0175
Using Virtual Magnetic Resonance Elastography and IVIM to Evaluate Placental Microstructure and Microcirculation in Gestational Hypertension1Department of Radiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 2MR Research Collaboration, Siemens Healthineers, Shanghai, China, 3Department of Obstetrics & Gynecology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 4MR Research Collaboration, Siemens Healthineers, Beijing, China
Synopsis
Keywords: Placenta, fMRI, Gestational hypertension, perfusion, placenta, virtual magnetic resonance elastography
Motivation: Detecting placental dysfunction using MRI before placental macrovascular lesions by ultrasound may help the early identification of placental pathologic changes in gestational hypertension (GH).
Goal(s): To explore changes in placental elasticity and perfusion in GH and control groups using MRI.
Approach: Placental elasticity and perfusion were assessed using virtual magnetic resonance elastography (vMRE) and intravoxel incoherent motion (IVIM). The vMRE and IVIM parameters, MR morphologic parameters, and ultrasound and lab test results were compared between the two groups.
Results: Placental stiffness and perfusion fraction helped distinguish between the two groups, with no substantial differences in the other parameters.
Impact: Virtual magnetic resonance elastography and intravoxel incoherent motion can quantify placental elasticity and circulation at the microscopic level, and are superior to the ultrasound parameters, in gestational hypertension. They may serve as a vital noninvasive supplement to assess placental dysfunction.
Introduction
Gestational hypertension (GH) significantly endangers maternal and fetal health, primarily due to aberrant placental formation and compromised perfusion1,2. Traditional Doppler imaging is inadequate as it evaluates only larger vessels, such as the umbilical artery (UA) or fetal middle cerebral artery (MCA), missing finer microcirculatory and structural changes3. Virtual magnetic resonance elastography (vMRE) and intravoxel incoherent motion (IVIM) emerge as noninvasive tools, crucial for assessing placental biomechanics and perfusion, which may detect early dysfunction4,5. vMRE's proficiency in measuring tissue elasticity and IVIM's in characterizing microcirculation within the placenta have been noted, yet their roles in differentiating GH from normal pregnancies remain unexplored. This research seeks to fill this void, contrasting placental elasticity and microcirculatory metrics in GH-affected and healthy pregnancies via vMRE and IVIM, aiming to shed new light on GH's placental attributes6-10.Methods
This retrospective study was approved by the institutional review board. We included 44 pregnant women based on the inclusion and exclusion criteria. MRI was performed in all patients using a 1.5T system (MAGNETOM Aera, Siemens Healthineers AG, Erlangen, Germany) with a 12-channel surface body coil and 2 embedded spine coils. The images were acquired using the T2-weighted Half-Fourier-Acquired Single-shot Turbo Spin Echo (HASTE) sequence with the following parameters: TR/ TE, 1300 ms/167 ms; slice thickness, 4.0 mm; field of view (FOV), 380 × 309 mm2. The IVIM images were collected using a spectrum of distinct b values of 0, 50, 100, 150, 200, 500, and 800 s/mm2. The scanning parameters were as follows: TR/TE, 6400 ms/65 ms; slice thickness, 5.5 mm; FOV, 320 × 320 mm2. Two radiologists with 5 and 10 years of experience, respectively, manually delineated the region of interest on placental IVIM images. The stiffness value presented by μdiff was automatically calculated using the vMRE toolbox based on the following equation: μdiff=α∙ln(S200⁄S800)+β (α= -9.8, β=14) (6). The IVIM parameters including true diffusion coefficient (D), pseudo-diffusion coefficient (D*), perfusion fraction (f), and apparent diffusion coefficient (ADC) values were processed with FireVoxel software (CAI2R; New York University, NY, USA) (Fig. 1). T2-weighted imaging was used to obtain placental areas and volumes. The pulsatility index (PI), resistance index (RI), and peak systolic velocity/end-diastolic velocity (S/D) in UA and MCA and all laboratory test indexes were recorded retrospectively. The cerebroplacental ratio (CPR) value was calculated as MCA - PI/UA - PI.Results
