0126
Multiple advanced diffusion models for preoperative prediction of macrotrabecular-massive subtype in solitary hepatocellular carcinoma1Department of Diagnostic Radiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2MR Research Collaboration, Siemens Healthineers, Beijing, China, 3Shanghai Key Laboratory of Magnetic Resonance, East China Normal University, Shanghai, China
Synopsis
Keywords: Microstructure, Diffusion/other diffusion imaging techniques, Tumor
Motivation: Pretherapeutic characterization of the aggressive macrotrabecular-massive (MTM) subtype hepatocellular carcinoma (HCC) may promote the implementation of precision treatment and improvement of prognosis.
Goal(s): To investigate the value of multiple advanced diffusion models in identifying the MTM subtype of HCC preoperatively.
Approach: DWI of twelve b-values (0-2000 s/mm2) were performed in 70 patients with HCC. Multiple diffusion-derived parameters were extracted and compared between MTM and non-MTM HCC. The predictive efficacy of various diffusion parameters was assessed.
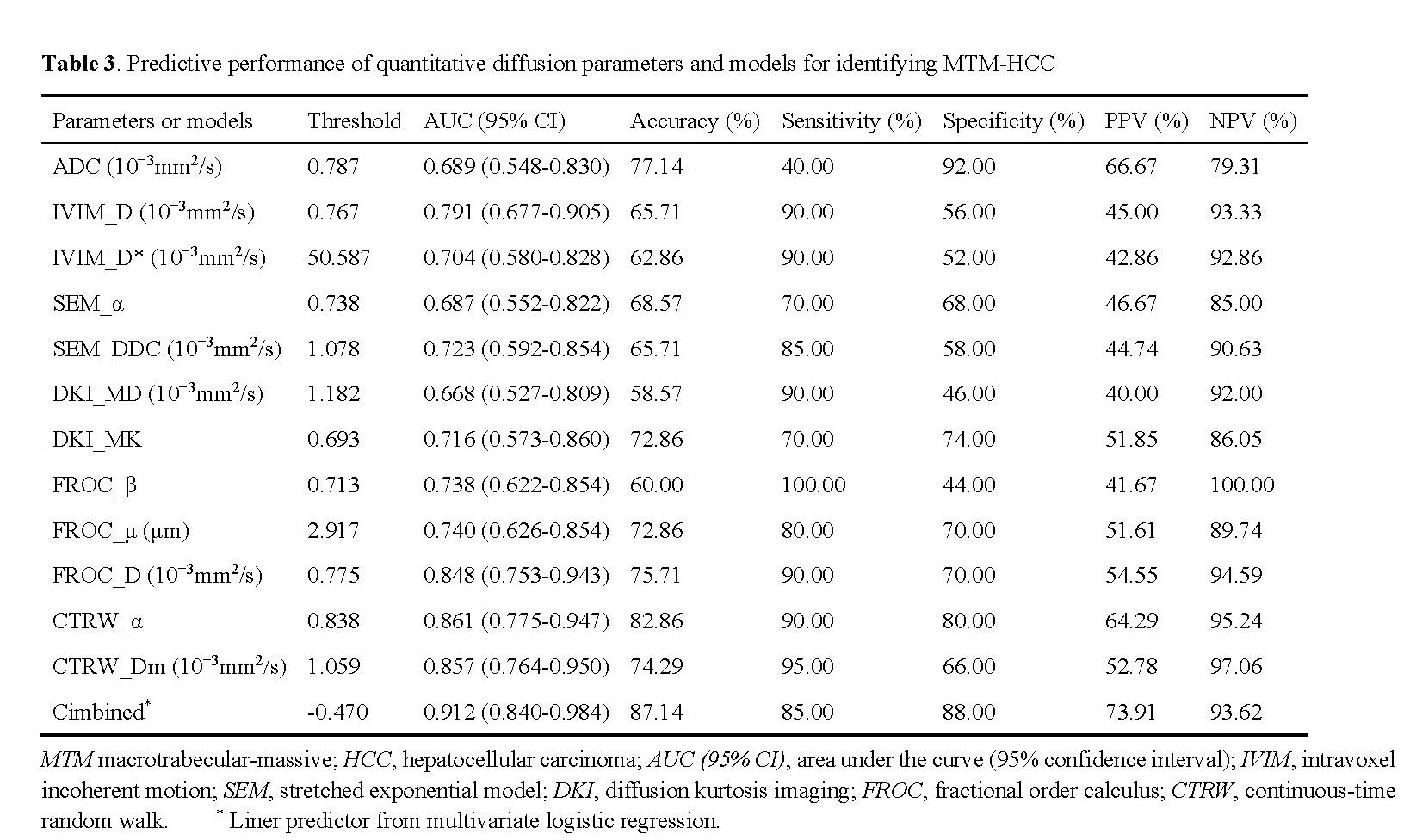
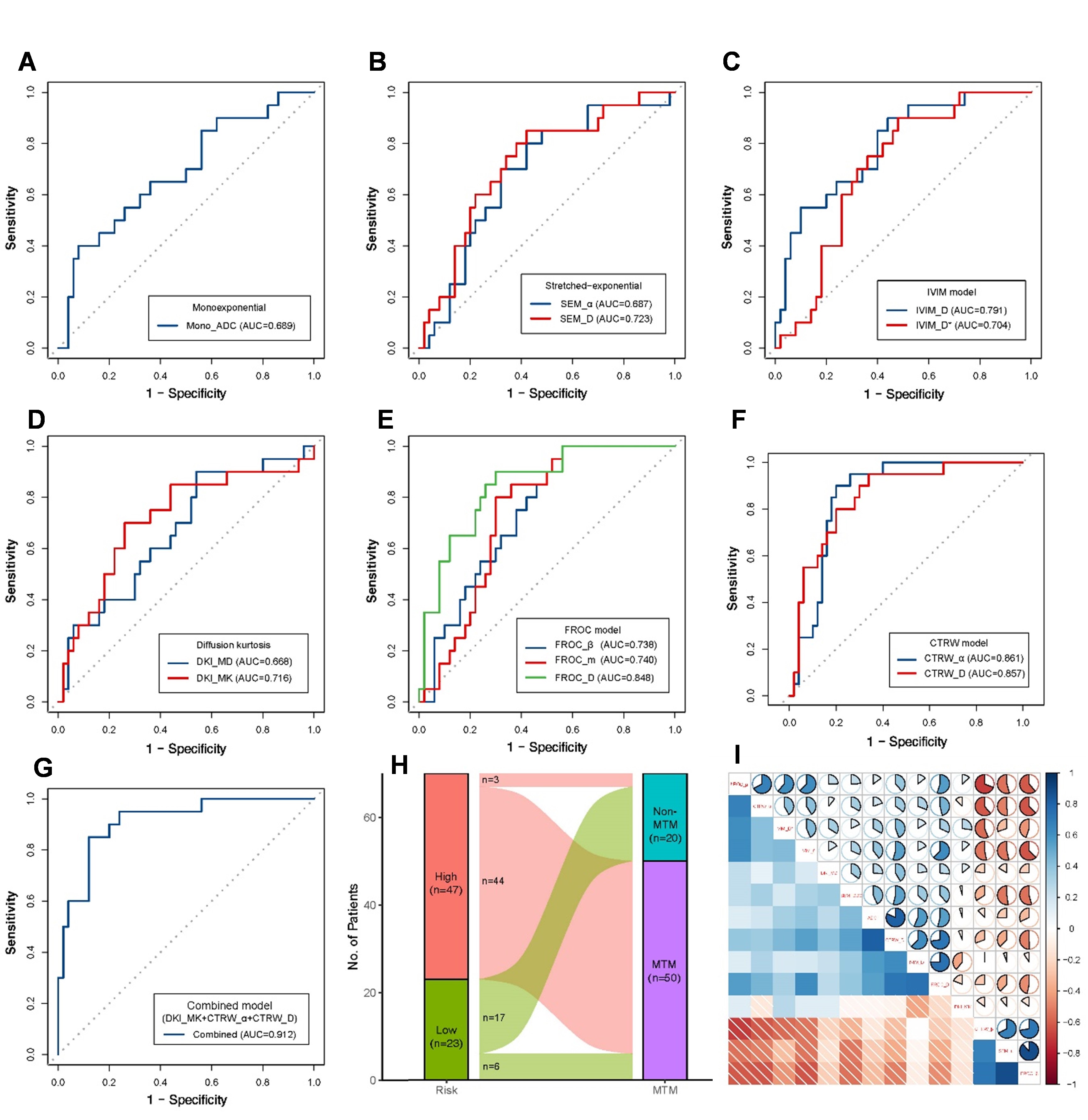
Results: CTRW_α exhibited the highest predictive performance with an AUC of 0.861 among individual parameters, a combination of parameters could improve the AUC to 0.912.
