0201
Estimating diffusion fractional anisotropy of disease in patients with advanced prostate and breast cancers. A single-center study.1Institute of Cancer Research, London, United Kingdom, 2Fondazione Policlinico Universitario Agostino Gemelli, Rome, Italy, 3The Royal Marsden NHS Foundation Trust, London, United Kingdom
Synopsis
Keywords: Cancer, Whole Body, Metastasis, Fractional Anisotropy
Motivation: Whole-body diffusion-weighted imaging in oncology assumes isotropic diffusion therefore that data probing the directional dependence of diffusion in body cancer applications is scarce.
Goal(s): To report the distribution of fractional anisotropy (FA) values in metastatic bone disease for a cohort of patients who underwent multi-directional diffusion weighted imaging.
Approach: Deep learning was used to auto-segment metastatic lesions; FA values are calculated for each segmented region and the distributions reported.
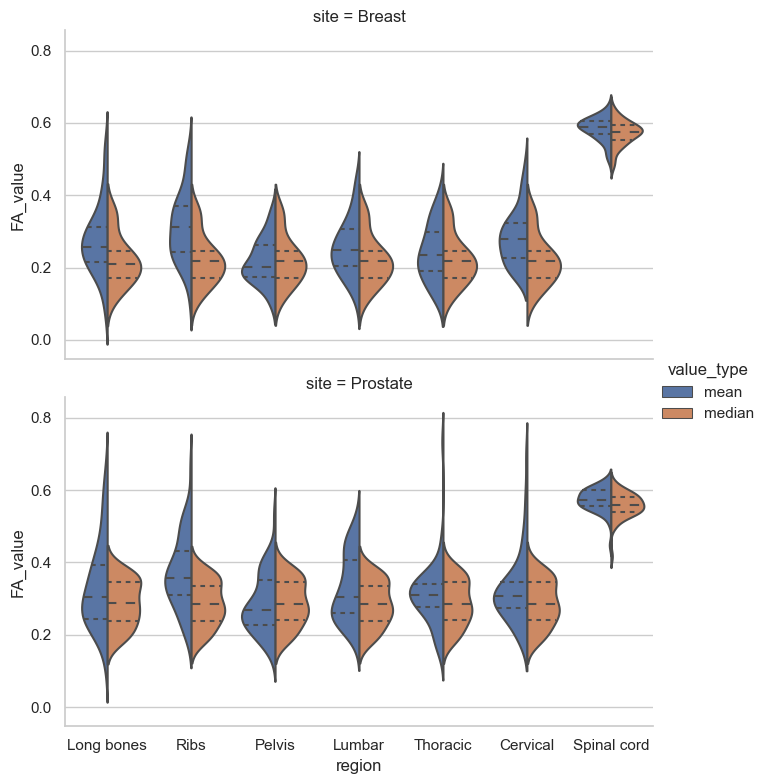
Results: FA distributions from 85 patients with metastatic disease (50 prostate, 33 breast) are reported and are deemed to be low (mean FA range breast group: 0.2179 - 0.3132; prostate group: 0.2866 - 0.3717).
Impact: We have conducted diffusion tensor imaging analysis for whole body DWI data and carried out the first bone lesion FA comparison study. This work provides a rationale for choice of diffusion-weighting gradient schemes in clinical imaging.