A total of 14 patients were recruited in the GH group and 30 individuals in the control group. The demographic and clinical data are described in Table 1. The prothrombin time (PT), D, f, and ADC values were substantially lower in the GH group compared with the control group (P <.05). The µdiff value was statistically higher in the GH group compared with the control group (P <.05) (Fig. 2). The other laboratory indexes, D*, all MRI morphological parameters, and Doppler parameters were similar between the 2 groups (P >.05) (Table 2). The area under curve (AUC) of the combination model differentiating patients with GH from controls was 0.862, with a sensitivity of 71.4% and specificity of 93.3%.Discussion
Ultrasound usually reflects placental insufficiency by measuring hemodynamic changes in the UA11. However, its imaging and flowmetry cannot assess the microperfusion and microstructural placental qualities. Most current studies agree that, when placental hypoxia and oxidative stress occur, they lead to the entry of proinflammatory and antiangiogenic mediators into the maternal–fetal circulation12. This triggers an increased inflammatory response and endothelial dysfunction, considerably reducing placental chorioallantoic capillaries and a remarkable increase in intervillous fibrosis, fibrous material deposition, and atherosclerotic infarction13. As the disease progresses, inadequate placental microcirculation leads to vascular resistance increased. Although the detailed mechanisms need further investigation, we believe that, at the time of the ultrasound diagnosis, the placental function is already substantially suppressed and the placental microstructure is damaged. Hence, magnetic resonance has the advantage of detecting the changes in placental microcirculatory perfusion and elasticity, demonstrating the mild forms of placental insufficiency that have already occurred in the GH that Doppler ultrasound may not accurately identify. We did not observe a considerable difference in MRI morphological parameters between the 2 groups. This might be explained by “shape adaptation,” suggesting that the placenta might try to expand its area and volume to adapt flexibly to the difficult and unpredictable situations14.Conclusion
For pregnant women with GH, vMRE and IVIM functional parameters can detect alterations in placental microstructure and microcirculation earlier than conventional ultrasound and laboratory methods.Acknowledgements
This study was financially supported by the Young Scholars Fostering Fund of the First Affiliated Hospital of Nanjing Medical University (PY2021002).
References
2. Wu P, Green M, Myers JE. Hypertensive disorders of pregnancy. BMJ 2023; 381:e71653.
3. Papageorghiou AT, Yu CK, Cicero S, Bower S, Nicolaides KH. Second-trimester uterine artery Doppler screening in unselected populations: a review. J Matern Fetal Neonatal Med 2002; 12:78-88.
4. Le Bihan D. What can we see with IVIM MRI? Neuroimage 2019; 187:56-67.
5. Le Bihan D, Ichikawa S, Motosugi U. Diffusion and Intravoxel Incoherent Motion MR Imaging-based Virtual Elastography: A Hypothesis-generating Study in the Liver. Radiology 2017; 285:609-619.
6. Deng J, Cao Y, Lu Y, et al. Value of placental virtual magnetic resonance elastography and intravoxel incoherent motion-based diffusion and perfusion in predicting adverse outcomes of small-for-gestational-age infants. Insights Imaging 2023; 14:153.
7. Kromrey ML, Le Bihan D, Ichikawa S, Motosugi U. Diffusion-weighted MRI-based Virtual Elastography for the Assessment of Liver Fibrosis. Radiology 2020; 295:127-135.
8. Chen T, Zhao M, Song J, et al. The effect of maternal hyperoxygenation on placental perfusion in normal and Fetal Growth Restricted pregnancies using Intravoxel Incoherent Motion. Placenta 2019; 88:28-35.
9. Deng J, Zhang A, Zhao M, et al. Placental perfusion using intravoxel incoherent motion MRI combined with Doppler findings in differentiating between very low birth weight infants and small for gestational age infants. Placenta 2023; 135:16-24.
10. Siauve N, Hayot PH, Deloison B, et al. Assessment of human placental perfusion by intravoxel incoherent motion MR imaging. J Matern Fetal Neonatal Med 2019; 32:293-300.
11. Hernandez-Andrade E, Huntley ES, Bartal MF, et al. Doppler evaluation of normal and abnormal placenta. Ultrasound Obstet Gynecol 2022; 60:28-41.
12. Chang KJ, Seow KM, Chen KH. Preeclampsia: Recent Advances in Predicting, Preventing, and Managing the Maternal and Fetal Life-Threatening Condition. Int J Environ Res Public Health 2023; 20.
13. Jahan F, Vasam G, Green AE, Bainbridge SA, Menzies KJ. Placental Mitochondrial Function and Dysfunction in Preeclampsia. Int J Mol Sci 2023; 24.
