0148
Reduced gadolinium dose by an optimized multi-parametric MR-STAT protocol1Computational Imaging Group for MR diagnostics & therapy, Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 2Department of Radiology and Nuclear Medicine, Amsterdam University Medical Center, Vrije Universiteit Amsterdam, Amsterdam, Netherlands, 3Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 4Department of Medical Imaging, Radboud University Medical Center, Nijmegen, Netherlands, 5Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 6Department of Neurology and Neurosurgery, UMC Utrecht Brain Center, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
Keywords: Quantitative Imaging, Quantitative Imaging, MR-STAT; Contrast Enhancement Imaging
Motivation: Several concerns have been raised about the harmful effects of gadolinium-based contrast agent (GBCA) usage during MRI exams.
Goal(s): To reduce the GBCA dose in MRI protocols.
Approach: We developed an optimized and fast MR-STAT protocol for “pre- and post-injection” quantitative MRI and applied it to two retrospective simulated patient datasets and one prospective in-vivo scan.
Results: The inferred lesion masks generated by comparing “pre- and post-injection” T1 maps demonstrated that the proposed relaxometry-based method was able to correctly detect the lesions. Furthermore, the performance for the low-dose protocol was comparable to that of the full-dose one.
Impact: The quantification of T1 changes after administering GBCA by using the accelerated MR-STAT protocol potentially enables a substantial reduction in both GBCA dose and acquisition time in clinical protocols.
Introduction
A range of concerns1-4 has been raised over the harmful effects of gadolinium-based contrast agents (GBCA) usage during MRI exams. In this work, we present a strategy to substantially reduce the GBCA dose which is based on the fact that T1/T2 values of pathological tissue change after GBCA administration5. Therefore, tissue lesions may be detected by comparing relaxometry maps acquired before and after GBCA injection. We hypothesize that this quantification process is sensitive enough to detect T1/T2 changes (i.e., pathological tissue) even with a substantially reduced GBCA dose.We developed a fast MR-STAT6 protocol for “pre- and post-injection” quantitative MRI (qMRI) and applied it to two retrospective simulated patient datasets7 and one prospective in vivo scan. We show that the proposed method allows for accurate lesion detection by using just 20% of the standard GBCA dose.
Methods
Protocol designThe effect of GBCA on the MR signal in the brain is usually limited to pathological tissue (enhancement region). As such, we can effectively leverage the strong correlation between “pre- and post-injection” quantitative tissue properties to accelerate the “post-injection” qMRI acquisition.
The proposed accelerated MR-STAT protocol encompasses four key steps (Figure 1):
Step 1: Fully-sampled “pre-injection” (10 seconds) and accelerated 25% keyhole8 “post-injection” (2.5 seconds) MR-STAT acquisitions;
Step 2: K-space combination of “pre- and post-injection” k-space data by integrating the high spatial frequency data from the “pre-injection” acquisition with the registered keyhole k-space;
Step 3: High-resolution MR-STAT reconstruction of T1 and T2 maps for both “pre- and post-injection” acquisitions9;
Step 4: Lesion mask generation by thresholding the relative difference in T1 map.
As significant contrast agent induced changes occur mainly in the low-frequencies of k-space following the GBCA injection8, we designed a sampling pattern to first encode all the low frequencies, followed by the acquisition of the high frequencies’ components (only for the “pre-injection”, fully-sampled scan). We subsequently optimized an RF pulse sequence simultaneously for “pre- and post-injection” acquisitions using this sampling pattern10, see Figure 2.
Given the predominant impact of GBCA on T1 shortening, our analysis primarily focuses on T1 changes.
Retrospective and simulated data
To validate the relaxometry-based, low-dose protocol, we retrospectively selected two MR-STAT tumor datasets 8 with manually segmented lesions. The quantitative T1 and T2 maps from these datasets were used as “pre-injection” data. Subsequently, we simulated the effect of a GBCA injection by calculating the expected decrease in T1 and T2 values in lesion areas for two gadobutrol concentration levels (0.7mM for full-dose and 0.14mM for low-dose) on each patient5,11,12. These “pre-injection” and simulated “post-injection” relaxometry maps were used to numerically simulate and validate the envisioned protocol (see Figure 1-2).
