0174
Longitudinal Trends and Effects in Placenta Multiparametric MRI (mpMRI) in Early Gestation1Physics and Biology in Medicine, University of California Los Angeles, Los Angeles, CA, United States, 2University of California Los Angeles, Los Angeles, CA, United States, 3Pediatrics, University of California Los Angeles, Los Angeles, CA, United States, 4Radiology, University of California Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Placenta, Placenta
Motivation: This study is motivated by the clinical need to understand and monitor early gestational placenta development.
Goal(s): The goal is to show that multi-parametric placenta imaging during early gestation is a clinical tool to flag possible pregnancies in danger of multiple adverse effects.
Approach: This study includes data from a previous perspective study where MRI was taken at two separate timepoints during early gestation. Information on volume, perfusion, and oxygenation were evaluated for longitudinal trends as well as changes driven by obesity and fetal sex outcomes.
Results: We show statistically significant differences of longitudinal trends in most of the parameters between study cohorts.
Impact: The results in this study could allow for clinicians to gain insight on pregnancy development within the early second trimester currently unavailable with the current imaging with Doppler ultrasound. This will allow for overall life improvement for mother and fetus.
INTRODUCTION
To describe longitudinal differences of placental volume, oxygenation, and perfusion during early gestation of adverse pregnancy groups vs. an uncomplicated pregnancy group as well as changes in longitudinal trends based on maternal and fetal conditions.METHODS
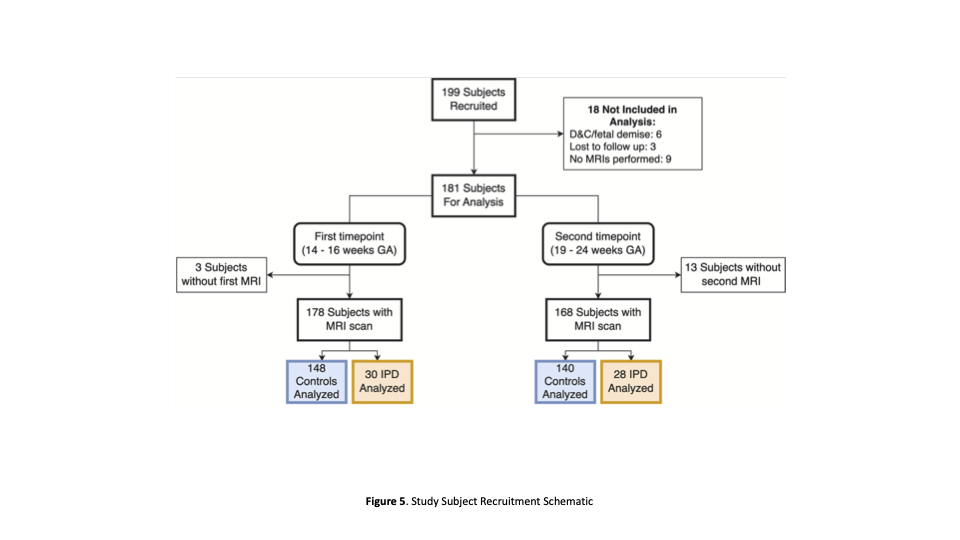