Impact: MTM is a distinct subtype of HCC and is associated with aggressive biological behavior, but it might be a suitable candidate for immunotherapy. Our result demonstrated that non-Gaussian diffusion parameters could serve as promising biomarkers for predicting MTM preoperatively.
Introduction
Macrotrabecular-massive hepatocellular carcinoma (MTM-HCC) is a novel proposed subtype of HCC in 5th edition of WHO classification [1], with an estimated prevalence ranging from 10% to 38.2% in all HCC tumors [2]. MTM HCC is characterized by its aggressive biological behavior and unfavorable prognosis, but it presents a promising opportunity for immunotherapy [3-6]. Notably, the diagnosis of MTM-HCC relies on histopathologic evaluation, limiting the ability of pretherapeutic subtype identification. Pretherapeutic characterization of the MTM subtype may facilitate the development of personalized treatment plans and improvement prognosis. Studies have shown that various imaging modalities, including US [7], CT [8], PET/CT [9], and MRI [10, 11], showed promise in predicting MTM. However, the inherent subjectivity and interobserver variation in interpreting imaging characteristics raise clinical concerns. Given the complex microstructure within HCC lesions, water diffusion motion exhibits non-gaussian behavior [12]. Advanced diffusion models [13-15], such as intravoxel incoherent motion (IVIM), stretched exponential model (SEM), diffusion kurtosis imaging (DKI), fractional-order calculus (FROC), and continuous-time random walk (CTRW), revealed diffusion heterogeneity of