0167
An MRI-visible mesenchymal stem cell therapy reinvigorates T lymphocytes in glioblastoma1Department of Radiology, Sun Yat-Sen University, Sun Yat-Sen Memorial Hospital, Guangzhou, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Keywords: Probes & Targets, MR-Guided Interventions, Glioblastoma, Mesenchymal stem cells
Motivation: Immunotherapy resistance in glioblastoma (GBM) has been linked to a paucity of tumor-infiltrating T lymphocytes and concurrent T-cell dysfunction.
Goal(s): This research aims to determine whether MRI-visible mesenchymal stem cells (MSCs) could be employed for GBM immunotherapy.
Approach: CXCL10-Nrf2-FTH-MSCs with enhanced T lymphocyte recruitment (Cxcl10 gene), oxidative stress tolerance (Nrf2 gene), and MRI visibility (Fth gene) were genetically engineered. With the guidance of FTH-MRI, these MSCs were injected into the tumor periphery of orthotopic GL261 GBMs in mice.
Results: In vivo MRI monitoring and histology examinations demonstrated that CXCL10-Nrf2-FTH-MSCs can significantly limit GBM growth by reviving T lymphocytes within the tumor.
Impact: FTH-MRI is a practical method for guiding intracranial stem cell transplantation. MRI-guided peritumoral implantation of CXCL10-Nrf2-FTH-MSCs provides a novel immunotherapeutic approach based on tumoricidal stem cells for the treatment of GBM.
Introduction
Glioblastoma (GBM) is the most prevalent and severe type of brain tumor1. Current immunotherapies for GBM frequently fail due to a deficiency of T lymphocytes and dysfunctional T cells in GBM2. CXCL10 could not only facilitate the migration of T cells to the tumor site but also drive their polarization into highly potent effector T cells3,4. Our previous study5 demonstrated that peritumoral injection is the preferred administration route for mesenchymal