Background
It is often assumed in whole-body diffusion-weighted imaging (WB-DWI) of cancer that the diffusion of water molecules is isotropic and there is therefore no directional dependence of derived measures of apparent diffusion coefficient (ADC)1. This assumption often governs the selection of clinical diffusion-encoding gradient schemes that do not probe the directionality of diffusion in-vivo in favour of increasing signal-to-noise ratio using fewer gradient directions (e.g., 3 orthogonal directions in atrace weighed scan or even a single direction)2. Unfortunately, this means that data probing the directional dependence of diffusion in body cancer applications is scarce as at least 6 diffusion encoding directions are required for calculation of the underlying diffusion tensor and derived parameters including the fractional anisotropy (FA). Here we report on initial findings in a unique cohort of patients who underwent whole-body multi-directional diffusion-weighted (MDDW) imaging including six gradient directions. Our aim was to describe the distribution of FA values found in regions of metastatic bone disease, as delineated using an automated tumour segmentation pipeline.Methods
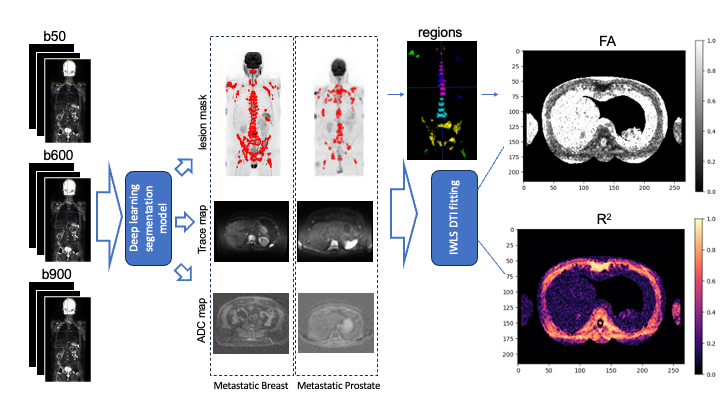
A total of 83 patients underwent a whole-body MDDW scan as part of a single center prospective clinical trial (NCT05380609). 50 and 33 patients had confirmed metastatic disease from prostate and breast cancer respectively. Images were acquired on a 1.5T MAGNETOM Aera / Sola system, at three b-values, 50, 600 and 900 s/mm2, with the number of averages set to 2, 2, and 3 respectively, each with the same six diffusion encoding gradient directions: [0, -1, +1], [0, -1, -1], [+1, 0, -1], [-1, 0, -1], [+1, -1, 0], and [-1, -1, 0](after normalisation) 3. All images were acquired using 40 slices per station (5mm slice thickness) acquired over 5 stations for prostate cancer, 4-6 stations for breast cancer. Iterative weighted least square (IWLS) 4,5 was used for estimating the full diffusion tensor at each voxel location, from which estimates of FA are subsequently derived (data variance and goodness-of-fit $$$R^{2}$$$ are also reported after model fitting). IWLS model fitting was performed using custom code in python.A recently developed and validated deep learning tool6 for segmenting bone lesions in patients with advanced prostate cancers was used to extract FA values from within regions of metastatic bone disease (Figure 1). The method provides delineation of disease segmented into six skeletal regions: pelvis, lumbar spine, thoracic spine, cervical spine, ribs, and long bones in about one minute. Furthermore, the tool can automatically delineate the spinal cord and surrounding CSF. The average FA from each region was derived and compared to the FA of the spinal cord.
Results
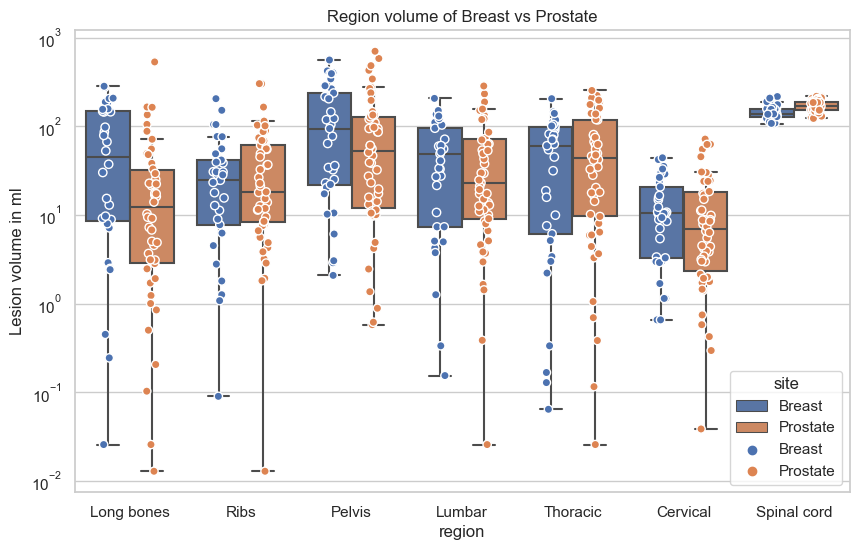
Violin plots of FA are presented in Figure 2 for both prostate and breast cancer patients in all delineated regions. The spinal cord contains a significantly higher FA value distribution compared with tumour regions that is in line with the literature7. Furthermore, the distribution of disease volumes delineated by the tool is presented in Figure 3.Discussion
