0178
A combined T2* weighted gradient echo and 1D quantitative flow sequence for investigating placental function1The Sir Peter Mansfield Imaging Centre, The University of Nottingham, Nottingham, United Kingdom, 2The School of Medicine, The University of Nottingham, Nottingham, United Kingdom, 3Biomedical Research centre, Hospital NHS Trust, The National Institute for Health Research, Nottingham, United Kingdom
Synopsis
Keywords: Placenta, Placenta, Quantitative flow
Motivation: Both oxygenation and blood flow are key measures of placental function; if we could dynamically, and simultaneously measure T2* and flow we could investigate placental function over time.
Goal(s): To Implement and test a gradient echo, quantitative flow sequence with EPI readout in the placenta.
Approach: 4 participants were scanned at 3T using the sequence, and the T2* and velocity maps produced were investigated.
Results: The T2* weighted image retained sufficient contrast, and the quantitative flow was repeatable across subjects, measuring similar velocities in the placenta (<0.1cm/s) that has previously been measured with MRI.
Impact: This sequence has promise for dynamically investigating placental function, simultaneously providing information about oxygenation and blood flow. This will allow us to evaluate placental function in compromised pregnancies over time, and investigate the role of placental contractions.
Introduction
Key measures of placental function include the oxygen distribution, as well as the maternal blood circulation between the villous trees, and fetal flow within the villous trees enabling exchange between the blood pools. T2* is sensitive to oxygenation within the placenta and can differentiate between healthy and compromised placentas using gradient echo sequences such as EPI [1]. In a gradient echo the phase data (which is actually sensitive to the magnetic susceptibility) are often ignored. However it is possible to add a 1D flow quantification lobe to EPI, so that the sequence can provide both a magnitude T2* weighted image as well as a quantitative map of flow. Since EPI can be run dynamically this opens up the possibility of studying dynamic changes in blood flow over time.The aim of this abstract is to apply this sequence in healthy pregnant volunteers and analyse the results to test the feasibility of this sequence.