stem cells (MSC)-based cellular vehicles to inhibit intracranial malignant glioma growth. However, the limited survival of engrafted MSCs remains a significant barrier to their therapeutic efficacy. Nrf2 overexpression enhances MSC survival and oxidative stress tolerance6,7, which could be used to improve the effectiveness of MSC-based cell therapies. For guiding intracranial glioma stem cell transplantation, FTH-MRI is a practical method, referring to its potential for use in cellular therapy for other brain diseases8. Thus, taken together, this research aims to determine whether CXCL10-Nrf2-FTH-MSCs could be employed for continuous and targeted delivery of CXCL10 to increase tumor-infiltrating T cells, restore their function in GBM, and restrict its progression.Methods
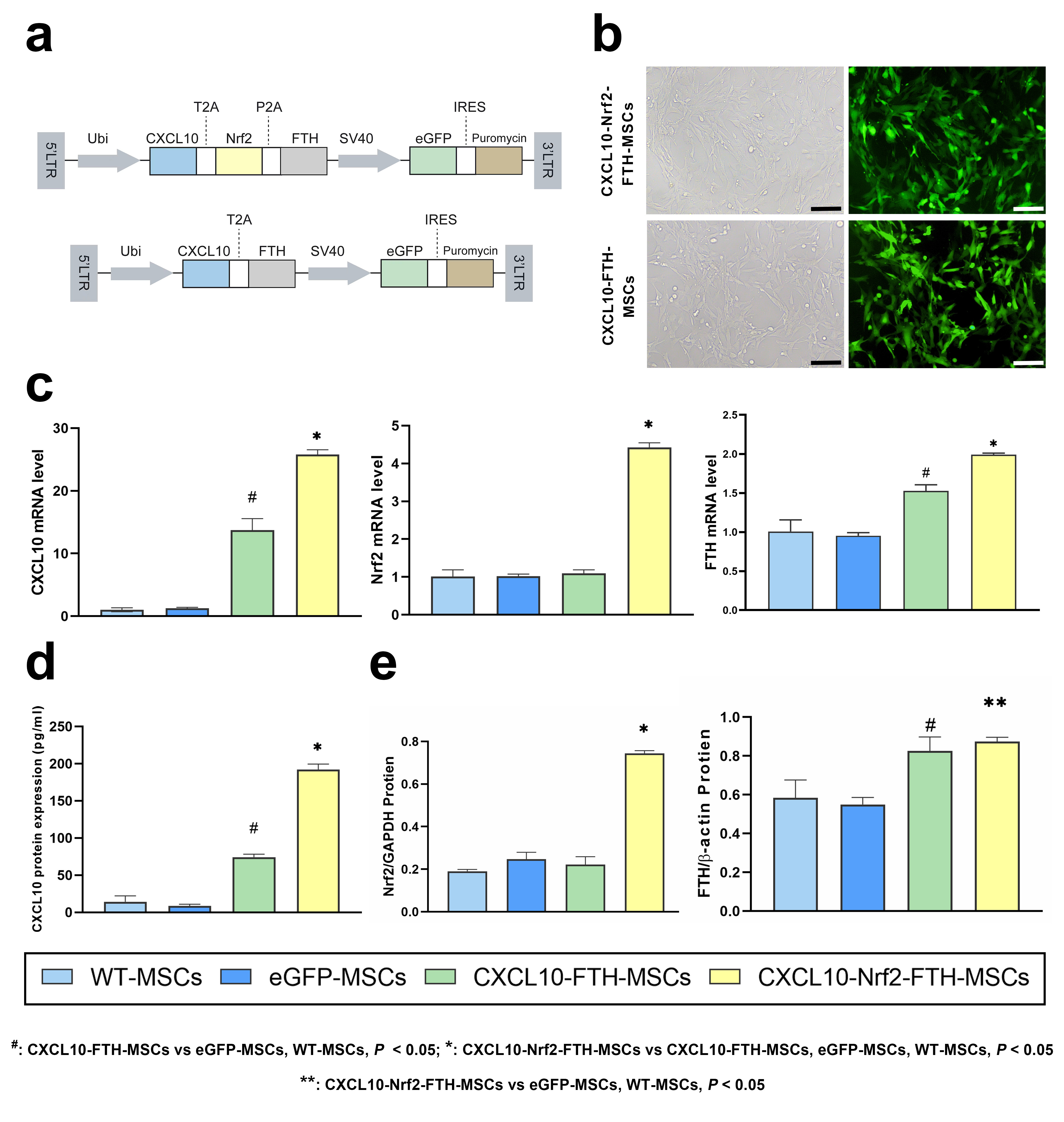
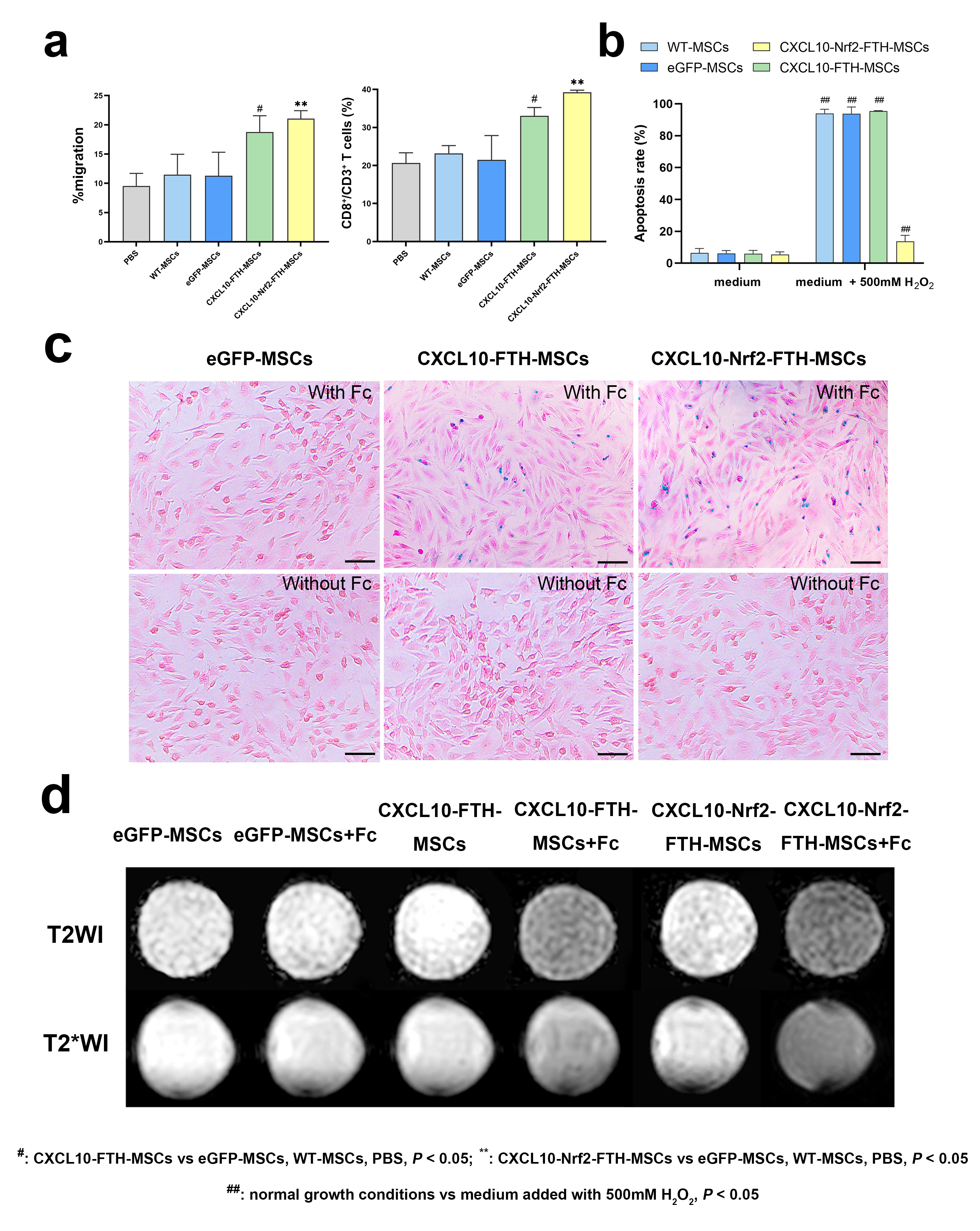
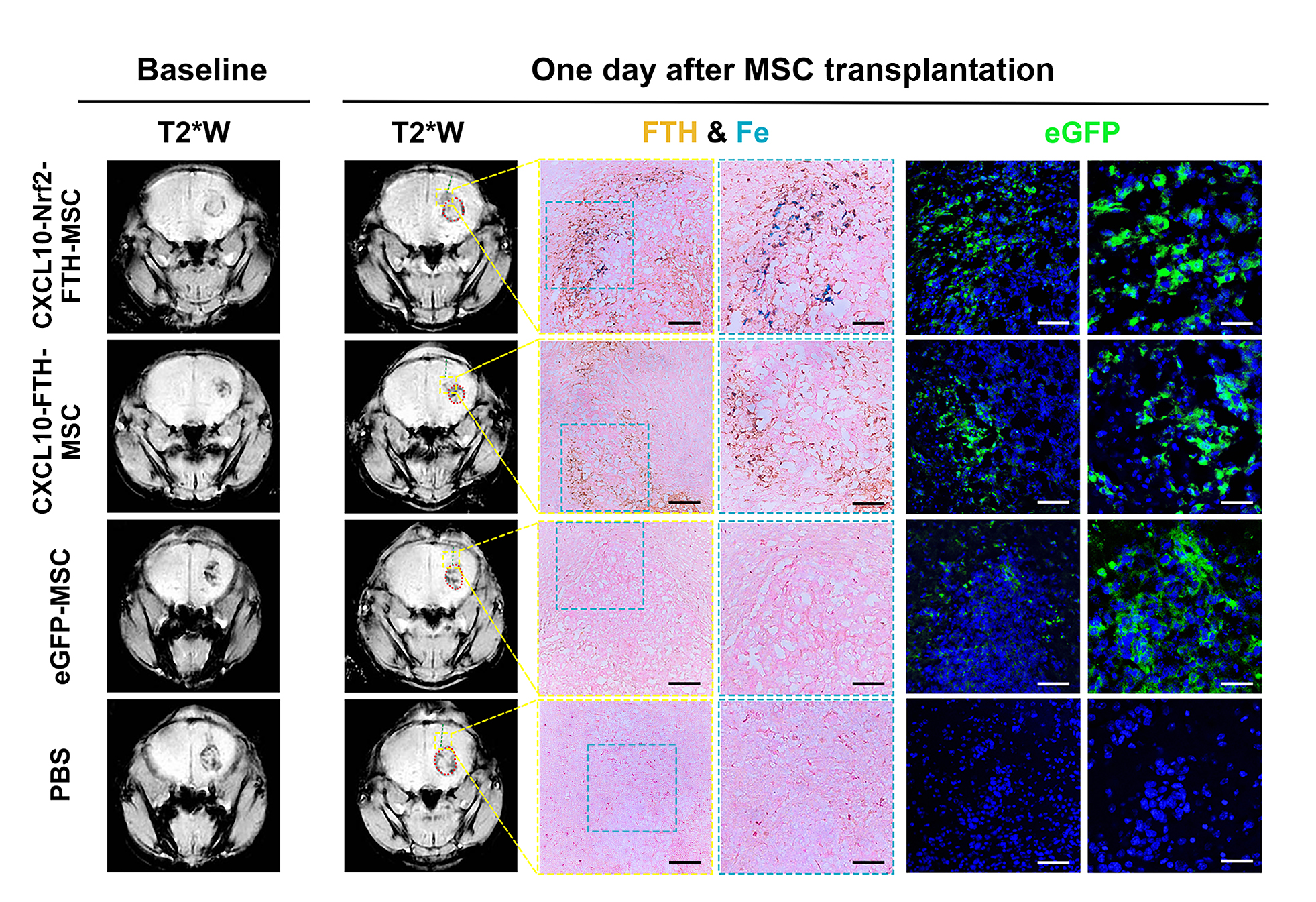