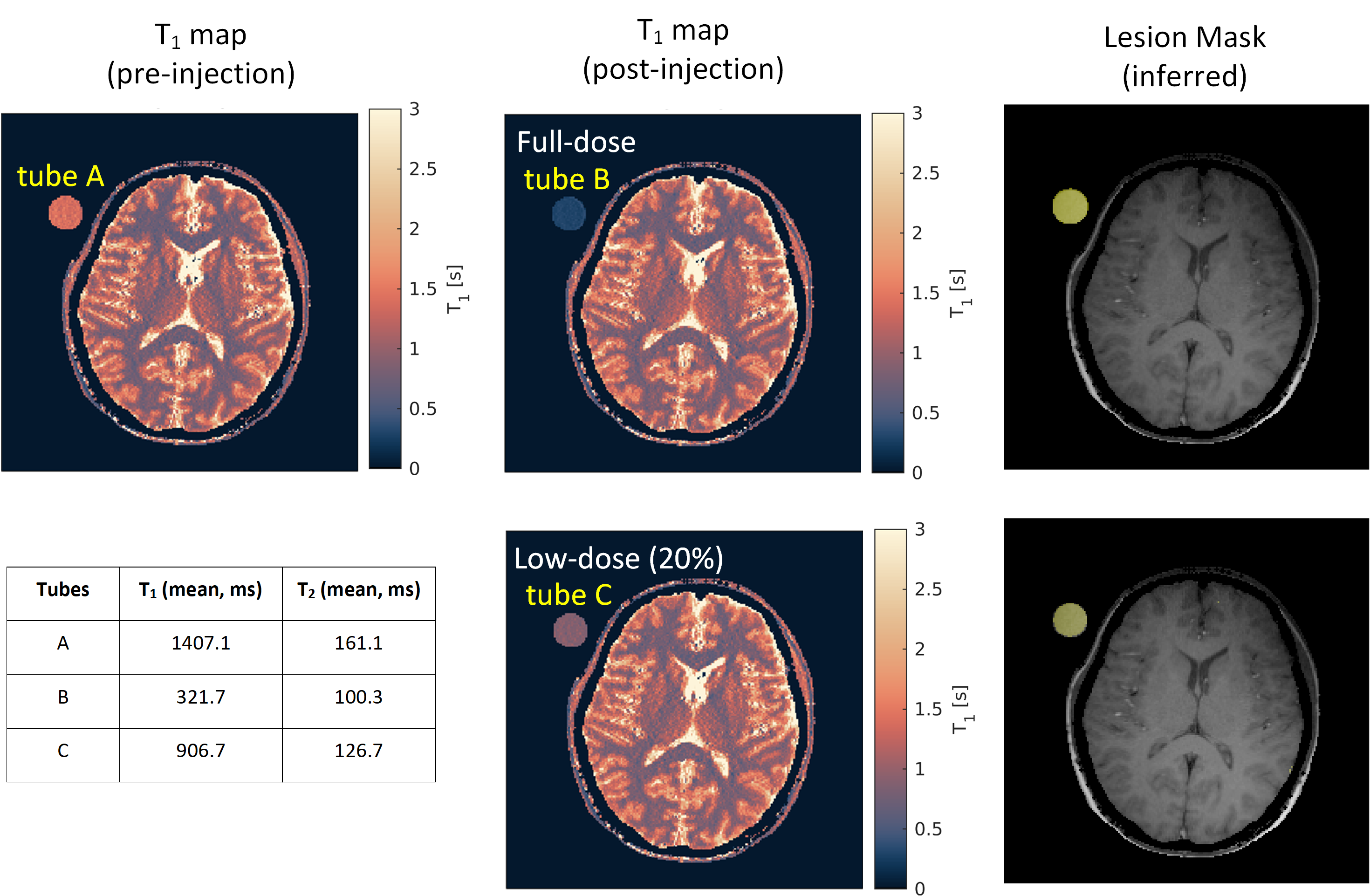
Prospective in vivo experiment
Prospective relaxometry measurements were conducted on a Philips 3T MR scanner. A Eurospin gel tube (tube A, T1 = 1407.1 ms) was placed in close proximity of the head of a healthy volunteer to simulate “pre-injection patient data” (tube A mimics the tumor tissue before injection). After the “pre-injection” scan, the “lesion” tube was replaced with another Eurospin gel tube (tube B, T1 = 321.7 ms) to mimic a “post-injection” acquisition with full GBCA dose. As a comparison, we also replaced the “lesion” tube by another Eurospin gel tube (tube C, T1 = 906.7 ms) to mimic a “post-injection” acquisition with low GBCA dose (20%).