Method
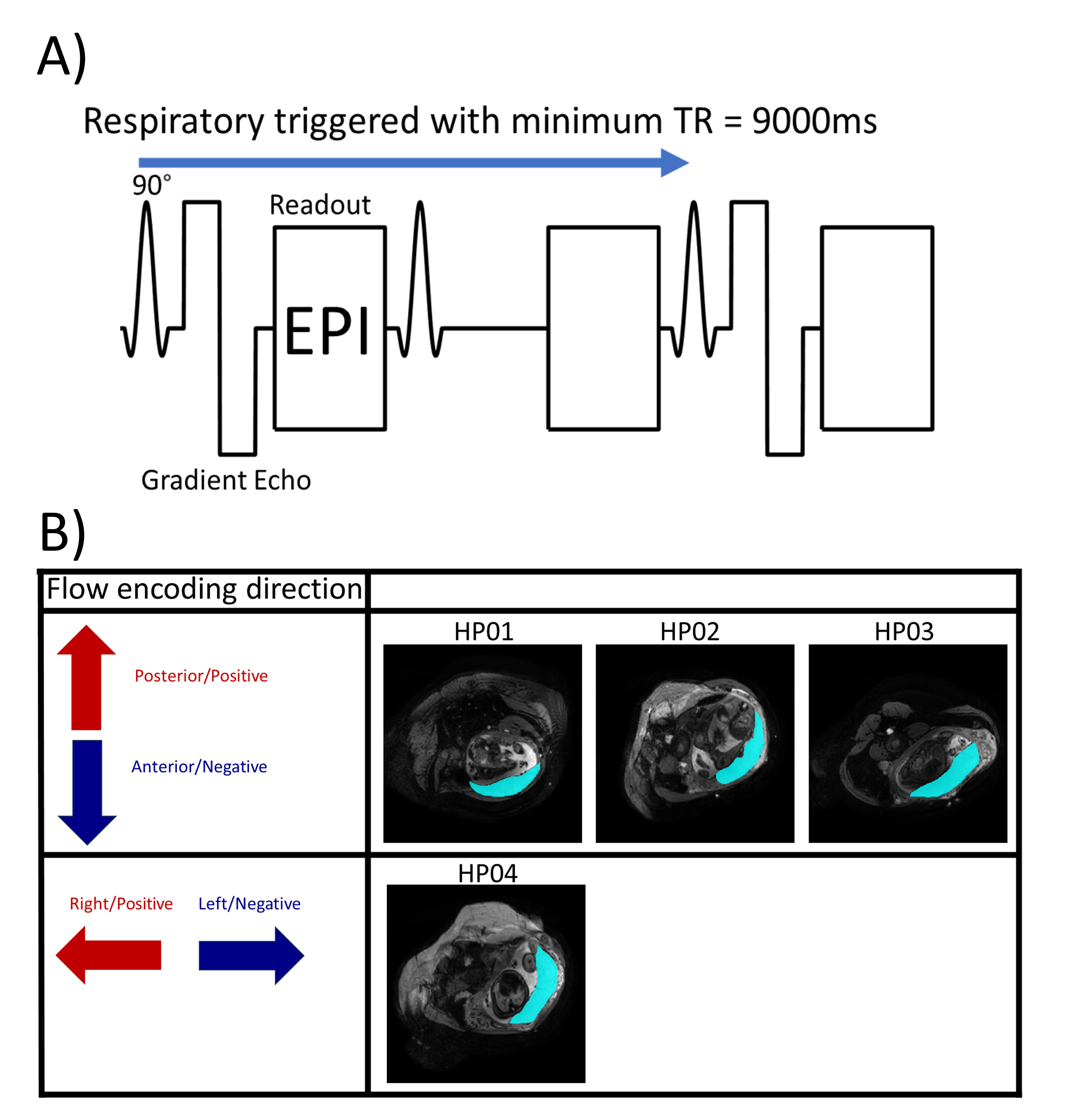
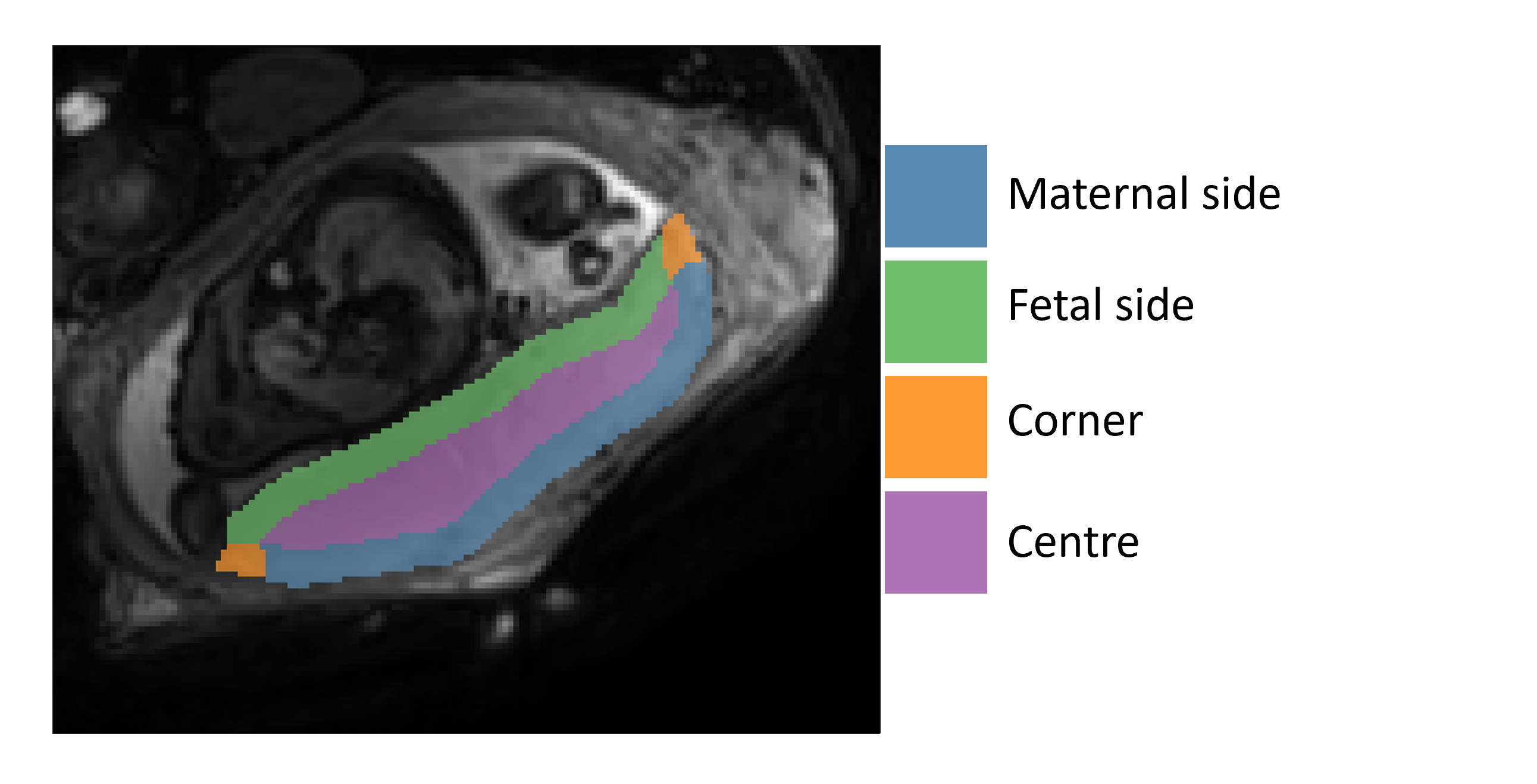
Ethics approval for this study was obtained from the Regional Ethics Committee. Four healthy pregnant volunteers (GA 30+0 to 31+0 weeks) were scanned on a Philips 3T Ingenia scanner in normal operating mode with participants placed in approximately a 15° left tilt to prevent vena cava compression. The sequence was a respiratory triggered gradient echo with 1D quantitative flow with EPI readout, of TE=29ms and minimum TR=9000ms (figure1A). The voxel size was 1.56x1.56x4 mm3 and between 6 and 10 slices were taken, of varying FOV to cover the entire placenta, with the duration of each scan varying from 5-10 minutes. Placentas were scanned in the transverse plane, with the 1D quantitative flow velocity encoding strength of ±1cm/s, and direction selected to measure transit across the placental width, with the first three participants encoded Anterior-Posterior, and the fourth Right-Left (figure1B).Two slices from the central region of each placenta were masked, and