14. Haeussner E, Schmitz C, von Koch F, Frank HG. Birth weight correlates with size but not shape of the normal human placenta. Placenta 2013; 34:574-582.
Figures
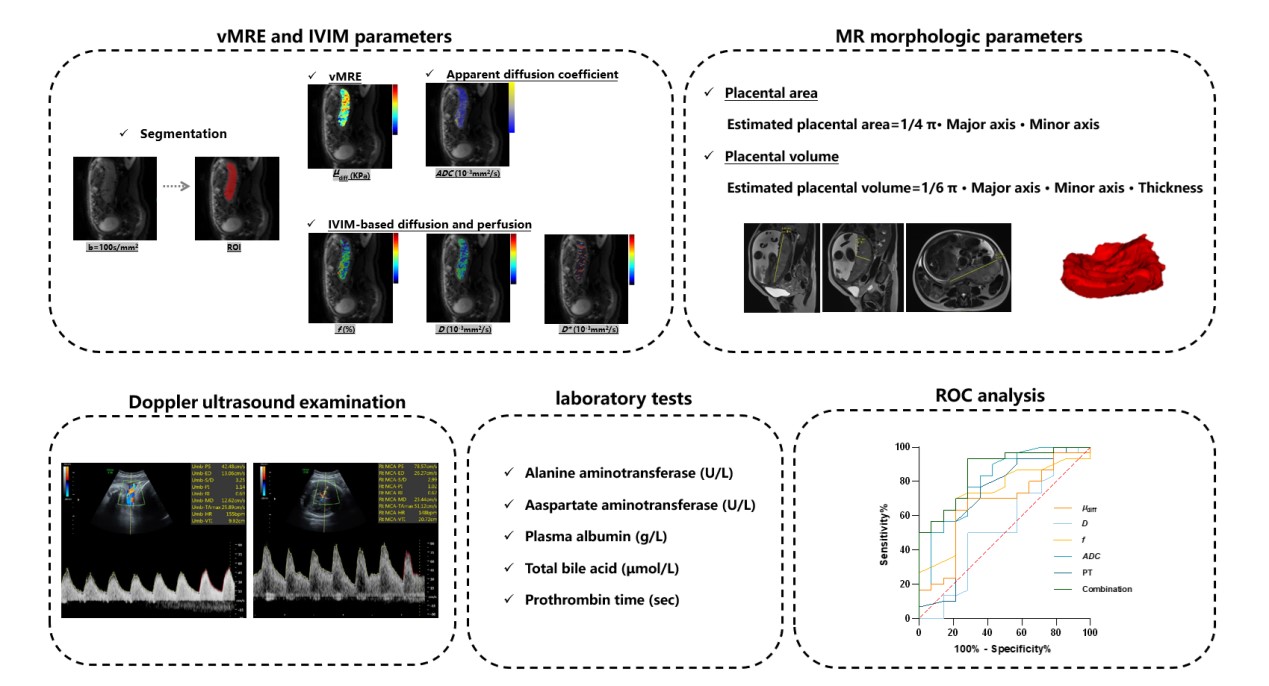
Figure 1. Framework of the study.
CPR, cerebroplacental ratio; μdiff, diffusion-weighted imaging–based shear modulus; D, true diffusion coefficient; D*, pseudo-diffusion coefficient; f, perfusion fraction; IVIM, intravoxel incoherent motion; MCA, middle cerebral artery; PI, pulsatility index; RI, resistance index; ROC, receiver-operating characteristic; ROI, region of interest; S/D, peak systolic velocity/end-diastolic velocity; UA, umbilical arterial; vMRE, virtual magnetic resonance elastography.
