a Bayesian algorithm and fixed the intracellular water pre-exchange lifetime τin. Then we freed τin to obtain the τin map.
Statistical analysis: The microstructural features were averaged over the manually delineated lesion regions of interest. The group differences were compared with an unpaired two-tailed t-test in GraphPad Prism. The diagnostic efficacy was evaluated with sensitivity, specificity, accuracy, and area under the receiver operating characteristic curve (AUC).
Results
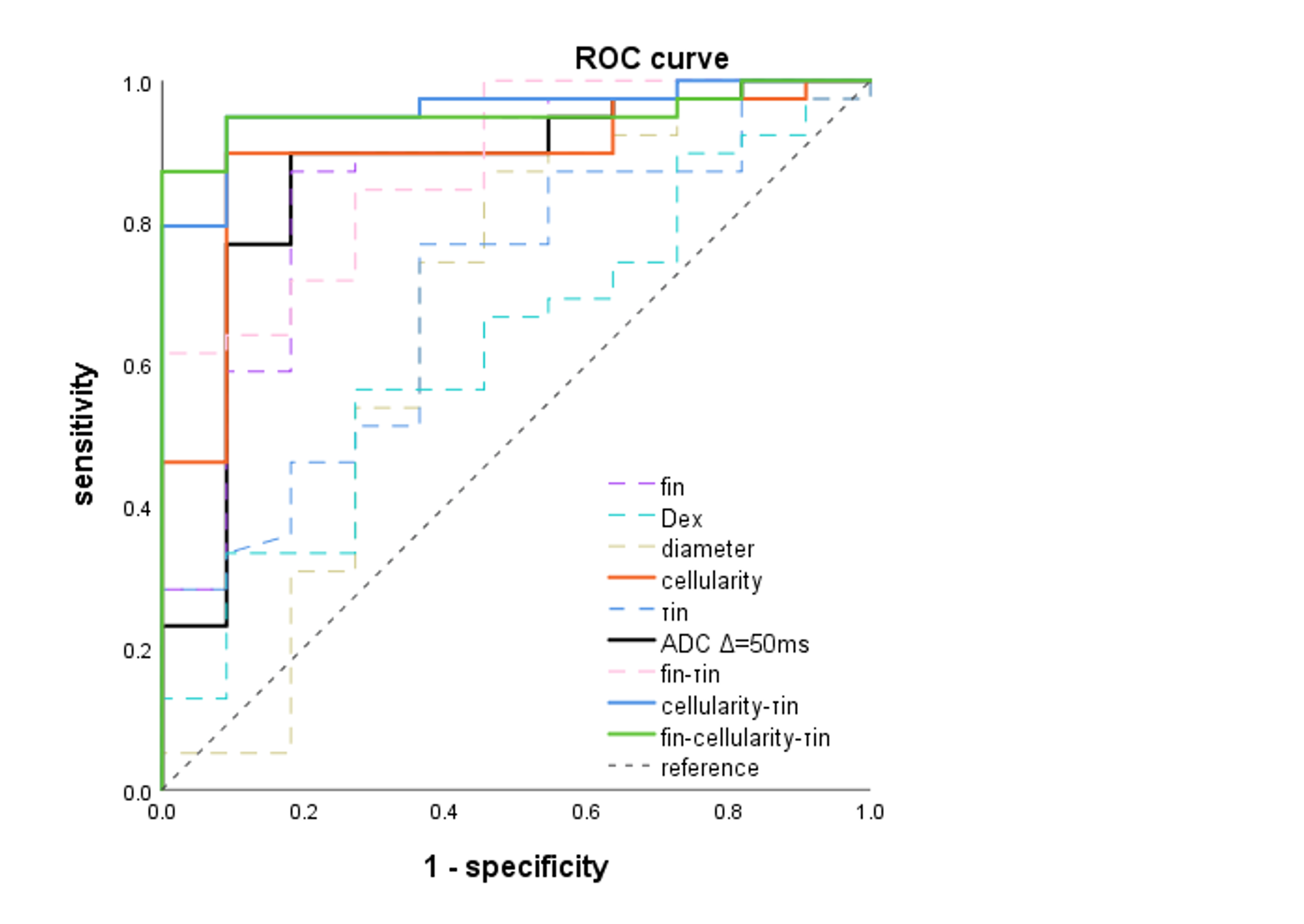
Among the parameters derived from the JOINT models, the fin, cellularity and τin of benign lesions were significantly lower than those of malignant ones, and the ADC was significantly higher (Figure 2). The AUCs of the fin, Dex, d, cellularity, τin and ADC at 50ms were 0.858, 0.622, 0.664, 0.888, 0.701 and 0.862 respectively. We further tested the combination of different parameters using binary Logistic regression in SPSS. The combined parameters with AUC higher than single parameters were: fin-τin, cellularity-τin and fin-cellularity-τin were 0.879, 0.958, and 0.953 respectively, indicating that including τin from the joint model can improve diagnostic performance. The sensitivity, specificity and accuracy were listed in Table 1. Receiver Operating Characteristic (ROC) curve of these parameters is shown in Figure 3.Discussion and Conclusion
In this study, the time-dependent diffusion MRI technique was proposed to assess the microstructure of breast lesions. In malignant lesions, the cell density was larger and the diffusion was more restricted than that in benign lesions, so fin, cellularity and τin in the cancerous tissues were higher, and Dex was lower. The microstructural parameters and their combinations outperformed ADC-based diagnosis, especially, the cellularity-τin achieved an AUC up to 0.958. The diagnostic performance was comparable with or superior to previously reported accuracies of conventional dMRI or other microstructural studies of breast tumors[10,11], indicating the clinical potential of these translatable new markers.Acknowledgements
This work is supported by the National Natural Science Foundation of China (81971606, 82122032), and Science and Technology Department of Zhejiang Province (2022C03057, 202006140).References
[1] Paepke S, Metz S, Salvago A B, et al.Benign Breast Tumours - Diagnosis and Management[J].Breast Care,2018, 13 (6): 403-412.
