0197
Intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) of pancreas for assessment of β-cell dysfunction in hyperglycemia1Department of Medical Imaging,, Guangdong Second Provincial General Hospital, Guangzhou, China, 2Department of Radiology, Affiliated Hospital of Jianghan University, Wuhan, China
Synopsis
Keywords: Endocrine, Pancreas, Type 2 diabetes mellitus
Motivation: Early detection of damaged β-cell function may help timely protect and stop the progression of hyperglycemia to type 2 diabetes mellitus (T2DM). The impaired β-cell function may be associated with damaged pancreatic microstructure.
Goal(s): The pancreatic microstructural changes may serve as the biomarker for β-cell dysfunction.
Approach: We evaluate the microstructural changes of the pancreas in patients with hyperglycemic employing intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) and explore its correlation with the β-cell function.
Results: IVIM-DWI can effectively distinguish T2DM from hyperglycemia, it has the potential for identifying damaged b-cell function for patients with early-stage hyperglycemia but without obvious clinical manifestation of DM.
Impact: IVIM-DWI of pancreases is a reliable and non-invasive tool with great potential in detecting the early damaged β-cell function when the DM is still in the insidious stage, and help for improving diabetes diagnosis and management.
Background and Purpose
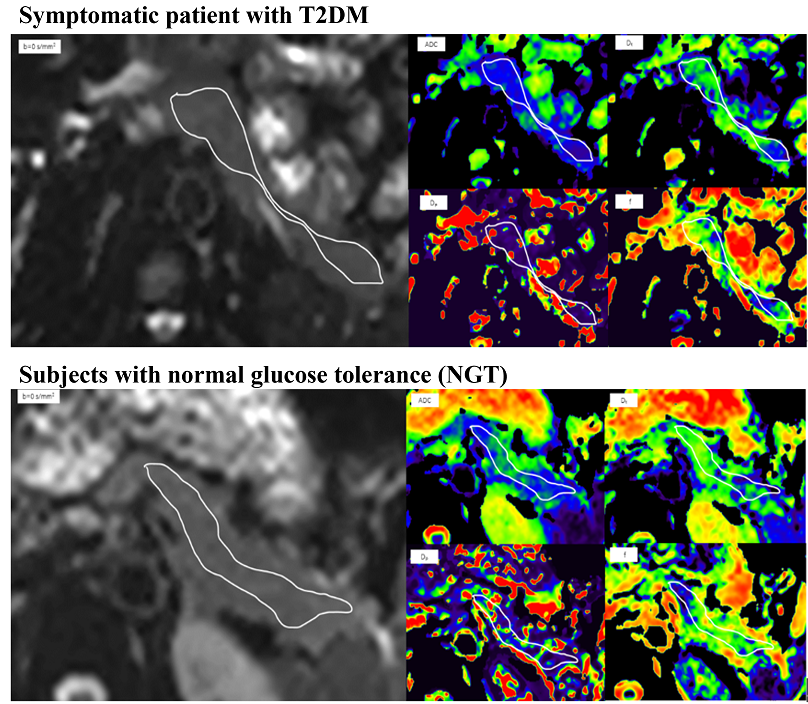
Diabetes mellitus (DM) is a chronic progressive disease that shows insulin resistance, and with or without β-cell dysfunction. However, the β-cell function of most patients with DM is approximately 50% impaired at time of diagnosis, and probably commences 10–12 years before diagnosis[1]. Additionally, the subsequent treatment regimen and its effectiveness are closely related to patients’ remaining β-cell function[2]. Routine hematology tests, which are used as biomarkers to initiate clinical intervention for hyperglycemia[3], often ignore early β-cell dysfunction in patients, delaying prevention and treatment. Thus, early