The study included a prospective cohort of 199 women who underwent 3T MRI at two-time points between 14-16 and 18-24 gestational weeks . This study continually monitored the pregnancy via other study time points, allowing information such as fetal sex and placenta weight to be considered during data analysis. Both MRI timepoints collected information on placental volume, oxygenation (T2*), and perfusion (PBF; placenta blood flow, and hPBF; high placenta blood flow) thus allowing for probing in trends between adverse effect groups. Previous studies found predictive measures of IPD and specifically fetal growth restriction and small gestational age cohort (FGR+SGA) and fetal growth restriction and small gestational age and preeclampsia cohort (FGR+SGA+PE). However, our study uses linear regression to determine the longitudinal development of the placenta in early gestation using the same MRI-derived parameters. The cohorts investigated are uncomplicated pregnancies defined as no IPD diagnosis as well as FGR, SGA and preeclampsia diagnosis, FGR+SGA cohort, and FGR+SGA+PE cohort. The sub-cohorts explored are Obese and Non-Obese cohorts and Female and Male fetal sex cohorts for each parameter for only the uncomplicated pregnancy group. Only the sub-cohorts of uncomplicated pregnancies are investigated due to the lack of obese patients with adverse effects and the lack of both sexes present in the FGR+SGA cohort and FGR+SGA+PE cohort. Obesity in this study is defined as a pre-pregnancy BMI equal to or over 30 as consulted by the collaboration's OBGYN. Z scores were calculated to understand variable behavior in comparison to the uncomplicated group, as well as p-values to determine significance.RESULTS
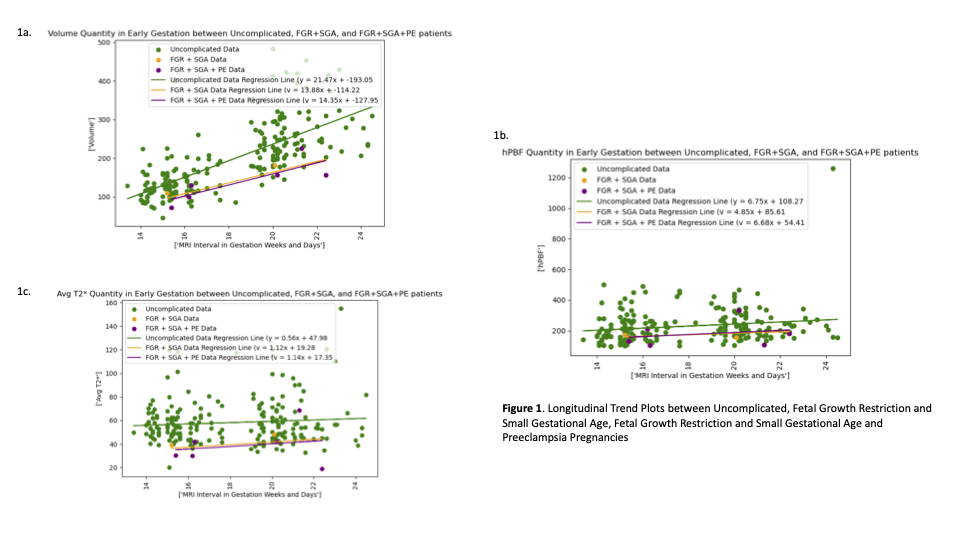
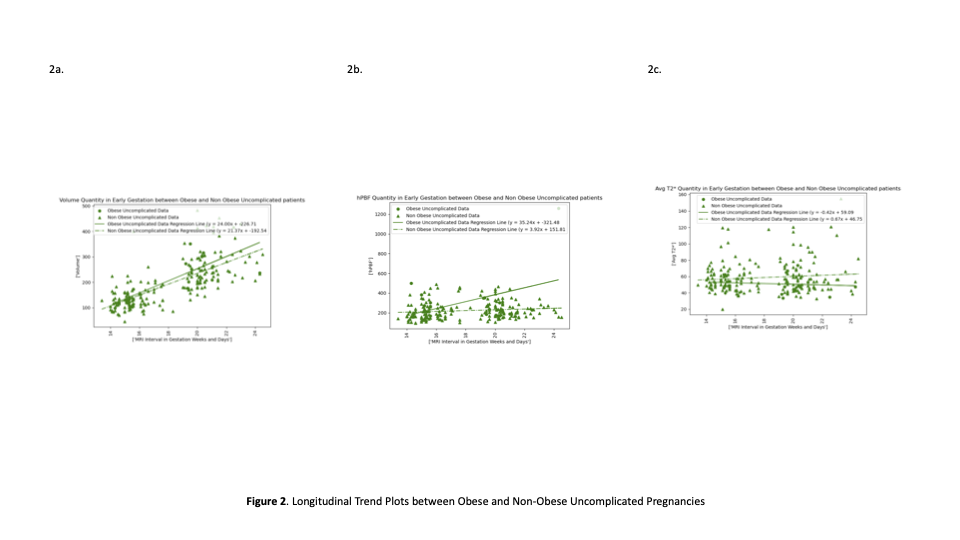
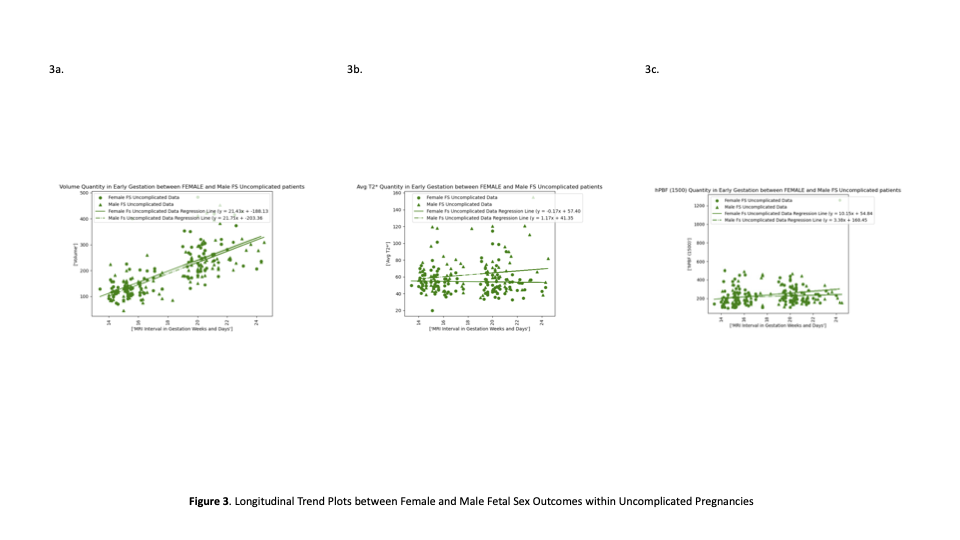
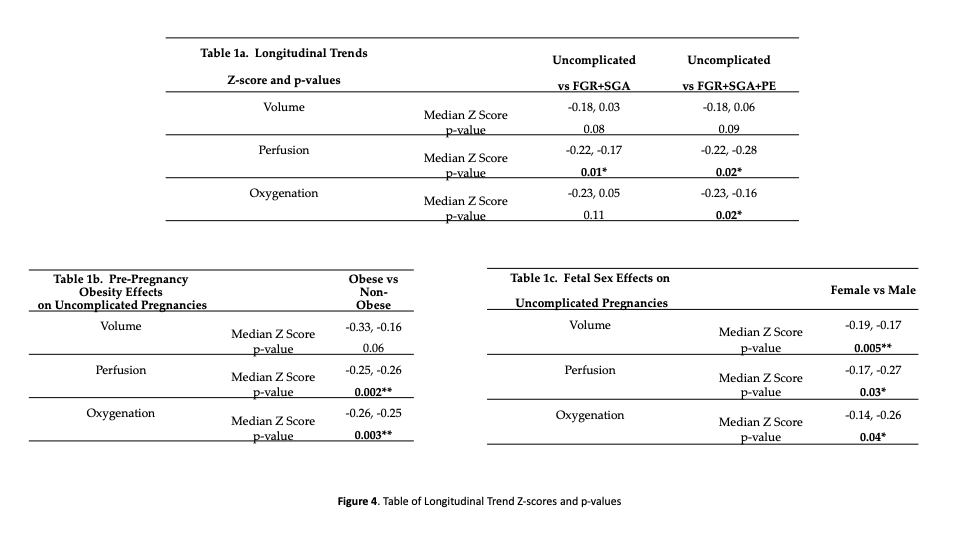
Figure 1 shows longitudinal trends of volume, perfusion, and oxygenation of uncomplicated pregnancies, FGR+SGA pregnancies, and FGR+SGA+PE pregnancies. Figure 2 and 3 show, respectively, the effects of obesity and fetal sex on the MRI parameters of uncomplicated pregnancies. The median Z scores and p-values are reported, with p-values being calculated in