[2] Stepisnik J.TIME-DEPENDENT SELF-DIFFUSION BY NMR SPIN-ECHO[J].Physica B,1993, 183 (4): 343-350.
[3] Reynaud O.Time-Dependent Diffusion MRI in Cancer: Tissue Modeling and Applications[J].Frontiers in Physics,2017, 5.
[4] Xu J, Jiang X, Li H, et al.Magnetic resonance imaging of mean cell size in human breast tumors[J].Magnetic Resonance in Medicine,2020, 83 (6): 2002-2014.
[5] Tezcan S, Uslu N, Ozturk F U, et al.Diffusion-Weighted Imaging of Breast Cancer: Correlation of the Apparent Diffusion Coefficient Value with Pathologic Prognostic Factors[J].European Journal of Breast Health,2019, 15 (4): 262-267.
[6] Wu P, Cui L, Guo B H, et al.Values of Minimal Apparent Diffusion Coefficient,Difference between Ratios of Apparent Diffusion Coefficients,and Dynamic Contrast-enhanced Magnetic Resonance Imaging Features in Diagnosing Breast Ductal Carcinoma In Situ with Microinvasion[J].Zhongguo yi xue ke xue yuan xue bao. Acta Academiae Medicinae Sinicae,2019, 41 (6): 737-745.
[7] Iima M, Honda M, Sigmund E E, et al.Diffusion MRI of the breast: Current status and future directions[J].Journal of Magnetic Resonance Imaging,2020, 52 (1): 70-90.
[8] Demartini W, Lehman C.A review of current evidence-based clinical applications for breast magnetic resonance imaging[J].Topics in magnetic resonance imaging: TMRI,2008, 19 (3): 143-50.
[9] Jiang X, Devan S P, Xie J, et al.Improving MR cell size imaging by inclusion of transcytolemmal water exchange[J].Nmr in Biomedicine,2022, 35 (12).
[10] Tsvetkova S, Doykova K, Vasilska A, et al.Differentiation of Benign and Malignant Breast Lesions Using ADC Values and ADC Ratio in Breast MRI[J].Diagnostics,2022, 12 (2).
[11] Gao Y, Wang Y, Zhang H, et al.The outstanding diagnostic value of DKI in multimodal magnetic resonance imaging for benign and malignant breast tumors: A diagnostic accuracy study[J].Medicine,2023, 102 (40).