detection of the occult histopathologic alteration of the pancreatic parenchymal texture may facilitate the timely identification of β-cell dysfunction and prevent progression to irreversible hyperglycemia eventually. The pancreatic histopathology of patients with hyperglycemia is very complex and characterized by steatosis, fibrosis, inflammation, islet amyloid increase, and microcirculation disturbance[4-6]. Intro-voxel incoherent motion diffusion-weighted imaging (IVIM-DWI), a spin-off technology of DWI, can evaluate not only the pure water diffusion but also the capillary perfusion, reflecting the microstructure and the microcirculation in the vivo tissues, respectively[7]. We aim to in utilize IVIM-DWI to produce a new set of imaging markers for the early detection of the microstructure and microcirculation changes and the β-cell dysfunction in the pancreas of hyperglycemic patients in order to impel early prevention.Materials and Methods:
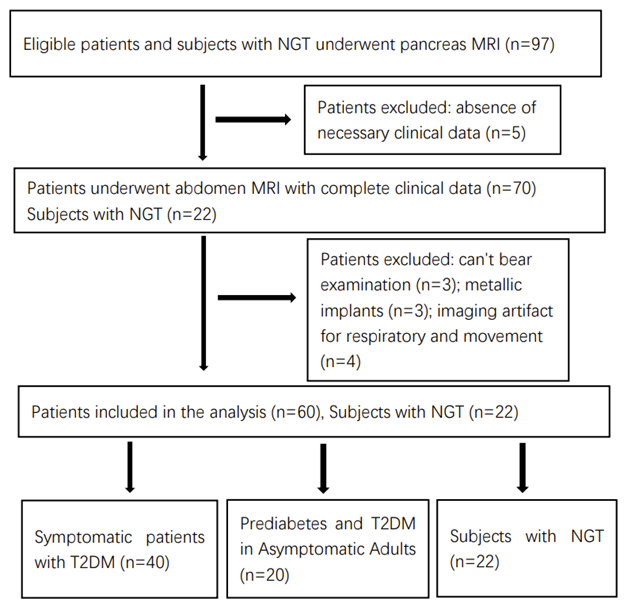
Our study included 60 hyperglycemic patients and 22 healthy controls. IVIM-DWI and the blood examination were performed, and calculated the β-cell function indexes. We divided patients into three grades according to diagnostic criteria, prediabetes (n= 10), T2DM diagnosed by isolated 2-h glucose increasing (n= 10), T2DM diagnosed by fasting and 2-h glucose increasing simultaneously (n= 40), and compared them with healthy controls. We observed the relationship between the imaging parameters with the β-cell function indexes and the diagnostic performance of the parameters for the grades of hyperglycemia.Results:
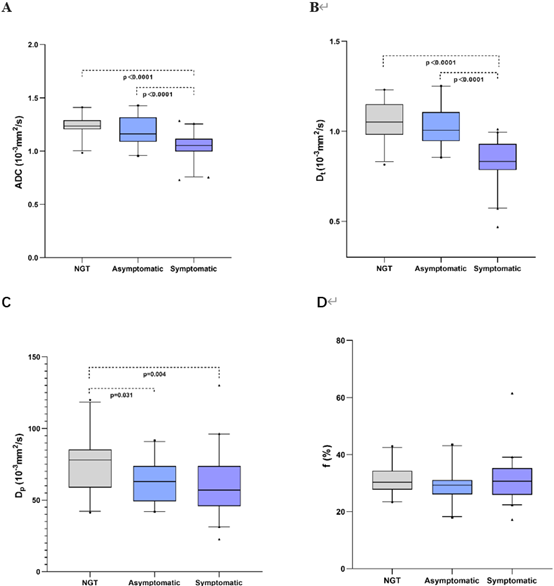
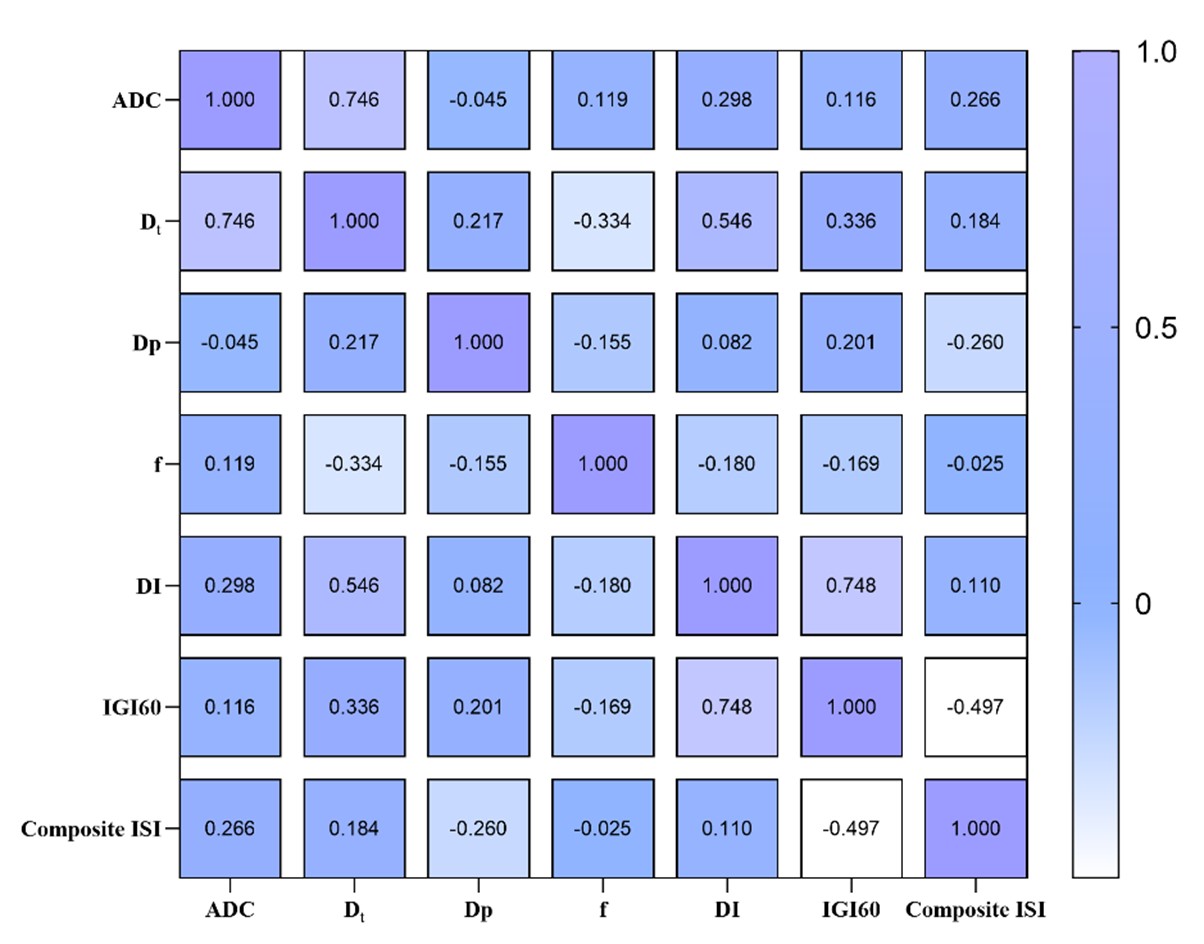
The imaging parameters of ADC, Dt, and Dp gradually decreased among the groups, and the significant difference existed of them: ADC (p< 0.0001), Dt (p< 0.0001), Dp (p= 0.013). The optimal diagnostic performance of the parameters for differentiating the grades of hyperglycemia was Dt. There were some correlations between imaging metrics with β-cell function indexes (p< 0.05).Discussion
