0177
Simplified Anisotropic IVIM using Spherical Means and an Application in the Placenta1Cardiff University Brain Research Imaging Centre, Cardiff University, Cardiff, United Kingdom, 2School of Computer Science and Informatics, Cardiff University, Cardiff, United Kingdom, 3BHF Manchester Centre for Heart and Lung Magnetic Resonance Research, University of Manchester, Manchester, United Kingdom, 4Division of Cardiovascular Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, United Kingdom, 5Maternal and Fetal Health Research Centre, Institute of Human Development, University of Manchester, Manchester, United Kingdom, 6St. Mary's Hospital, Manchester University Hospitals NHS Foundation Trust, University of Manchester, Manchester, United Kingdom, 7Centre for Medical Image Computing and Department of Computer Science, University College London, London, United Kingdom
Synopsis
Keywords: Placenta, Placenta
Motivation: The intravoxel incoherent motion (IVIM) model can separately assess diffusion in tissue and perfusion in vasculature. However, anisotropic extensions to IVIM that model coherently orientated vasculature are complex and difficult to fit.
Goal(s): Enhance the IVIM model to account for macroscopic anisotropy in vascular structures, while minimizing the increase in model complexity.
Approach: We model perfusion and diffusion compartments using constrained tensors and estimate the tensor parameters via the spherical mean.
Results: Our spherical mean anisotropic IVIM approach quantifies and maps anisotropy in perfusion and diffusion compartments and captures microstructural and microcirculatory alterations in the placenta during pregnancy.
Impact: Existing anisotropic IVIM models are complex and clinically impractical. We demonstrate a spherical mean approach that simplifies the disentanglement of perfusion- and diffusion-related anisotropy. This can enable rapid quantification of biomarkers for detecting microcirculatory and microstructural changes in anisotropic tissue.
Introduction
The intravoxel incoherent motion (IVIM) model separates diffusion- and perfusion-related components of the diffusion MRI (dMRI) signal. However, the IVIM model assumes isotropic signal attenuation, whereas macroscopic anisotropy can occur in diffusion-related components and perfusion-related components (e.g. in coherent vasculature in muscles1).Extensions to IVIM additionally accounting for macroscopic anisotropy in diffusion- and perfusion-related signal components have been demonstrated in muscle1, brain2–4, heart5, kidney6–8, prostate9, and placenta10. Separating perfusion- and diffusion-related anisotropy in dMRI offers the opportunity for new imaging biomarkers, for example separate perfusion- and diffusion-related fractional anisotropy (FA).
However, these anisotropic IVIM models are complex. For instance, some extend IVIM by incorporating full tensors for the diffusivity, perfusion-related diffusivity, and perfusion fraction, yielding an 18 parameter model7. Even when full tensors are only used for some of these, models involve numerous parameters.
Spherical mean techniques can calculate quantitative microstructural metrics whilst factoring out orientation dependence11, meaning fewer model parameters that are easier to fit whilst still accounting for anisotropy. Here we introduce simplified anisotropic IVIM using spherical mean (SM) techniques and demonstrate its application in placental MRI.
Methods
Pregnant participants gave informed consent to undergo dMRI of the placenta (22-37 weeks’ gestation), DAPHNE study (REC 22/YH/0144). Here, we include data from 19 participants with normal pregnancy outcome (defined as normotensive pregnancy, and term delivery of normal birthweight baby).We scanned on a Siemens Vida scanner at 3T using the Body 18 coil, utilising a previously published dMRI protocol that was optimised for the placenta12. The protocol has $$$b= [5,10,18,25,36,50,100,200,400,600,800,1200,1600]\;$$$s mm-2 with multiple gradient directions optimised for maximal angular coverage13. Other imaging parameters were TE$$$=83\;$$$ms, TR$$$=3300\;$$$ms, Grappa 2, partial Fourier 6/8, voxel size = $$$3\times3\times15\;$$$mm, image matrix $$$128\times128\times9$$$, acquisition time = 3:07.
Data were pre-processed with MP-PCA denoising14, Rician bias correction15, and Gibbs ringing removal16. We manually defined a region-of-interest (ROI) containing the placenta and basal plate as previously described10.