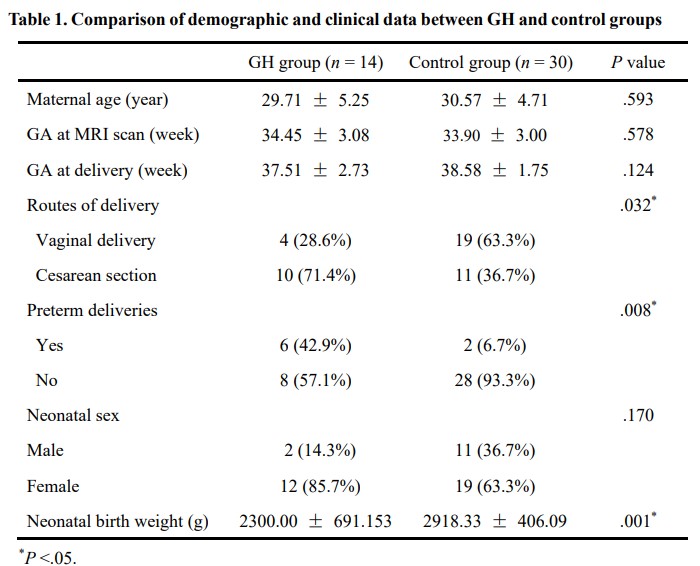
Table 1. Comparison of demographic and clinical data between GH and control groups
GA, Gestational age; GH, gestational hypertension; MRI, magnetic resonance imaging; PE, preeclampsia.
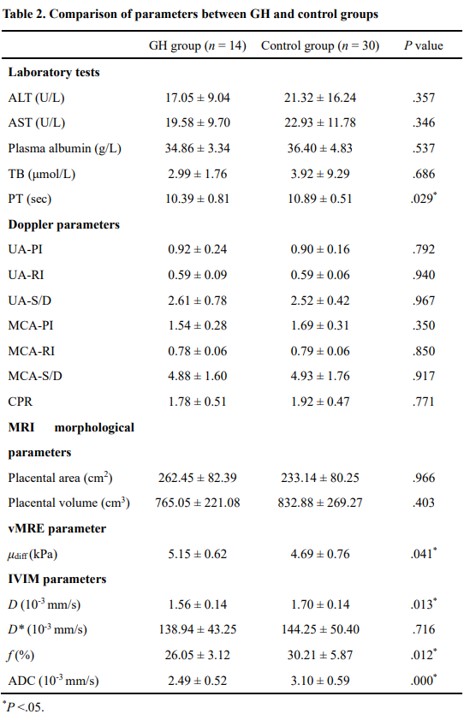
Table 2. Comparison parameters between GH and control groups
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CPR, cerebroplacental ratio; μdiff, diffusion-weighted imaging–based shear modulus; D, true diffusion coefficient; D*, pseudo-diffusion coefficient; f, perfusion fraction; MCA, middle cerebral artery; PI, pulsatility index; PT, prothrombin time; RI, resistance index; S/D, peak systolic velocity/end-diastolic velocity; TB, total bile acid; UA, umbilical arterial; vMRE, virtual magnetic resonance elastography.
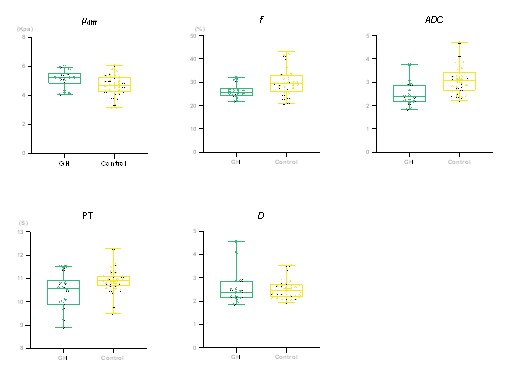
Figure 2. Box plots of µdiff, D, f, ADC, and PT for GH and control groups.
ADC, apparent diffusion coefficient; μdiff, diffusion-weighted imaging–based shear modulus; D, true diffusion coefficient; f, perfusion fraction; GH, gestational hypertension; PT, prothrombin time.
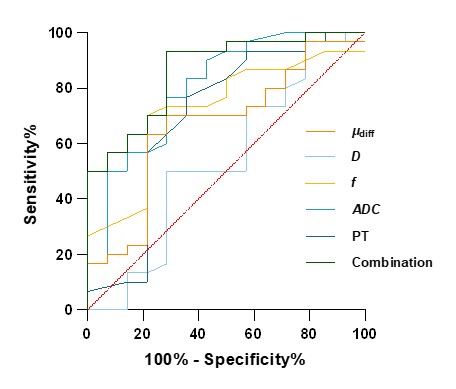
Figure 3. ROC curves for differentiating GH groups from control groups.
ADC, apparent diffusion coefficient; μdiff, diffusion-weighted imaging–based shear modulus; D, true diffusion coefficient; f, perfusion fraction; PT, prothrombin time; ROC, receiver-operating characteristic.