water molecules in non-Gaussian distribution and showed high diagnosis value for tumor detection and characterization. This study aimed to investigate the utility of advanced diffusion models using multi b-value DWI in preoperative predicting MTM subtype of HCC.Methods
Consecutive patients with pathologically confirmed HCC were prospective collected. All patients underwent MR examination on a 3T MRI system (MAGETOM Prisma, Siemens Healthineers, Germany) before hepatectomy. The MRI protocol included T1WI, T2WI with fat suppression, contrast-enhanced T1WI, and DWI with multiple b-value (01, 201, 501, 1002, 1502, 2003, 4003, 6004, 8004, 12006, 15008, 200010 s/mm2). The parametric mappings of different diffusion models were calculated via an in-house developed software BoDiLab, including (1) ADC from mono-exponential model; (2) D (true-diffusion coefficient), D* (pseudo-diffusion coefficient), and f (perfusion fraction from IVIM model; (3) α (heterogeneity index) and DDC (distributed-diffusion coefficient) from SEM; (4) MD (mean diffusivity) and MK (mean kurtosis) from DKI model; (5) β (spatial fractional-order index), μ (spatial parameter), and D (diffusion coefficient) from FROC model; (6) α (temporal diffusion heterogeneity), β (spatial diffusion heterogeneity), and Dm (anomalous diffusion coefficient) from CTRW model [13-15]. The volumes of interest (VOIs) of the whole tumor were drawn on images of b800. All statistical analyses were conducted using R software. Diffusion parameters were compared by Mann–Whitney U test. Logistic regression analyses were performed