The imaging parameters for all tests were: slice thickness: 3 mm; FOV: 224×224 mm2; in-plane resolution: 1×1 mm2; acquisition time: 10 s for “pre-injection” and 2.5 s for “post-injection” per slice.
Results
Figure 3 and Figure 4 display the T1 maps for each “pre-injection”, low-dose “post-injection”, and full-dose “post-injection” from the representative slice of the simulated tumor patients. The inferred lesion masks were generated by thresholding the relative difference between “pre- and post-injection” T1 maps, revealing high whole-brain Dice scores with respect to ground-truth. “Pre- and post-injection” (full and low-dose) results for the prospective in-vivo test are shown in Figure 5.Discussion and Conclusion
We implemented and evaluated an optimized and fast MR-STAT protocol aimed at reducing GBCA dose in a very short acquisition time (12.5 seconds per slice in this study) using retrospective and prospective tests. These preliminary results reveal that quantitative T1 changes comparable to administering a lower (20%) dose of GBCA can be detected, potentially enabling a substantial reduction in both GBCA dose and acquisition time in clinical protocols. In future work, prospective in vivo patient validation will be performed. Furthermore, accelerated 3D acquisitions will be tested. We expect that this may allow even lower dose injection given the higher SNR in 3D acquisitions13.Acknowledgements
This work has been financed by the Netherlands Organization for Scientific Research (NWO), HTSM Grant 17986.References
1. McDonald RJ, McDonald JS, Kallmes DF, et al. Gadolinium deposition in human brain tissues after contrast-enhanced MR imaging in adult patients without intracranial abnormalities. Radiology. 2017;285(2): 546-554.
2. Rogowska J, Olkowska E, Ratajczyk W, Wolska L. Gadolinium as a new emerging contaminant of aquatic environments. Environ Toxicol Chem. 2018;37(6):1523- 1534.
3. Shankar PR, Parikh K, Davenport MS. Financial implications of revised ACR guidelines for estimated glomerular filtration rate testing before contrast- enhanced MRI. J Am Coll Radiol. 2018;15(2):250- 257.
4. Ramalho J, Semelka RC, Ramalho M, et al. Gadolinium-based contrast agent accumulation and toxicity: an update. AJNR Am J Neuroradiol. 2016;37:1192–1198
5. Lauffer RB. Paramagnetic metal complexes as water proton relaxation agents for NMR imaging: theory and design. Chem Rev. 1987;87(5):901-927.
6. Sbrizzi A, van der Heide O, Cloos M, et al. Fast quantitative MRI as a nonlinear tomography problem. Magn Reson Imaging. 2018;46:56–63.
7. Kleinloog JPD, Mandija S, D'Agata F, Liu H, van der Heide O, Koktas B, Jacobs SM, van den Berg CAT, Hendrikse J, van der Kolk AG, Sbrizzi A. Synthetic MRI with Magnetic Resonance Spin TomogrAphy in Time-Domain (MR-STAT): Results from a Prospective Cross-Sectional Clinical Trial. J Magn Reson Imaging. 2023;57(5):1451-1461.
8. van Vaals JJ, Brummer ME, Dixon WT, Tuithof HH, Engels H, Nelson RC, Gerety BM, Chezmar JL, den Boer JA. "Keyhole" method for accelerating imaging of contrast agent uptake. J Magn Reson Imaging. 1993;3(4):671–675.
9. Liu H, Heide OV, Mandija S, Berg CATV, Sbrizzi A. Acceleration strategies for MR-STAT: Achieving high-resolution reconstructions on a desktop pc within 3 minutes. IEEE Trans Med Imaging. 2022;41(10): 2681-2692.
10. Fuderer M, van der Heide O, Liu H, Berg CATV, Sbrizzi A. Efficient performance analysis and optimization of transient-state sequences for multi-parametric MRI. NMR in Biomedicine. 2023;36(3): e4864.
11. Pintaske J, Martirosian P, Graf H, et al. Relaxivity of gadopentetate dimeglumine (Magnevist), gadobutrol (Gadovist), and gadobenate dimeglumine (MultiHance) in human blood plasma at 0.2, 1.5, and 3 Tesla. Investigative radiology. 2006;41(3): 213-221.