We fit the diffusion tensor (DT) with weighted linear least squares17 utilising all measurements, and calculated downstream metrics, using MRTrix18. We fit IVIM in dmipy19.
We introduce two anisotropic IVIM spherical mean approaches, based on stick-zeppelin and zeppelin-zeppelin models that were previously suggested for placental dMRI10. These are two-compartment models made up of stick20 and zeppelin21 components.
The spherically averaged stick signal is
$$\bar{S}_S(d_{par})=\frac{\sqrt{\pi}\;\mbox{erf}\left({\sqrt{bd_{par}}}\right)}{2\sqrt{bd_{par}}}$$
where erf() is the error function, $$$d_{par}$$$ is the parallel diffusivity, $$$\bar{S}_S$$$ is the spherically averaged signal and $$$b$$$ is the b-value.
The spherically averaged zeppelin signal is11
$$\bar{S}_Z(d_{par},d_{perp})=\exp(-bd_{perp})\frac{\sqrt{\pi}\;\mbox{erf}\left({\sqrt{b(d_{par}-d_{perp})}}\right)}{2\sqrt{b(d_{par}-d_{perp})}}$$
where dperp is the perpendicular diffusivity.
The signal for SM-zeppelin-zeppelin is
$$\bar{S}=f\bar{S}_Z(d_{par}^*,d_{perp}^*)+(1-f)\bar{S}_Z(d_{par},d_{perp}).$$
The signal for SM-stick-zeppelin is
$$\bar{S}=f\bar{S}_S(d_{par}^*)+(1-f)\bar{S}_Z(d_{par},d_{perp}).$$
We fit SM-stick-zeppelin and SM-zeppelin-zeppelin using dmipy19. We calculated FA for the tissue- and perfusion-related zeppelin compartments separately.
Figure 1 gives the parameter constraints when fitting, and Figure 2 schematically represents each model.
Results
Figure 3 displays all maps for one participant. DT and IVIM maps are akin to previous studies10. For example, diffusivities, FA, and perfusion fraction are higher at placental margins. SM-stick-zeppelin perfusion-related diffusivity is high in the basal plate whereas diffusion-related diffusivity is high in the chorionic plate. Both SM-stick-zeppelin and SM-zeppelin-zeppelin tissue-related FA maps show intra-placental contrast.Figure 4 plots the ROI-averaged parameter values against gestational age for each participant, showing that these parameters capture diffusion- and perfusion-related changes over gestation. SM-stick-zeppelin has the two parameters with highest correlation with gestation.
Discussion
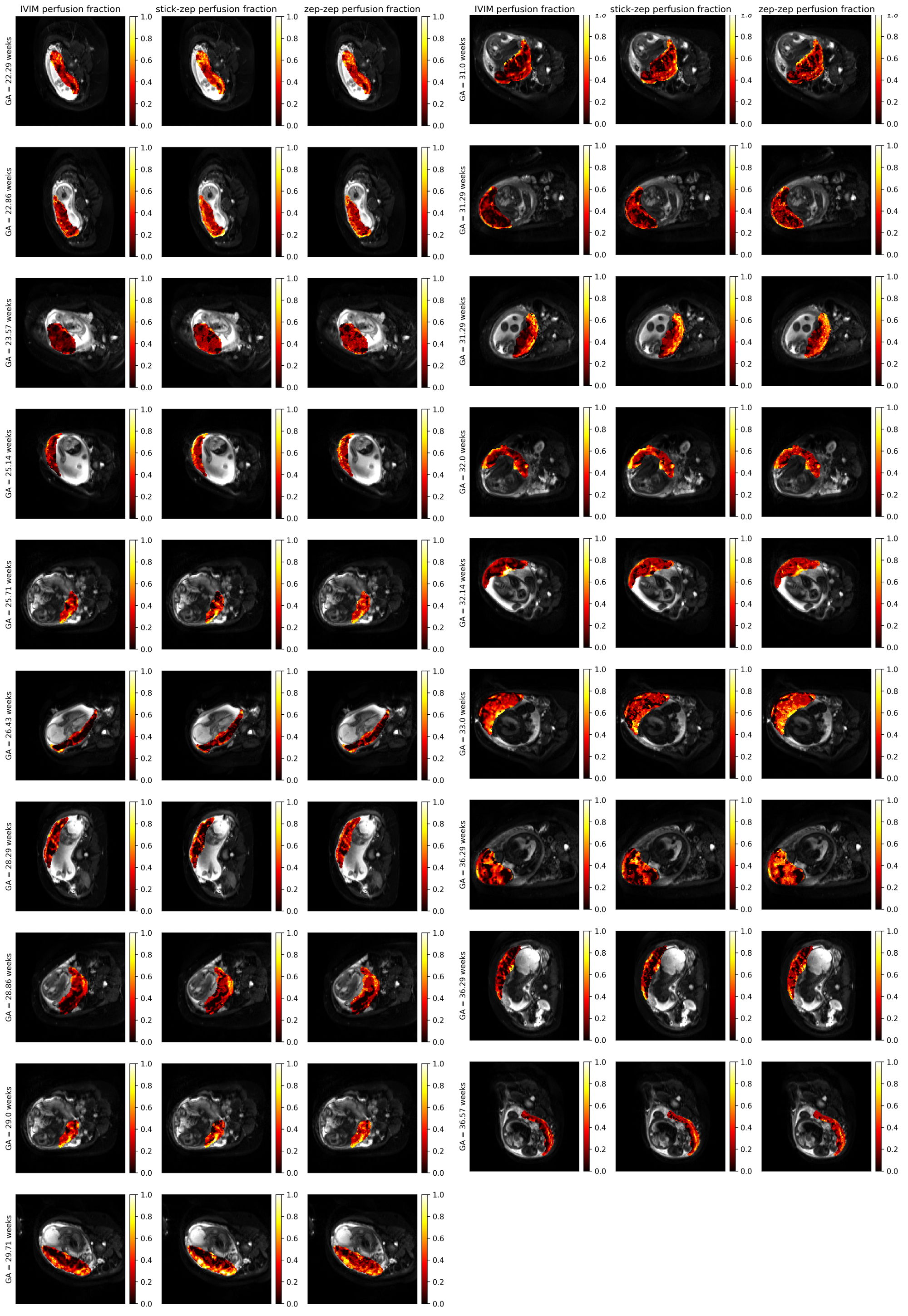