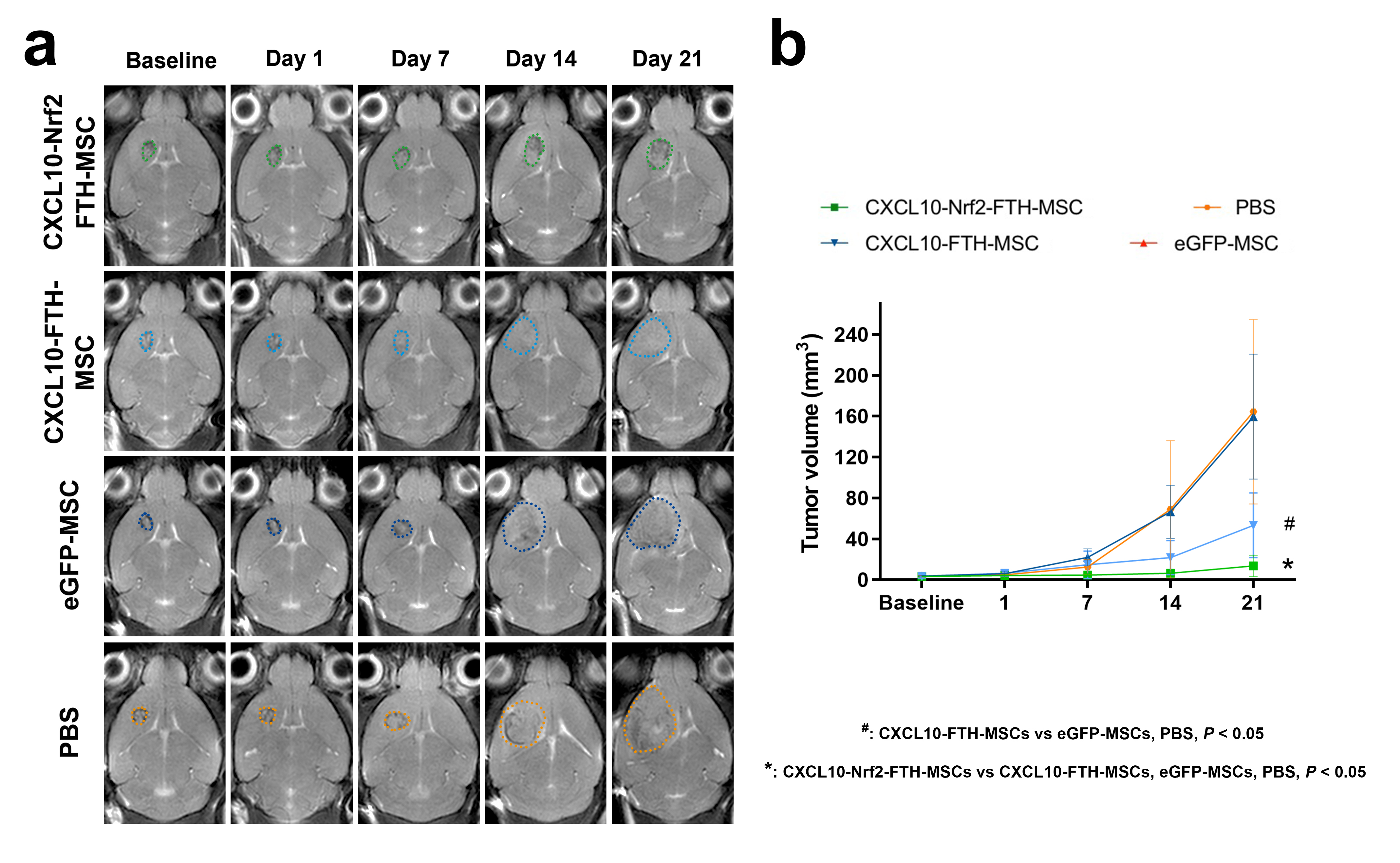
Lentiviral vectors encoding mouse Cxcl10 (NM_021274), Fth (NM_010239), and Nrf2 (NM_010902) were constructed. MSCs were transduced with LV-CXCL10-T2A-Nrf2-P2A-FTH-eGFP to obtain CXCL10-Nrf2-FTH-MSCs. CXCL10-FTH-MSCs and eGFP-MSCs were genetically engineered as controls. The mRNA and protein overexpression of Cxcl10, Nrf2, and Fth was detected using quantitative real-time PCR, ELISA, and Western blot. The transwell migration assay, H2O2-induced apoptosis assay, Prussian blue staining, and in vitro MRI were used to evaluate the overexpression of Cxcl10, Nrf2, and Fth genes in CXCL10-Nrf2-FTH-MSCs.In vivo and serial MRIs were performed to monitor the therapeutic effect of peritumoral transplantation of MSCs on orthotopic GL621 GBMs in C57/BL6 mice. MRI was performed on a clinical 3.0 T MR scanner (Ingenia; Philips Medical Systems) equipped with a 3 cm 8-channel phased array mouse coil (Suzhou Zhongzhi Medical Technologies, China). In vivo MRIs were performed at each time point of one day prior to injection (baseline), the day of injection (day 1), and 7, 14, and 21 days after injection (day 1, day 7, day 14, and day 21). CXCL10-Nrf2-FTH-MSCs were identified on T2*W images (TR/TE = 450/22 msec, flip angle = 30˚, slice thickness/gap = 1/0.1mm, FOV = 50 × 50mm2, acquisition matrix = 332 × 332, reconstruction matrix = 640 × 640, NSA = 3) on day 1 to confirm the peritumoral transplantation. The tumor volume of gliomas at each time point was measured on T2W images (TR/TE = 1600/60 msec, flip angle = 90˚, slice thickness/gap = 1/0mm, FOV = 40 × 40mm2, acquisition matrix = 268 × 268, reconstruction matrix = 512 × 512, NSA = 2) Ex vivo flow cytometry of mouse brains was performed to evaluate tumor-infiltrating T lymphocytes 21 days after MSC transplantation.