12. Fujita S, Nakazawa M, Hagiwara A, et al. Estimation of gadolinium-based contrast agent concentration using quantitative synthetic MRI and its application to brain metastases: a feasibility study. Magnetic Resonance in Medical Sciences, 2019;18(4): 260-264.
13. Liu H, Heide OV, Versteeg E, et al. A three-dimensional MR-STAT protocol for high-resolution multi-parametric quantitative MRI. NMR in Biomedicine. 2023;e5050. https://doi.org/10.1002/nbm.5050.
Figures
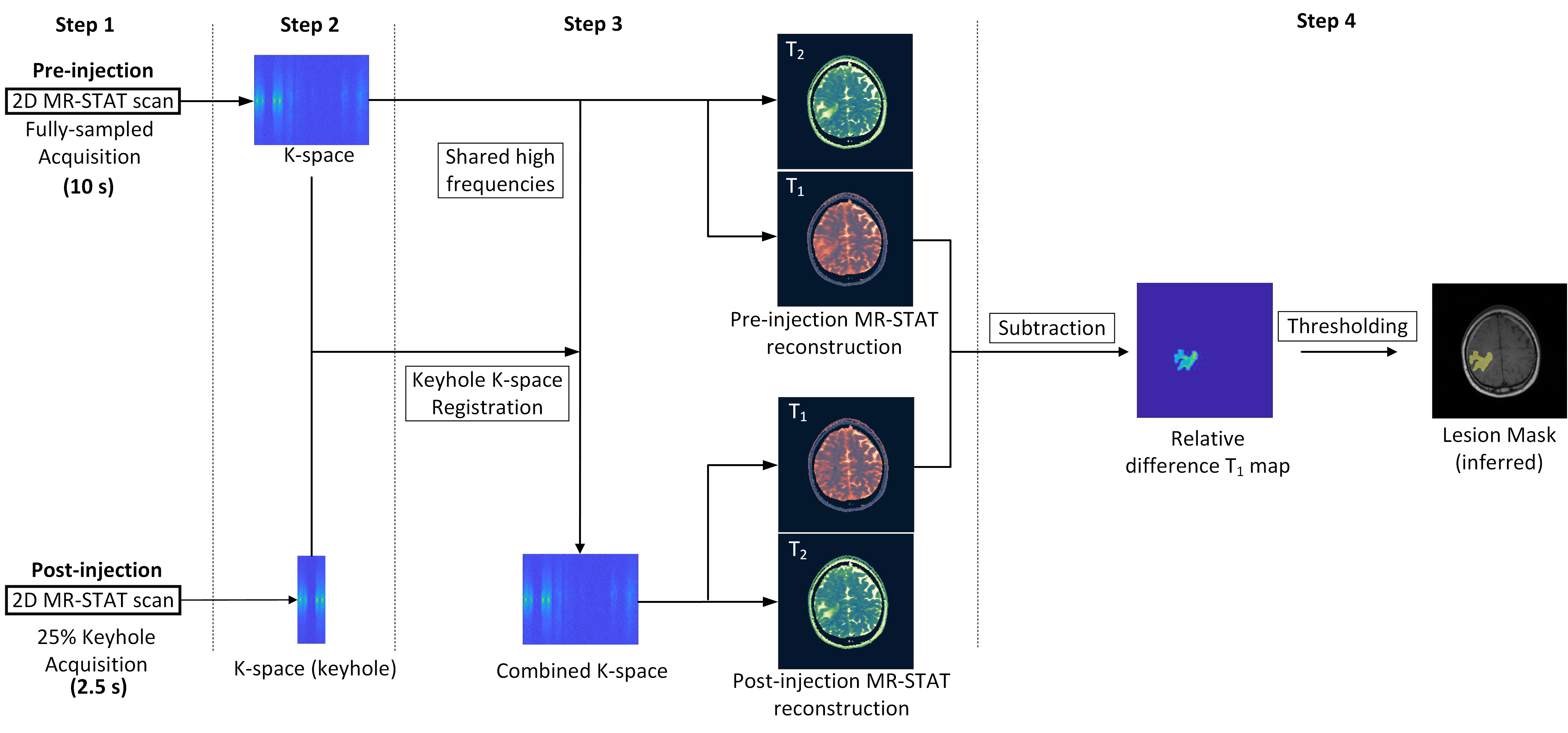
Figure 1. Flowchart of the reduced GBCA dose MR-STAT protocol.