Early detection of damaged β-cell function may help provide timely protection and stop the final progression of patients with hyperglycemia to T2DM. We applied the parameters of IVIM as a noninvasive imaging marker to assess microstructural alterations in the pancreas of hyperglycemic patients and identify the grade of hyperglycemia. This study demonstrated that: 1) a progressively decreasing trend in the values of ADC, Dt, and Dp can manifest as hyperglycemia progresses; 2) IVIM metrics of the pancreas revealed good diagnostic performance for differentiating the grades of hyperglycemia; and 3) IVIM parameters are correlated with some indices of β-cell function.In our study, the imaging metrics of ADC, Dt, and Dp gradually decreased among the three groups with successive progress, which coincides with the previous viewpoint that β-cell dysfunction is a long and progressive process and provides visual evidence for the process. The ADC value is significantly reduced in patients with T2DM; thus, we assume that the pancreatic parenchymal texture and component had already changed in these patients because a lower ADC is deemed to the motion of water molecules be restricted[8], which mechanism is higher density of cellularity results in an increase in the density of cell membranes[9]. The difference in Dt among the three groups is also obvious; thus, the restriction of molecular diffusion may be considered one of the factors influencing the function of pancreatic cells, including islet cells.The decrease in Dp was thought to be linked to increased collagen fibril deposition[33],Dp was the only parameter able to differentiate the NGT and PRE+T2DM2h group in our study. Thus, it is likely that the decrease in parenchymal perfusion in the pancreas may have already appeared in the early stages.Thus, Dp can be used as an imaging marker to identify poor microcirculation in pancreatic tissue of hyperglycemic patients.
Conclusion
