0154
Field Cycling Imaging: a novel very low field modality to characterize breast cancer1Aberdeen Biomedical Imaging Centre, University of Aberdeen, Aberdeen, United Kingdom, 2Institute of Biomedical Imaging, Graz University of Technology, Graz, Austria, 3Institute of Medical Sciences, University of Aberdeen, Aberdeen, United Kingdom, 4Breast Unit, Aberdeen Royal Infirmary, Aberdeen, United Kingdom, 5University Grenoble Alpes, Inserm U1205, BrainTech Lab, Grenoble, France
Synopsis
Keywords: Low-Field MRI, Low-Field MRI, breast cancer
Motivation: Field Cycling Imaging (FCI) has never been used in clinics and its capability in medical diagnosis has not yet demonstrated.
Goal(s): Our goal was to demonstrate the capabilities of FCI as an imaging modality to diagnose breast cancer by measuring the T1 variations at low field from 2.3 to 200 mT.
Approach: Ten patients were imaged with our recent FCI prototype scanner and images were compared with standard clinical imaging and histology.
Results: FCI provides relevant biomarkers of molecular dynamics that detect tumours and discriminate invasive from non-invasive tumours. In addition, FCI is insensitive to breast density and provides accurate tumour delineation.
Impact: FCI, which uses variant low field strengths, could complement clinical imaging without contrast agents non-invasively and could improve the estimation of tumour size and resection margins, even for dense breasts, including DCIS which is often under/over-estimated in clinical imaging.
Introduction
Standard breast cancer imaging (ultrasound, mammography and MRI) has limitations to delineate tumour margins accurately. Field-Cycling imaging (FCI)1 is a novel modality that can image over a range of low magnetic field strengths through rapid switching between magnetic field levels. This allows measuring the field-depended changes of the longitudinal T1 relaxation time (or R1=1/T1), known as nuclear magnetic relaxation dispersion (NMRD). NMRD profiles provide information on molecular dynamics exploiting novel biomarkers that recently have been shown in breast cancer and glioma models2,3. Our aim was to demonstrate the capabilities of FCI in clinics for breast cancer and to confirm biomarkers, as observed preclinically in vitro and in vivo.Methods
Twenty-six females with breast cancer were recruited from January 2019 to March 2022 (ethics approved by NoSREC, number 19/NS/0064). Ten patients (mean age, 53 years ± 10) with various tumour types and BIRAD scores completed the study. Patients were diagnosed with Invasive Ductal Carcinoma (n=1), Ductal Carcinoma In Situ (DCIS, n=5), borderline phyllodes (n=1) and mixed phenotypes (n=3). One patient presented two distinct lesions at histology and each lesion was analysed separately (n=11 data).FCI was performed with four evolution fields (200, 65.8, 22 and 2.3mT) using a single-slice inversion recovery spin echo sequence with five evolution times (Fig. 1). The slice thickness was set to 10mm and the in-plane resolution to 2 to 4mm, depending on the FOV with matrix size of 64x128. The total duration of the FCI examination was 45min. Clinical imaging including ultrasound, mammography, and in four cases MRI at 1.5T were used for comparison. Routine clinical histopathological Hematoxylin Eosin (HE) analysis was conducted at the excised lesion after surgery as per standard practice and used for validation. Tumour sizes in FCI images were calculated using ImageJ4 and measured as per standard procedures for other imaging modalities. All were compared to HE histology using the difference in size between imaging and HE histology divided by size from HE histology in %.