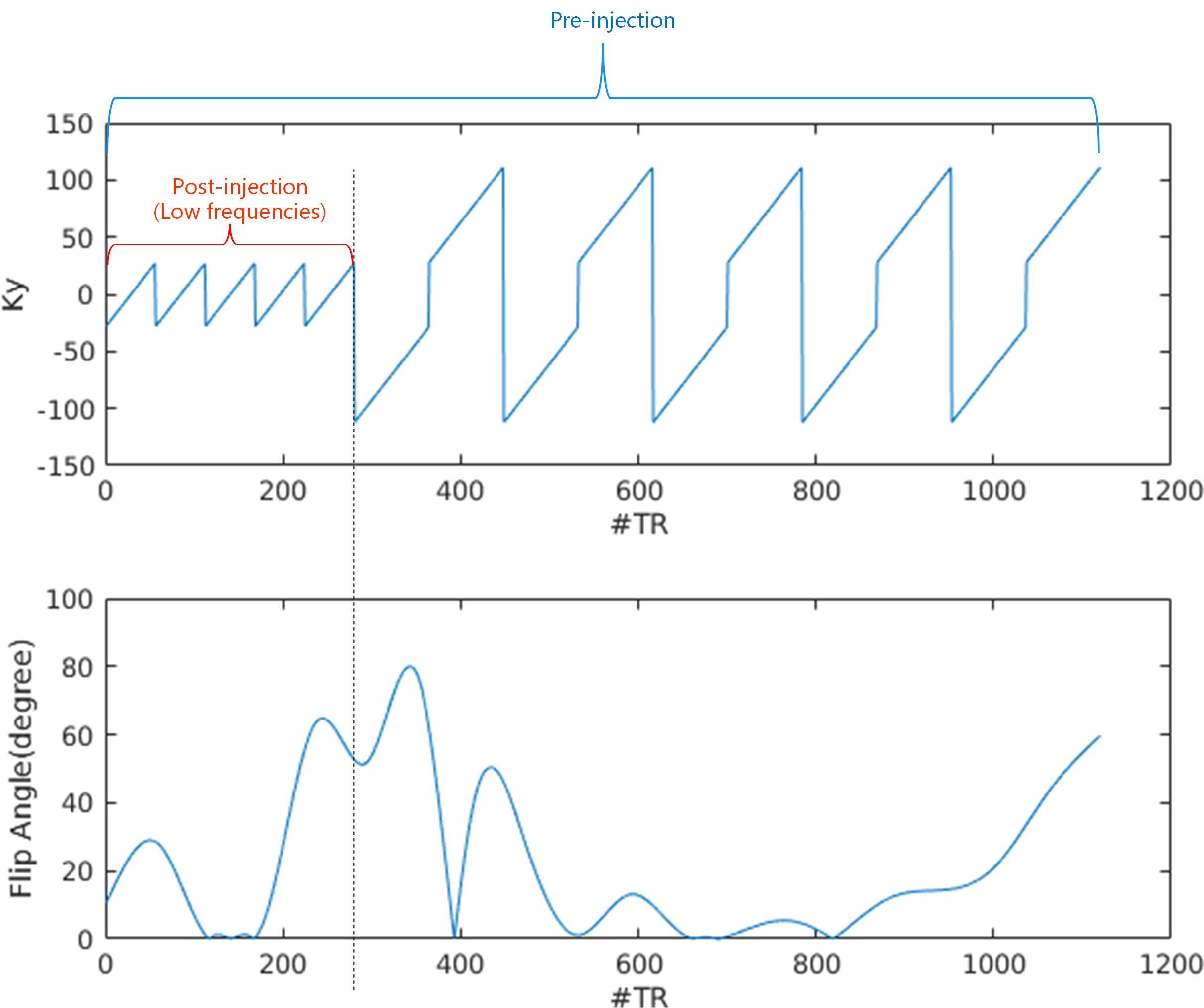
Figure 2. Sampling pattern and flip angle train scheme used in the optimized MR-STAT protocol. Note that after the GBCA injection only the low frequency segment (first 280 repetitions) is applied.