split into 4 ROIs (Figure2) by taking the outline of the placental mask and dividing it into maternal edge and fetal edge. Placental voxels within 6 voxels (9.4mm) of the maternal or fetal edge were classified as maternal or fetal side, the overlap of these masks was defined as the corners, and the remaining voxels were the centre of the placenta. The mean positive and negative velocities (corresponding to opposite directions) were calculated for each participant, from each acquisition.
The velocity data were smoothed slice by slice with a first order 2D Butterworth filter of size 6mm to reduce the effects of minor fetal or maternal motion. Volumes which contained gross motion causing artifacts were discarded from analysis.
Results
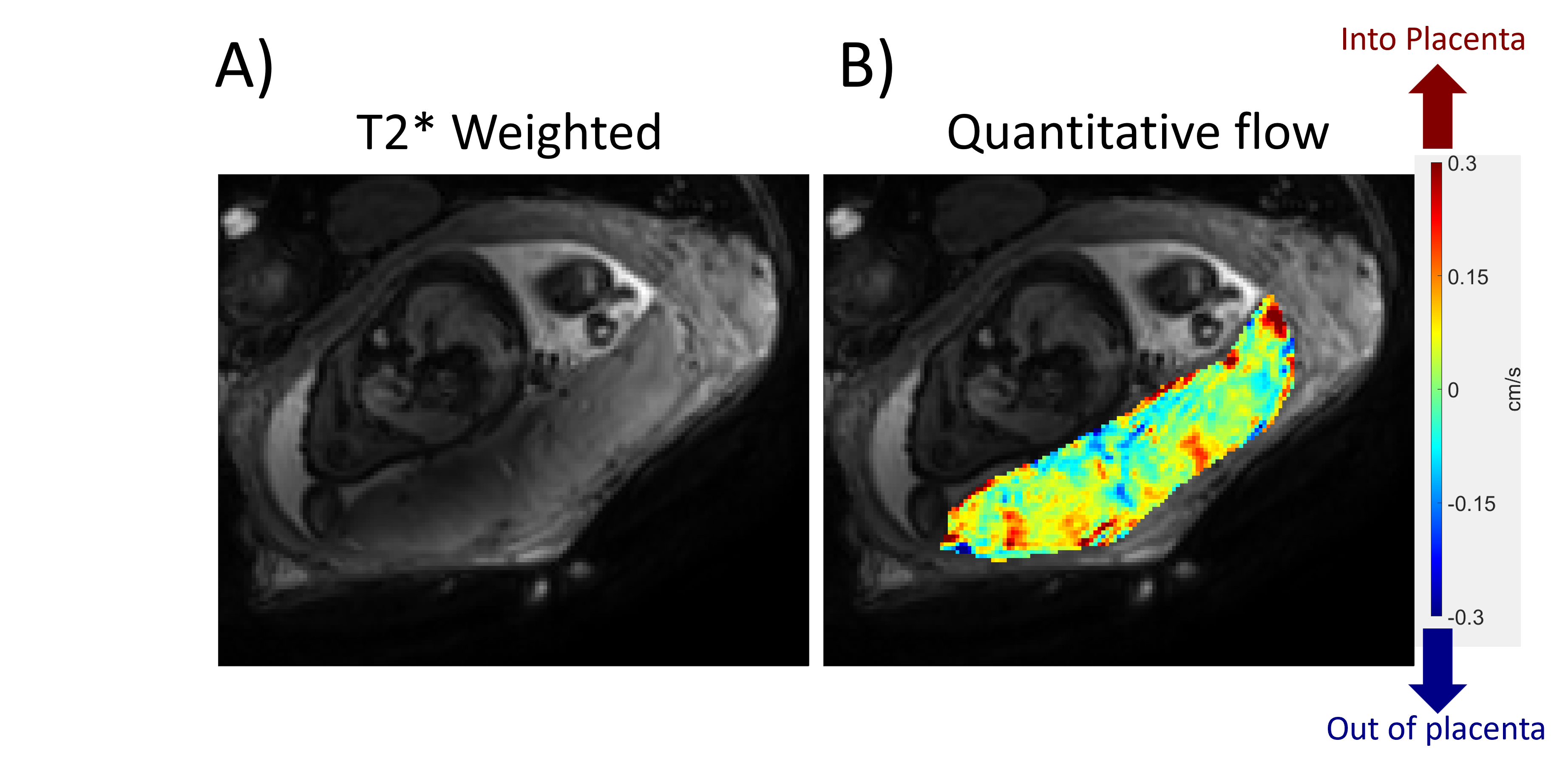
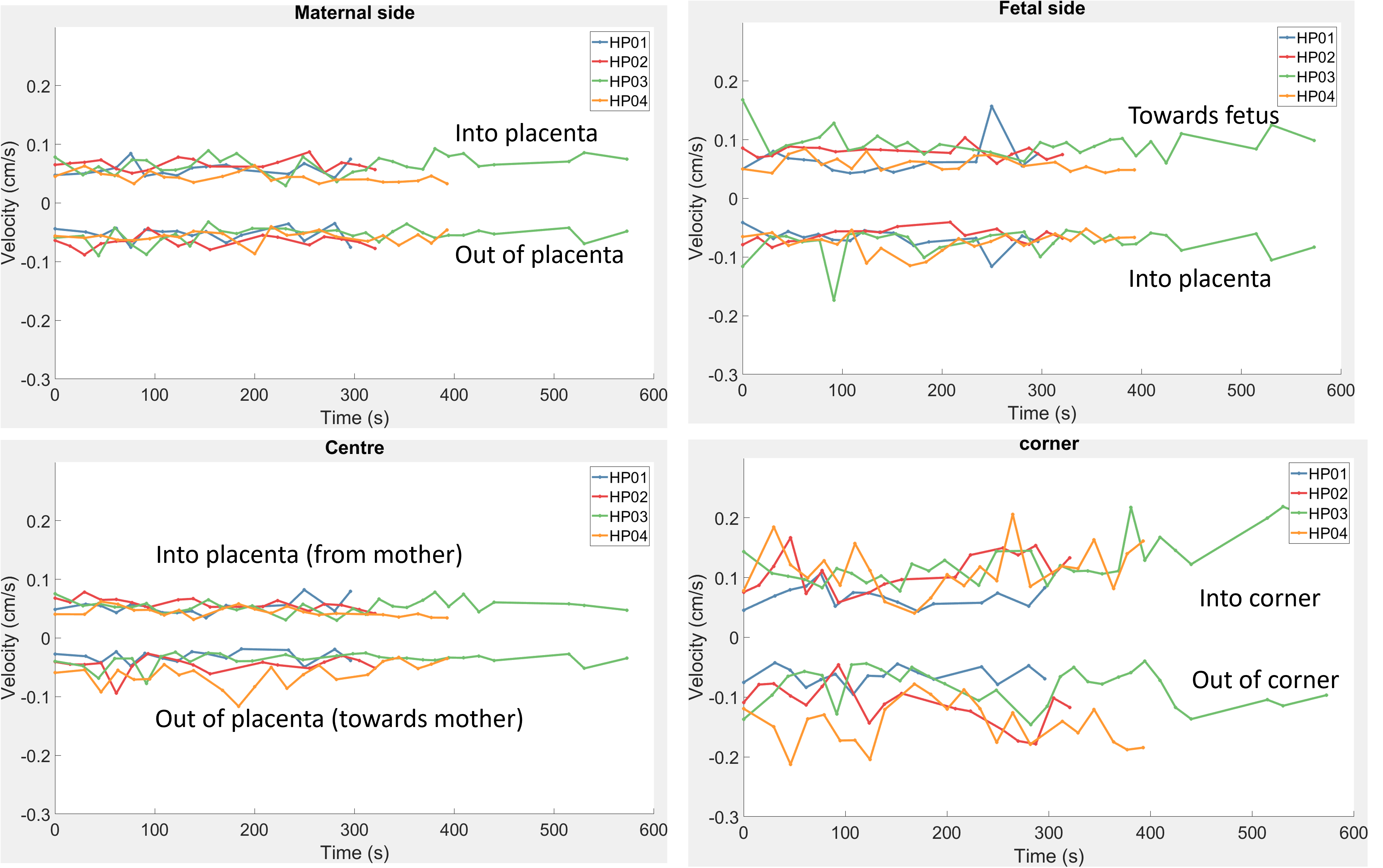
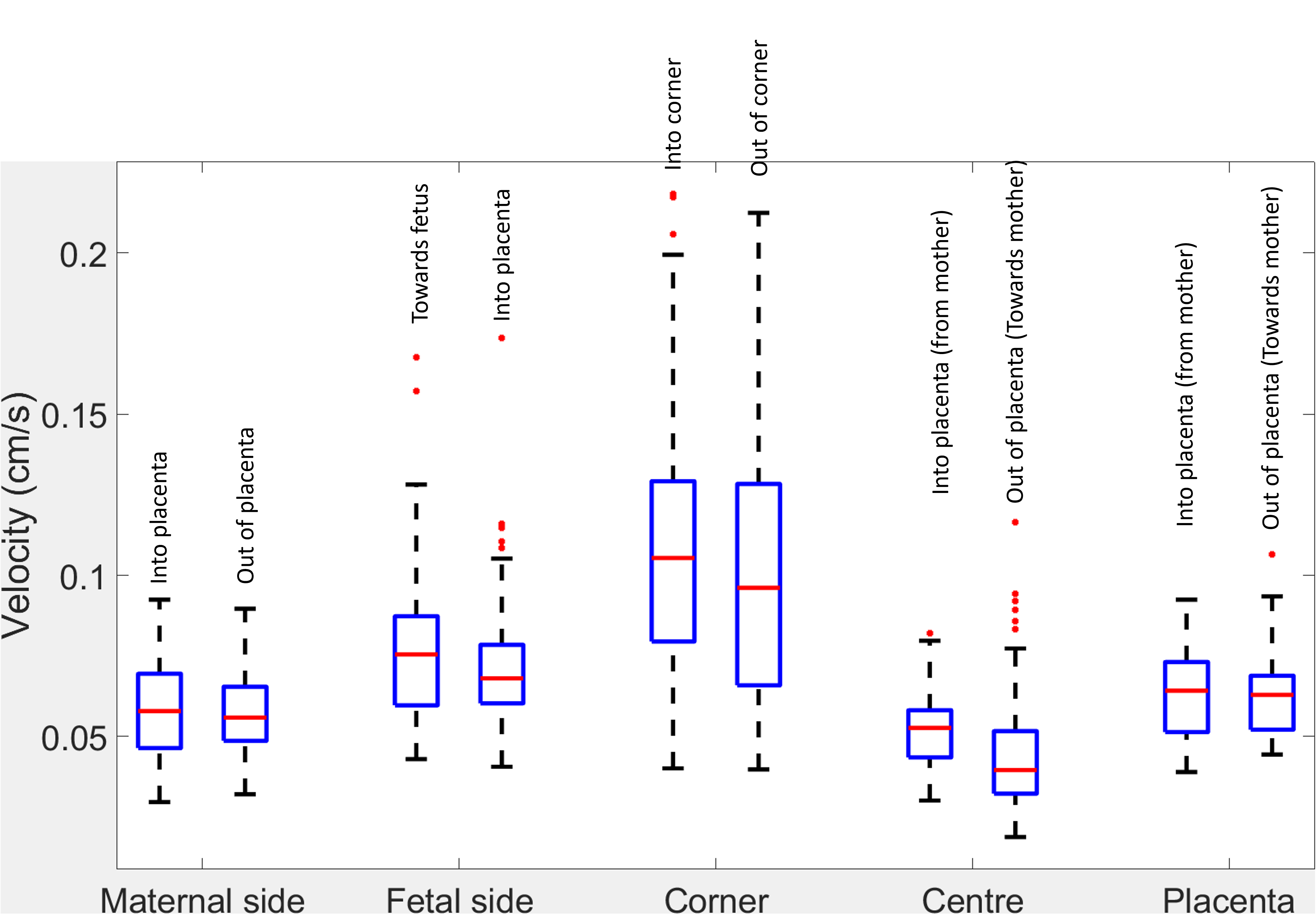
The T2* weighted magnitude from HP03 and the quantitative flow map from HP03 is shown in figure 3A&B, with the flow encoding from anterior to posterior (bottom to top of image).The mean value for each ROI from each dynamic acquisition, was plotted for each subject in figure 