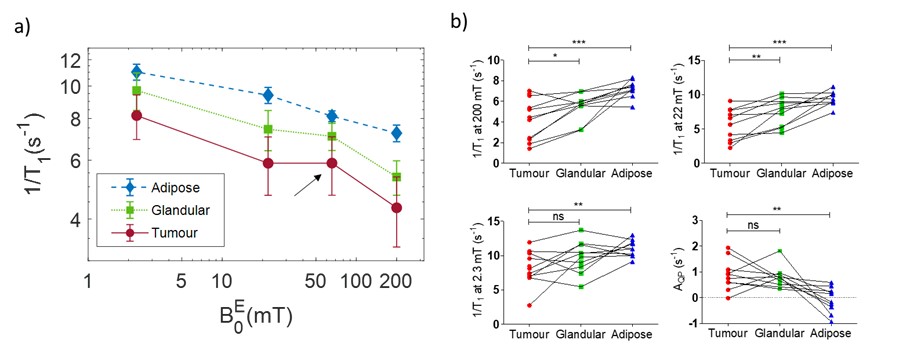
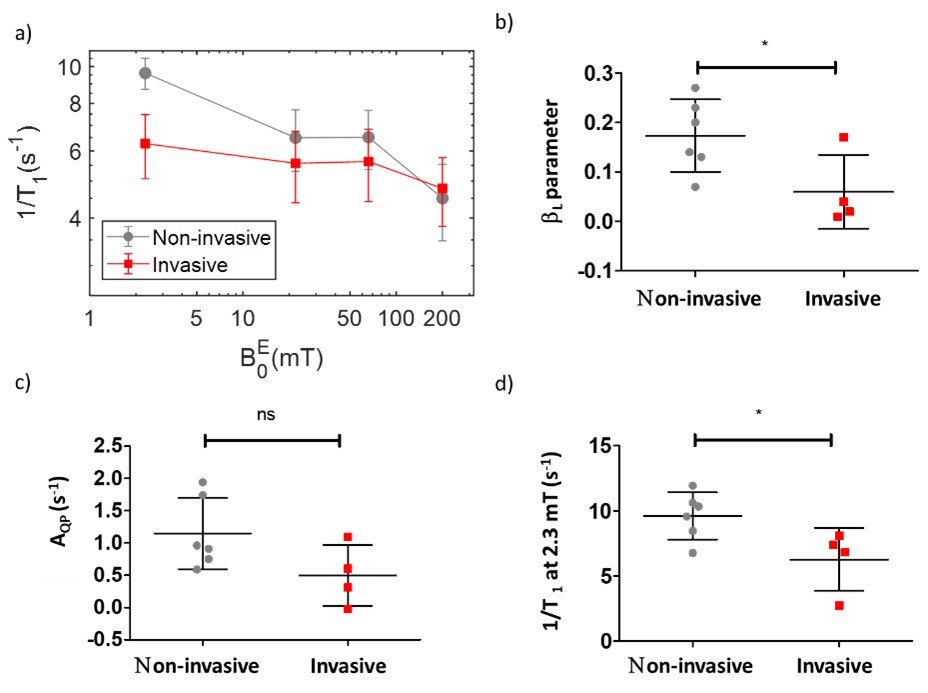
Data analysis was performed in MATLAB using in-house software. 1/T1 quantification was conducted using the monoexponential model derived from the Bloch equations to fit the magnetization recovery across field strengths. The 1/T1 NMRD profiles were fitted using a power law model (1/T1=αB-β) to derive the slope of the dispersion (β parameter) at fields below (βL) and above (βH) 22 mT. The amplitude of the quadrupolar peak (QP) at 65.8mT, which corresponds to the 14N-1H quadrupolar coupling between nitrogen 14 of proteins and water protons, was estimated by interpolation. NMRD dispersions were extracted from three ROIs: tumour from the diseased breast, adipose and glandular breast tissue from the contralateral breast.