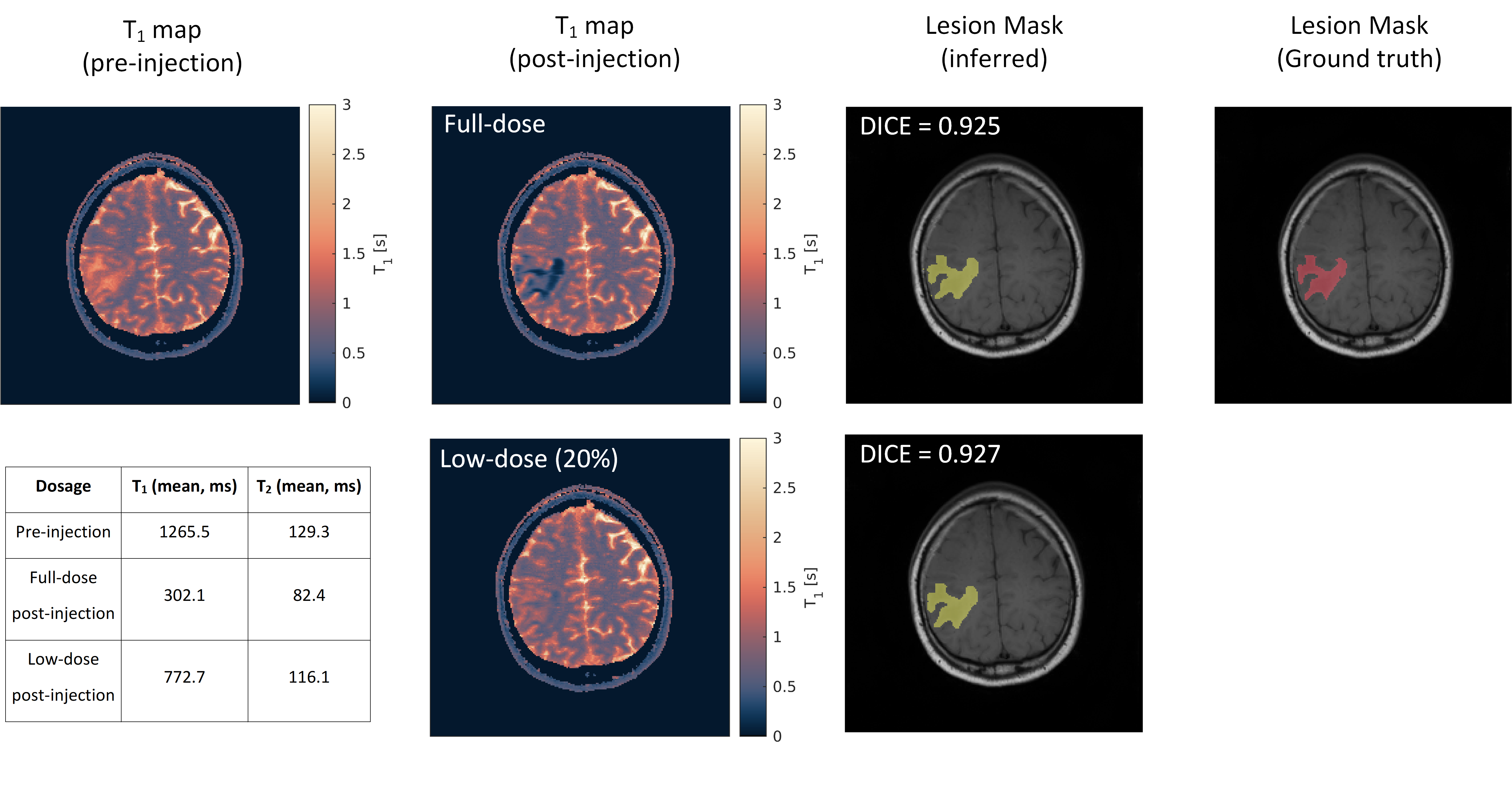
Figure 3. T1 maps of simulated data from the first tumor patient with different simulated dosages of GBCA by applying the optimized MR-STAT protocol. The values in the table are the ground truth of the simulated “pre- and post-injection” parameters in the lesion area. Note that the inferred lesion mask was generated by thresholding the relative difference between “pre- and post-injection” T1 maps. The reconstructed T2 maps are not shown.