comparison to the uncomplicated pregnancy z score. Table 1a shows longitudinal trend differences between Uncomplicated and FGR+SGA cohorts and Uncomplicated and FGR+SGA+PE cohorts. Volume showed -0.18 and 0.03 z scores in the Uncomplicated and FGR+SGA cohorts, respectively, and -0.18 and 0.06 z scores in the Uncomplicated and FGR+SGA+PE cohorts, with p-values reported as 0.08 and 0.09. Perfusion showed -0.22 and -0.17 z scores in the Uncomplicated and FGR+SGA cohorts and -0.22 and-0.28 z scores in the Uncomplicated and FGR+SGA+PE cohorts with p-values reported as 0.01* and 0.02*. Oxygenation showed -0.23 and 0.05 z scores in the Uncomplicated and FGR+SGA cohorts and -0.23 and -0.16 z scores in the Uncomplicated and FGR+SGA+PE cohorts with p-values reported as 0.11 and 0.02*. The sub-cohort findings can be found in Tables 1b. and 1c. showing significance in z scores for each parameter except volume in obese vs. non obese cohort.DISCUSSION
MRI-derived volume shows non-significant differing trends in placenta development as well as offset in placenta growth measurements for uncomplicated pregnancies and FGR+SGA/FGR+SGA+PE cohorts. MRI-derived perfusion and oxygenation show statistically significant differences in the longitudinal trend in the FGR+SGA+PE cohort. This is driven by the offset of the measurements, as shown in Figure 1. There was statistical significance within perfusion longitudinal trend differences between uncomplicated pregnancies and FGR+SGA cohorts excluding oxygenation trends within the same cohorts.Uncomplicated pregnancies from obese women show significant differences in perfusion and oxygenation. Perfusion measurements had a steeper slope trend, showing expected higher perfusion starting at the beginning of the second trimester. The inverse is present in the oxygenation trends showing continuously lower oxygenation measurements during early gestation for obese patients, also expected as early as the start of the second trimester. The fetal sex outcome shows statistical significance in all the MRI parameters for uncomplicated pregnancies explored in the study. The female fetal sex showed higher measurements for perfusion and volume than the male fetal sex and the inverse for oxygenation.