Our results indicate that bone lesions within the skeleton generally exhibit low FA values, which is in line the current philosophy surrounding the measurement of ADC is whole-body disease. Using automated deep-learning segmentation, in combination with our unique datasets, it is possible to better characterise the delineated bone lesions with DTI and help probe deeper into the underlying biological microenvironment for whole-body diffusion images. In addition, our experiments confirmed that IWLS gives stable estimates diffusion tensor coefficients as they do not deviate with increased number of iterations8. $$$R^{2}$$$ is generated together with the FA map to show how well each linear model is fitted for each voxel. Low $$$R^{2}$$$ values indicate the uncertainty of high FA value in liver in Figure 1. Further work will focus on the determining whether the FA values found in this cohort of patients indicate that bias might be expected when measuring ADC using a single diffusion encoding direction scheme over a trace-weighted imaging scheme.Conclusion
We have conducted diffusion tensor imaging analysis for whole body DWI data and carried out the first bone lesion FA comparison study. This pilot work will enable us to investigate quantitative imaging markers for whole-body data with the help of automated segmentation tools.Acknowledgements
This study represents independent research funded by the National Institute for Health and Care Research (NIHR) Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, London, and by the Royal Marsden Cancer Charity. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.References
1. Koh, D. M., & Collins, D. J. (2007). Diffusion-weighted MRI in the body: applications and challenges in oncology. American Journal of Roentgenology, 188(6), 1622-1635.Baliyan V, Das CJ, Sharma R, Gupta AK. Diffusion weighted imaging: Technique and applications. World J Radiol. 2016 Sep 28;8(9):785-798.
2. Le Bihan D, Mangin JF, Poupon C, Clark CA, Pappata S, Molko N, Chabriat H. Diffusion tensor imaging: concepts and applications. J Magn Reson Imaging. 2001 Apr;13(4):534-46.
3. Salvador R, Peña A, Menon DK, Carpenter TA, Pickard JD, Bullmore ET. Formal characterization and extension of the linearized diffusion tensor model. Hum Brain Mapp. 2005 Feb;24(2):144-55.
4. Collier Q, Veraart J, Jeurissen B, den Dekker AJ, Sijbers J. Iterative reweighted linear least squares for accurate, fast, and robust estimation of diffusion magnetic resonance parameters. Magn Reson Med. 2015 Jun;73(6):2174-84.
5. Candito, A.; Blackledge, M. D.; Holbrey, R.; Koh, D.-M. Automated Tool to Quantitatively Assess Bone Disease on Whole-Body Diffusion Weighted Imaging for Patients with Advanced Prostate Cancer. In Medical Imaging with Deep Learning; 2022.
6. Duval, T.; Lévy, S.; Stikov, N.; Campbell, J.; Mezer, A.; Witzel, T.; Keil, B.; Smith, V.; Wald, L. L.; Klawiter, E.; Cohen-Adad, J. G-Ratio Weighted Imaging of the Human Spinal Cord in Vivo. NeuroImage 2017, 145, 11–23. https://doi.org/https://doi.org/10.1016/j.neuroimage.2016.09.018.
7. Veraart J, Sijbers J, Sunaert S, Leemans A, Jeurissen B. Weighted linear least squares estimation of diffusion MRI parameters: strengths, limitations, and pitfalls. Neuroimage. 2013 Nov 1;81:335-346.
Figures