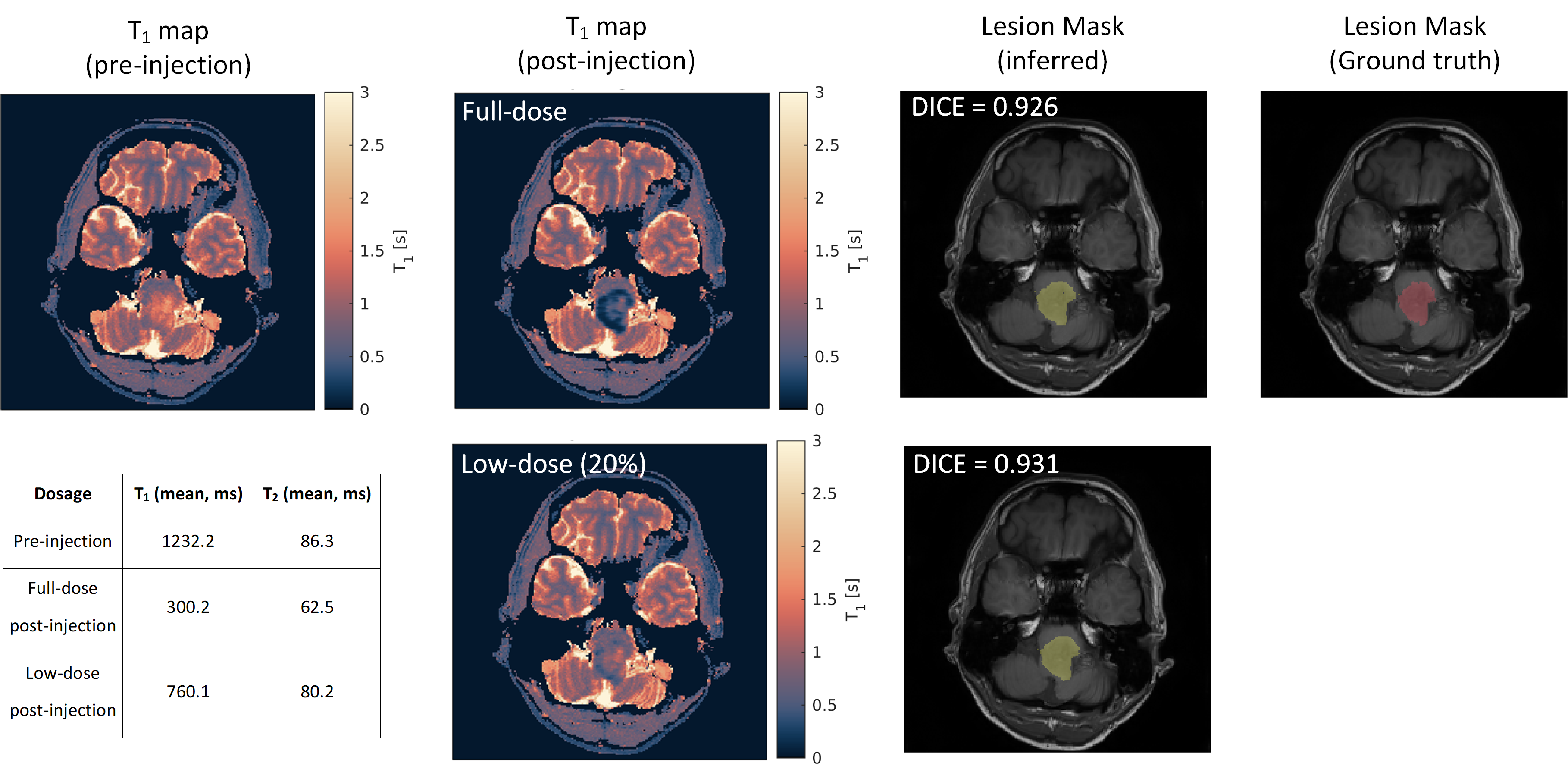
Figure 4. T1 maps of simulated data from the second tumor patient with different simulated dosages of GBCA by applying the optimized MR-STAT protocol. The values in the table are the ground truth of the simulated “pre- and post-injection” parameters in the lesion area. Note that the inferred lesion mask was generated by thresholding the relative difference between “pre- and post-injection” T1 maps. The reconstructed T2 maps are not shown.