IVIM-DWI measurements can effectively detect the microstructure and microcirculation changes of the pancreas, which also can effectively distinguish T2DM form hyperglycemia. It may be a promising, noninvasive method for identifying the damaged b-cell function especially for patients with early-stage hyperglycemia but without obvious clinical manifestation or history of DM. And this could facilitate to timely prevent and effectively manage the T2DM.Acknowledgements
We thank all of the participants and the Open Fund of National Innovation Center for advanced medical devices (grant NMED202120-01-002)References
1.Holman RR (1998) Assessing the potential for alpha-glucosidase inhibitors in prediabetic states. Diabetes Res Clin Pract 40 Suppl:S21-25
2.Taylor R, Al-Mrabeh A, Zhyzhneuskaya S et al (2018) Remission of Human Type 2 Diabetes Requires Decrease in Liver and Pancreas Fat Content but Is Dependent upon Capacity for β Cell Recovery. Cell Metab 28:547-556.e543
3. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 45:S17-s38
4.Rickels MR, Norris AW, Hull RL (2020) A tale of two pancreases: exocrine pathology and endocrine dysfunction. Diabetologia 63:2030-2039
5.Westermark P, Andersson A, Westermark GT (2011) Islet amyloid polypeptide, islet amyloid, and diabetes mellitus. Physiol Rev 91:795-826
6.Guadarrama-López AL, Valdés-Ramos R, Martínez-Carrillo BE (2014) Type 2 diabetes, PUFAs, and vitamin D: their relation to inflammation. J Immunol Res 2014:860703
7.Le Bihan D, Breton E, Lallemand D, Aubin ML, Vignaud J, Laval-Jeantet M (1988) Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 168:497-505
8.Lyng H, Haraldseth O, Rofstad EK. Measurement of cell density and necrotic fraction in human melanoma xenografts by diffusion weighted magnetic resonance imaging. Magn Reson Med 2000;43(6):828-36.
9.Szafer A, Zhong J, Gore JC. Theoretical model for water diffusion in tissues. Magn Reson Med 1995;33(5):697-712.
10.Li YT, Cercueil JP, Yuan J, Chen W, Loffroy R, Wang YX. Liver intravoxel incoherent motion (IVIM) magnetic resonance imaging: a comprehensive review of published data on normal values and applications for fibrosis and tumor evaluation. Quant Imaging Med Surg 2017;7(1):59-78.
Figures