Results
The tumour region was easily visible by FCI and exhibited hyper-intense regions (Fig.2). FCI tumour sizes were found close to those obtained from histology (38±12mm vs 37±12mm). This was not the case for the other imaging modalities for which 5 out of 8 DCIS cases were severely under/over-estimated by clinical imaging (Fig. 3). Tumour 1/T1 values were significantly lower from glandular and adipose tissue (p<0.05). The relaxation enhancement due to 14N-1H QP coupling at 65.8 mT was significantly larger in tumours than in breast tissues (0.85±0.44s-1 vs -0.07±0.49s-1, p<0.001) (Fig.4). Further segmentation of the tumour NMRD profiles showed significant differences between non-invasive and invasive tumours (Fig. 5). These appear both in 1/T1 values at 2.3 mT (9.6±1.8 s-1 vs 6.3±2.4s-1, p<0.05) and in the low-field slope βL of the 1/T1-NMRD (0.17±0.07 vs 0.06±0.08, p<0.05).Discussion
This is the first time that 1/T1-NMRD profiles acquired by FCI at very low field below 0.2T are extracted from breast cancer patients in vivo. Despite the low spatial resolution, FCI located accurately the lesions and provided non-biased size estimates, as validated by histology. FCI did not present issues with breast density for the patients scanned despite the range of BIRADs. 1/T1-NMRD profiles successfully discriminated between tumours and healthy tissues. The slope of the dispersion and 1/T1 at 2.3mT discriminated between invasive and non-invasive tumours suggesting rapid transmembrane water exchange and water molecular dynamics in case of invasion2,3.Conclusion
FCI shows high potential for breast tumour detection without need of contrast agent with potentially better delineation in DCIS. We also found relevant biomarkers of breast cancer invasiveness, which is of high interest for surgery planning and could improve the outcome of patient treatment if confirmed.Acknowledgements