Results
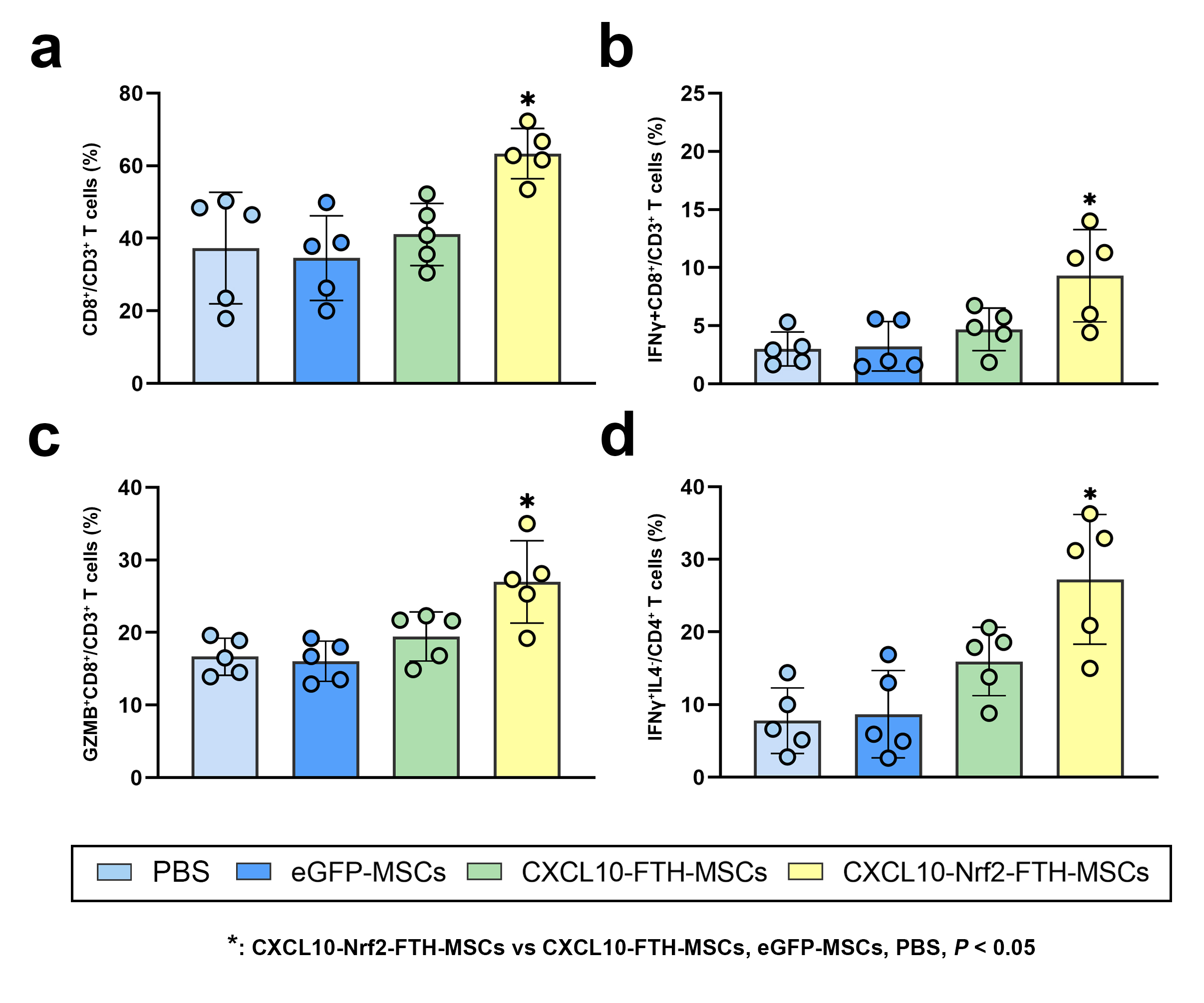
The constructed lentivirus effectively transduced MSCs to up-regulate CXCL10 secretion, Nrf2, and FTH expression (Figure 1). CXCL10-Nrf2-FTH-MSCs enhanced T lymphocyte migration, oxidative stress resistance, and cellular iron accumulation in vitro (Figure 2). Peritumoral MSC transplantation is illustrated in Figure 3, as verified by MRI and histological examinations. At baseline, GL261 gliomas exhibited a mass with a somewhat hyperintense signal and were frequently bordered by hypointense hemorrhage on T2*W images. On D01, CXCL10-Nrf2-FTH-MSCs and CXCL10-FTH-MSCs presented hypointense signals on T2*W imaging at the peritumoral zone. This is consistent with an abundance of FTH-positive and blue-stained MSCs shown on immunohistochemistry staining for FTH and Prussian blue staining, as well as an abundance of eGFP+ cells in the peritumoral area seen on eGFP immunofluorescence imaging. In vivo MRI and tumor volume growth curves (Figure 4) showed that the CXCL10-Nrf2-FTH-MSC and CXCL10-FTH-MSC groups showed significantly slower GL261 tumor growth than the other groups (P < 0.05). Comparatively, the tumor volume of the CXCL10-Nrf2-FTH-MSC group (13.68 ± 10.35 mm3) is significantly less than that of the CXCL10-FTH-MSC group (53.30 ± 31.62 mm3) (P < 0.05) on day 21. On day 21 after MSC transplantation, only GL261 tumors treated with CXCL10-Nrf2-FTH-MSCs demonstrated a significant increase in CD8+ T cells, IFN-γ+ cytotoxic T lymphocytes (CTLs), GzmB+ CTLs, and Th1 cells (P < 0.05) (Figure 5).Discussion and conclusion