4, with the positive and negative directions labelled to clarify their direction. Data was then grouped for each ROI to produce boxplots over all acquisitions (figure5) including the average over the entire placenta.
Discussion
The quantitative flow showed slow flows throughout the placenta, with regions of faster flow into the placenta, probably due to spiral artery input, and some corner regions with very fast flow (Figure 3B).The average speeds were similar between subjects (figure4), and matched measurements made previously using Phase Contrast Angiography [2] (<0.1cm/s). These slow speeds are required to allow efficient exchange between the maternal and fetal blood pools, and have been shown to be significantly increased in compromised pregnancies [2].
The variation between subjects was generally small (figure5). Intersubject variation was larger in the corner ROI, maybe because it was the smallest ROI, but possibly also because it would depend on its position relative to a draining vein.
Qualitatively the T2* signal retained sufficient contrast to be used for other measurements (figure3A), and although this sequence was only tested on anterior placentas and, relatively early third trimester pregnancies, an echo time of 29ms should be suitable for later gestation also.
This sequence gave repeatable results within this small groups of subjects of similar gestational ages and shows promise for monitoring placental function over time. In future we will use this sequence to evaluate placental function in compromised pregnancies and over longer timeframes to investigate the effect of placental contractions on oxygenation and blood flow.
Acknowledgements
This work was funded by the Wellcome Leap In Utero program.References
[1] Sinding, M., Peters, D.A., Frøkjær, J.B., Christiansen, O.B., Petersen, A., Uldbjerg, N. and Sørensen, A. (2016), Placental magnetic resonance imaging T2* measurements in normal pregnancies and in those complicated by fetal growth restriction. Ultrasound Obstet Gynecol, 47: 748-754. https://doi.org/10.1002/uog.14917
[2] Dellschaft, N.S., Hutchinson, G., Shah, S., Jones, N.W., Bradley, C., Leach, L., Pratt., Bowtell, R., Gowland P., The haemodynamics of the uman placental in utero, P PLOS Biology 18(5): e3000676, 2020.
Figures