The authors would like to thank radiographers Nichola Crouch, Mike Hendry, Laura Reid, Michelle Mauchline, and Arthur Ginsburg for their support with patient scans of FCI, Stacey Dawson for the study coordination, and the clinical teams of the Royal Aberdeen Infirmary for their support, in particular Sue Rodwell, Lorraine Drage, Farah Muir, Vera Hord and Dr Mairi Fuller for their help with patient recruitment. This project has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement No 668119 (project “IDentIFY”), as well as from the NHS Grampian Endowment Trust.References
1. Broche, L. M., Ross, P. J., Davies, G. R., MacLeod, M. J., & Lurie, D. J. A whole-body Fast Field-Cycling scanner for clinical molecular imaging studies. Sci Rep.2019;9(1), 10402.
2. Petit, M., Leclercq, M., Pierre, S., Ruggiero, M. R., El Atifi, M., Boutonnat, J., Fries, P. H., Berger, F., & Lahrech, H. Fast-field-cycling NMR at very low magnetic fields: water molecular dynamic biomarkers of glioma cell invasion and migration. NMR in Biomedicine, 2022;35(6), e4677.
3. Ruggiero, M. R., Ait Itto, H., Baroni, S., Pierre, S., Boutonnat, J., Broche, L. M., Aime, S., Berger, F., Geninatti Crich, S., & Lahrech, H Role of Transmembrane Water Exchange in Glioma Invasion/Migration: In Vivo Preclinical Study by Relaxometry at Very Low Magnetic Field. Cancers, 2022;14(17), 4180.
4. Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years of image analysis. Nat Methods. 2012;9(7):671–5.
Figures
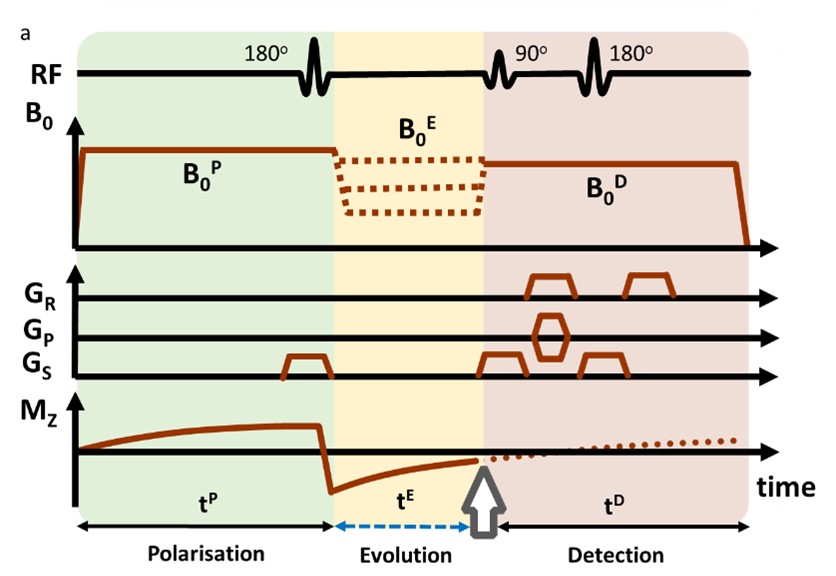
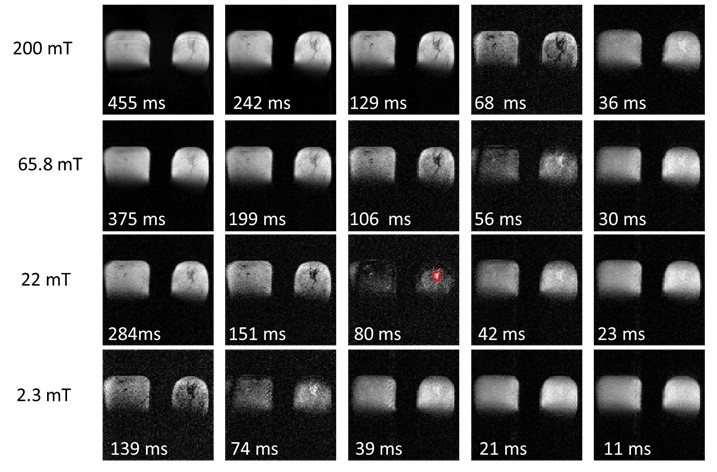
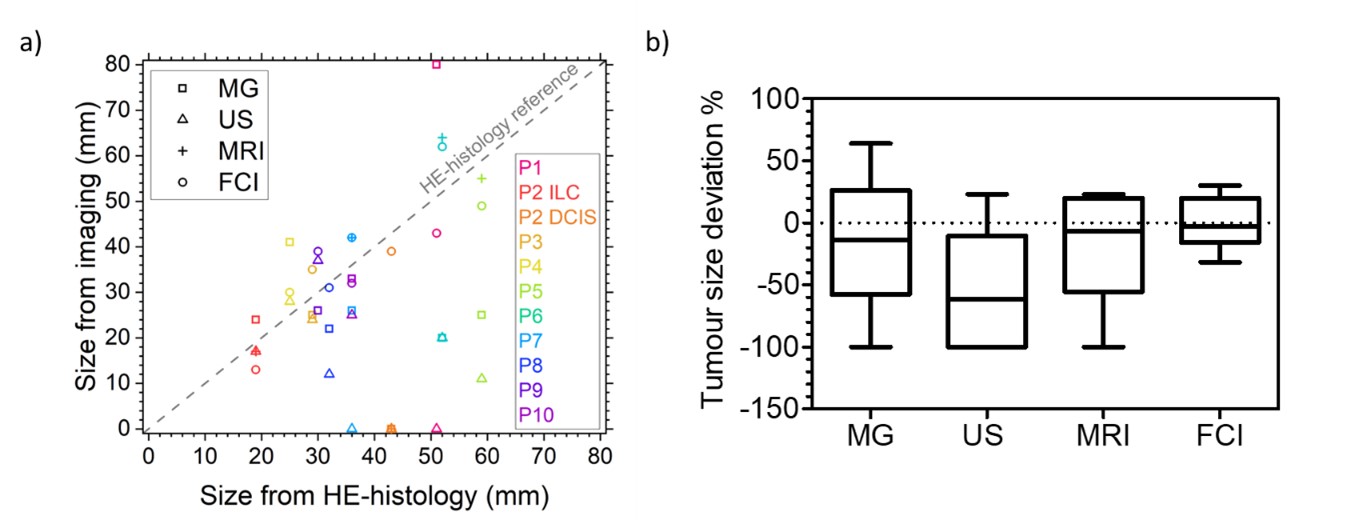
Figure 3. Tumour size estimation. a) Tumour size as measured by each imaging modality compared to the reference size obtained with HE histology. Colours and shapes are sorted by patient and imaging modality respectively. b) Tumour size deviation in mammography (MG), ultrasound (US), MRI, and FCI from HE histology in %. FCI tumour sizes were closer to measurements from HE histology compared with US, MG and MRI.