Under in vivo FTH-MRI guidance and surveillance, peritumoral transplantation of CXCL10-Nrf2-FTH-MSCs inhibits orthotopic GL261 GBM tumor growth in C57/BL6 mice by enhancing tumor-infiltrating T cells and restoring T-cell function. Our study demonstrated that peritumoral administration of CXCL10 and Nrf2-overexpressed MSCs can significantly limit GBM growth, hence providing a therapeutic option for malignant gliomas. FTH-MRI could be a useful tool for guiding MSC transplantation and monitoring the therapeutic efficacy of this cellular treatment.Acknowledgements
No acknowledgement found.References
1. Tan AC, Ashley DM, López GY, et al. Management of glioblastoma: State of the art and future directions. CA Cancer J Clin. 2020;70:299-312.
2. Rahman M, Sawyer WG, Lindhorst S, et al. Adult immuno-oncology: using past failures to inform the future. Neuro Oncol. 2020;22:1249-1261.
3. Chow MT, Ozga AJ, Servis RL, et al. Intratumoral Activity of the CXCR3 Chemokine System Is Required for the Efficacy of Anti-PD-1 Therapy. Immunity. 2019;50:1498-1512.e5.
4. Mikucki ME, Fisher DT, Matsuzaki J, et al. Non-redundant requirement for CXCR3 signalling during tumoricidal T-cell trafficking across tumour vascular checkpoints. Nat Commun. 2015;6:7458.
5. Mao J, Cao M, Zhang F, et al. Peritumoral administration of IFNβ upregulated mesenchymal stem cells inhibits tumor growth in an orthotopic, immunocompetent rat glioma model. J Immunother Cancer. 2020;8:e000164.
6. Mohammadzadeh M, Halabian R, Gharehbaghian A, et al. Nrf-2 overexpression in mesenchymal stem cells reduces oxidative stress-induced apoptosis and cytotoxicity. Cell Stress Chaperones. 2012;17:553-565.
7. Yuan Z, Zhang J, Huang Y, et al. NRF2 overexpression in mesenchymal stem cells induces stem-cell marker expression and enhances osteoblastic differentiation. Biochem Biophys Res Commun. 2017;491:228-235.
8. Kim HS, Cho HR, Choi SH, et al. In vivo imaging of tumor transduced with bimodal lentiviral vector encoding human ferritin and green fluorescent protein on a 1.5T clinical magnetic resonance scanner. Cancer Res. 2010;70:7315–7324.
Figures