Our novel approach maps diffusivity and anisotropy related to microcirculation and microstructure. Maps reveal consistent patterns across 19 scanned participants, illustrated in Figure 5 for perfusion fraction, and capture changes across gestation (Figure 4). The SM-stick-zeppelin perfusion fraction and perfusion-related parallel diffusivity have the highest correlation with gestational age, suggesting that an anisotropic IVIM SM approach better captures microstructural and microcirculatory changes than DT and IVIM models, and has potential for accurately capturing such alterations in dysfunctional placentas.DT-derived diffusivities decrease over gestation (Figure 4), in agreement with previous literature22. However, whilst the SM-stick-zeppelin perfusion-related $$$d_{par}$$$ decreases over gestation, both SM-stick-zeppelin tissue-related diffusivities increase over gestation (Figure 4). This suggests that SM-stick-zeppelin can disentangle different sources of attenuation in placental dMRI data, and that perfusion- and diffusion-related components may evolve differently over gestational age.
We used a straightforward signal direction-averaging method although our protocol, with multiple b-shells, is not ideally suited for this. Future work will explore using rotational invariants to more accurately estimate the spherical mean23.
Conclusion
We introduce an anisotropic IVIM SM approach to disentangle perfusion- and tissue-related diffusivity and anisotropy. This approach captures changes across gestation in placental MRI better than baseline models. Perfusion- and tissue-specific metrics are potential biomarkers for various diseases.Acknowledgements
We thank all pregnant participants, midwives, obstetricians, and radiographers who played a key role in obtaining the datasets. This work was funded by the Wellcome Leap In Utero programme project “Multi-modal studies to understand pregnancy and prevent stillbirth”.References
1. Karampinos, D. C., King, K. F., Sutton, B. P. & Georgiadis, J. G. Intravoxel partially coherent motion technique: Characterization of the anisotropy of skeletal muscle microvasculature. J. Magn. Reson. Imaging 31, 942–953 (2010).