Figures
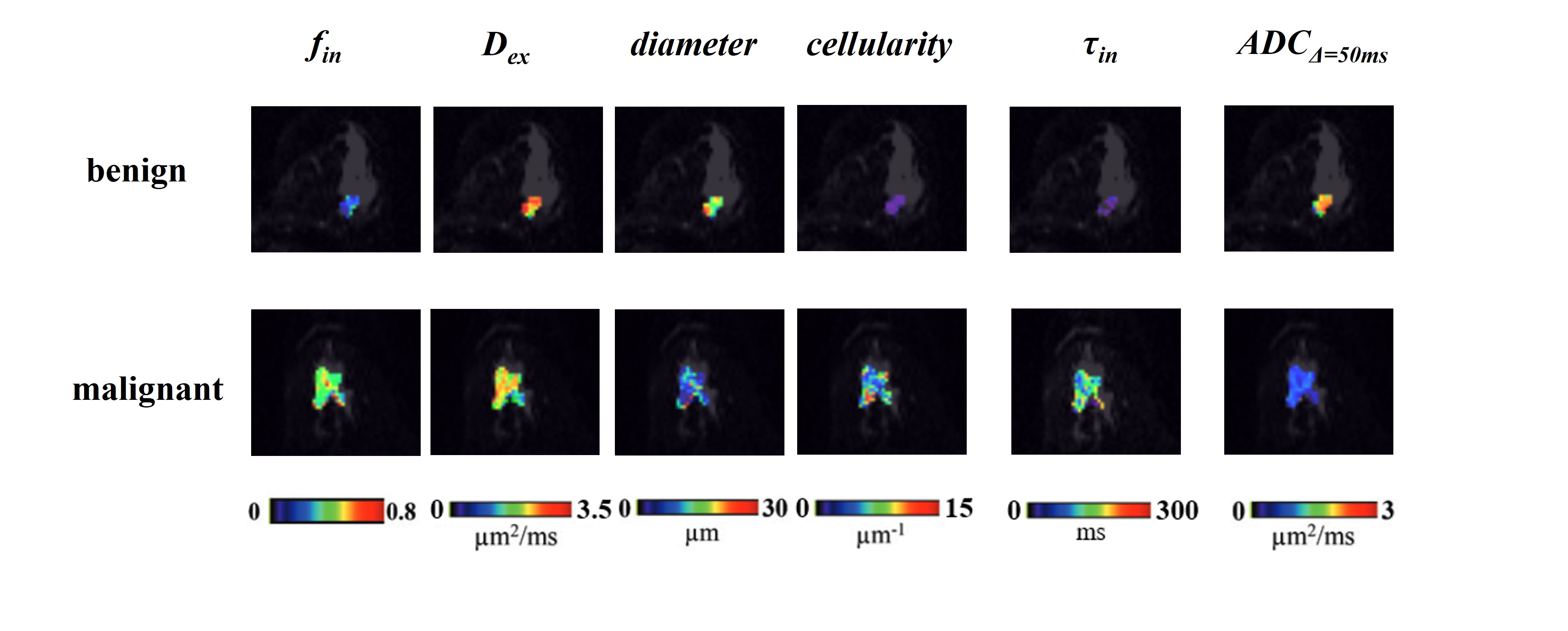
Figure 1. Microstructural maps of benign and malignant tumors, including the intracellular volume fraction fin, cell diameter, cellularity, extracellular diffusivity Dex, and intracellular water pre-exchange lifetime τin fitted from JOINT model and the diffusivity maps from pulsed gradient spin-echo (Δ=50ms) data.
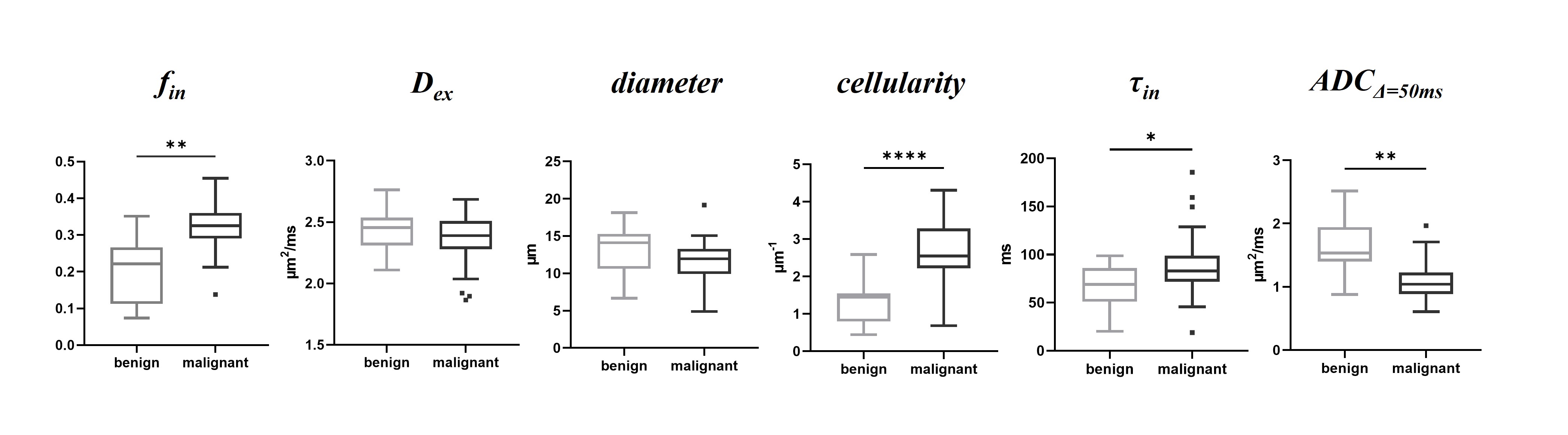
Figure 2. Group differences between benign and malignant breast tumors in terms of fin, Dex, diameter, cellularity, τin and ADCΔ=50ms. * = P <.05. Whiskers denote the range in each group (with the Tukey method), boxes indicate the SD, and midlines are the median.