CONCLUSION
The ability to possibly predict deviation of an uncomplicated pregnancy as early as the beginning of the second trimester allows for clinical intervention as adverse outcomes can lead to increased risk of serious health conditions, including mortality for both maternal and fetus. This study explores the sensitivity of early mpMR placenta imaging to capture deviation in perfusion, volume, and oxygenation between uncomplicated and adverse pregnancies, as well as acute changes in trends within uncomplicated pregnancies that ultrasound Doppler measurements do not offer.Acknowledgements
This study could not have been possible with out the following awarded grants; NICHD: U01HD087221.References
1. Brian Lee, Carla Janzen, Arya R. Aliabadi, Margarida Y.Y. Lei, Holden Wu, Dapeng Liu, Sitaram S. Vangala, Sherin U. Devaskar, Kyunghyun Sung,Early pregnancy imaging predicts ischemic placental disease,Placenta,Volume 140,2023,Pages 90-99,ISSN 0143-4004,https://doi.org/10.1016/j.placenta.2023.07.297.(https://www.sciencedirect.com/science/article/pii/S014340042300454X)
2. Schabel MC, Roberts VHJ, Gibbins KJ, Rincon M, Gaffney JE, et al. (2022) Quantitative longitudinal T2* mapping for assessing placental function and association with adverse pregnancy outcomes across gestation. PLOS ONE 17(7): e0270360. https://doi.org/10.1371/journal.pone.0270360
3. Poon, L.C., Lesmes, C., Gallo, D.M., Akolekar, R. and Nicolaides, K.H. (2015), Prediction of small-for-gestational-age neonates: screening by biophysical and biochemical markers at 19–24 weeks. Ultrasound Obstet Gynecol, 46: 437-445. https://doi.org/10.1002/uog.14904
4. Roberts DJ, Post MDThe placenta in pre-eclampsia and intrauterine growth restrictionJournal of Clinical Pathology 2008;61:1254-1260.
Figures