2. Finkenstaedt, T. et al. The IVIM signal in the healthy cerebral gray matter: A play of spherical and non-spherical components. NeuroImage 152, 340–347 (2017). 3. Mozumder, M., Beltrachini, L., Collier, Q., Pozo, J. M. & Frangi, A. F. Simultaneous magnetic resonance diffusion and pseudo-diffusion tensor imaging. Magn. Reson. Med. 00, 1–12 (2017).
4. Voorter, P. H. M. et al. On the anisotropy of IVIM-derived microvascular cerebral pseudo-diffusion: a physics-informed neural network approach. in 0872 doi:10.58530/2022/0872.
5. Abdullah, O. M. et al. Orientation dependence of microcirculation-induced diffusion signal in anisotropic tissues. Magn. Reson. Med. n/a-n/a (2015) doi:10.1002/mrm.25980.
6. Notohamiprodjo, M. et al. Combined intravoxel incoherent motion and diffusion tensor imaging of renal diffusion and flow anisotropy. Magn. Reson. Med. 73, 1526–1532 (2015).
7. Hilbert, F. et al. An intravoxel oriented flow model for diffusion-weighted imaging of the kidney. NMR Biomed. 29, 1403–1413 (2016).
8. Liu, A. L. et al. REnal Flow and Microstructure AnisotroPy (REFMAP) MRI in Normal and Peritumoral Renal Tissue. J. Magn. Reson. Imaging 1–10 (2018) doi:10.1002/jmri.25940.
9. Panagiotaki, E. et al. Noninvasive quantification of solid tumor microstructure using VERDICT MRI. Cancer Res. 74, 1902–1912 (2014).
10. Slator, P. J. et al. Placenta microstructure and microcirculation imaging with diffusion MRI. Magn. Reson. Med. 80, 756–766 (2018).
11. Kaden, E., Kelm, N. D., Carson, R. P., Does, M. D. & Alexander, D. C. Multi-compartment microscopic diffusion imaging. NeuroImage 139, 346–359 (2016).
12. Slator, P. J. et al. A framework for calculating time-efficient diffusion MRI protocols for anisotropic IVIM and an application in the placenta. in CDMRI’18 (2018).
13. Caruyer, E., Lenglet, C., Sapiro, G. & Deriche, R. Design of multishell sampling schemes with uniform coverage in diffusion MRI. Magn. Reson. Med. Off. J. Soc. Magn. Reson. Med. Soc. Magn. Reson. Med. 69, 1534–40 (2013).
14. Veraart, J. et al. Denoising of diffusion MRI using random matrix theory. NeuroImage 142, 394–406 (2016).
15. Koay, C. G. & Basser, P. J. Analytically exact correction scheme for signal extraction from noisy magnitude MR signals. J. Magn. Reson. 179, 317–322 (2006).
16. Kellner, E., Dhital, B., Kiselev, V. G. & Reisert, M. Gibbs‐ringing artifact removal based on local subvoxel‐shifts. Magn. Reson. Med. 76, 1574–1581 (2016).
17. Veraart, J., Sijbers, J., Sunaert, S., Leemans, A. & Jeurissen, B. Weighted linear least squares estimation of diffusion MRI parameters: Strengths, limitations, and pitfalls. NeuroImage 81, 335–346 (2013).
18. Tournier, J.-D. et al. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. NeuroImage 202, 116137–116137 (2019).
19. Fick, R. H. J., Wassermann, D. & Deriche, R. The Dmipy Toolbox: Diffusion MRI Multi-Compartment Modeling and Microstructure Recovery Made Easy. Front. Neuroinformatics 13, 1–26 (2019).
20. Behrens, T. E. J. et al. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magn. Reson. Med. 50, 1077–1088 (2003).
21. Panagiotaki, E. et al. Compartment models of the diffusion MR signal in brain white matter: A taxonomy and comparison. NeuroImage 59, 2241–2254 (2012).
22. Hutter, J. et al. Multi‐modal functional MRI to explore placental function over gestation. Magn. Reson. Med. 81, 1191–1204 (2019).
23. Coelho, S., Fieremans, E. & Novikov, D. S. Zero-shell diffusion MRI: Focus on microstructure by decoupling fiber orientations. in ISMRM 2023.
Figures