to construct the combined model for MTM prediction. The receiver operating characteristic (ROC) curve was performed to evaluate the prediction performance. Spearman’s correlation analysis was performed to explore the correlation between diffusion parameters.Results
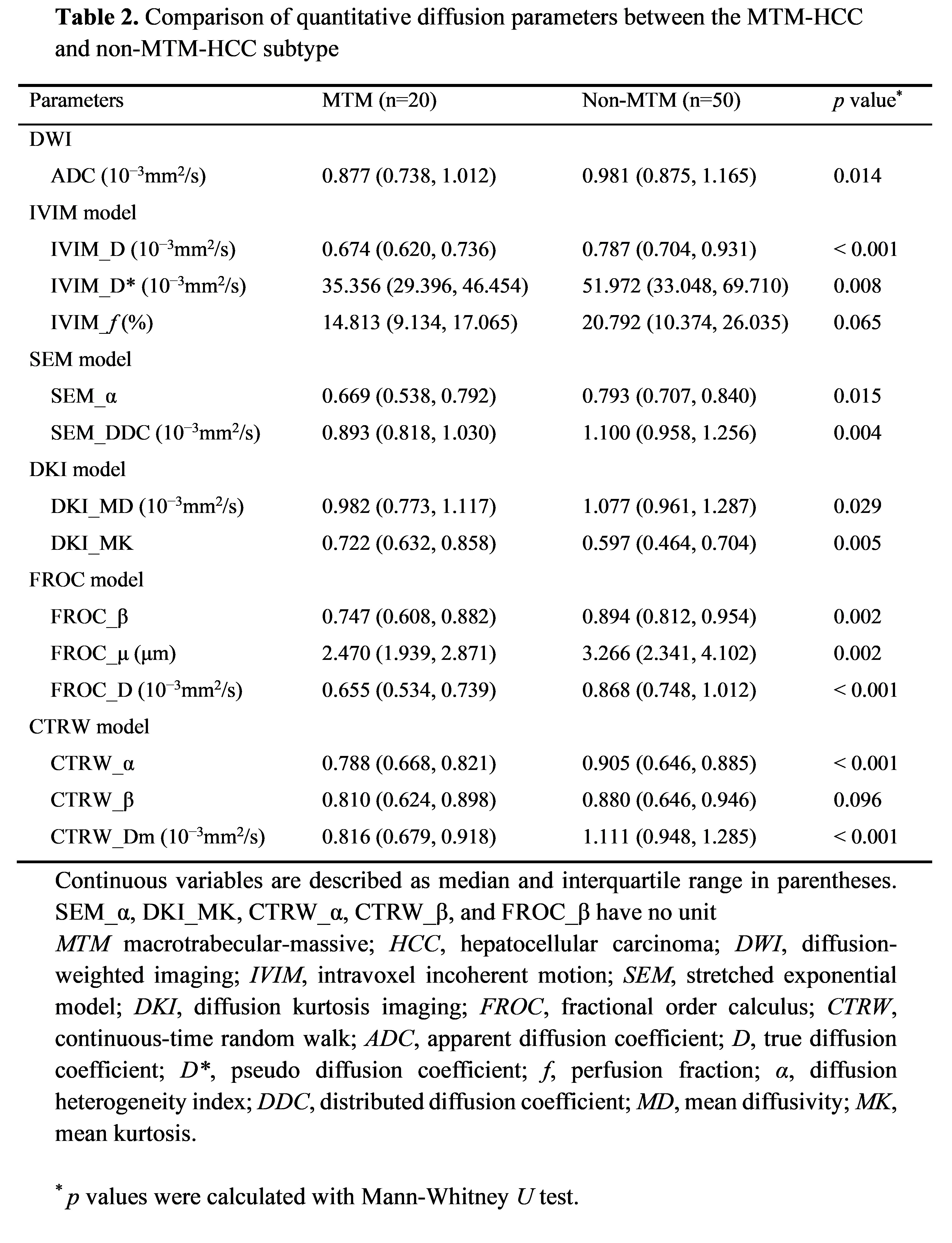
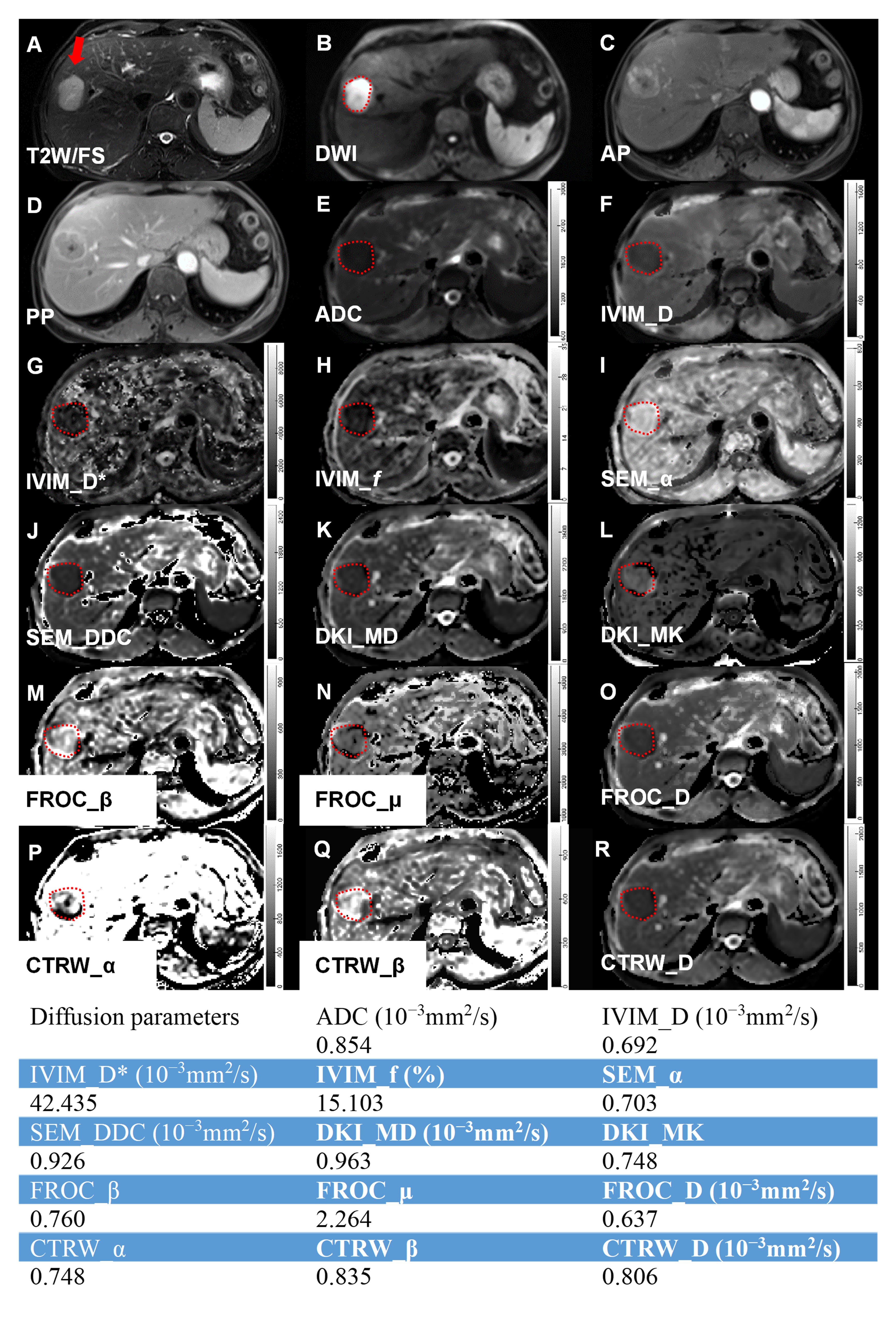
A total of 70 patients (median age 56, range 38–73; male: 51 and female: 19) were finally enrolled. 23 patients (28.6%) were MTM-HCC. The patients’ clinical data are summarized in Table 1. MTM HCC showed a higher alpha fetal protein (AFP) level (p = 0.004), tumor grade (p = 0.041), and prevalence of microvascular invasion (p = 0.034) than non-MTM subtype. The differences in the diffusion parameters between the two groups are listed in Table 2. Compared with non-MTM HCC, the ADC, IVIM_D, IVIM_D*, SEM_α, SEM_DDC, DKI_MD, FROC_β, FROC_μ, FROC_D, CTRW_α, and CTRW_Dm values in MTM HCC were significantly lower (all p<0.05), whereas the DKI_MK values were significantly higher (p<0.05). Figure 1 displays a set of images from a representative patient with MTM HCC. Table 3 and Figure 2 summarize and displayed the predictive performance of the diffusion parameters for discriminating MTM HCC from non-MTM HCC, and the correlation between parameters. CTRW_α exhibited the highest predictive performance with an AUC of 0.861, and a combination of parameters (DKI_MK, CTRW_α and CTRW_Dm) further improved the AUC to 0.912.Discussion
Due to different prognosis and possible treatment strategies, it is important to differentiate MTM HCC preoperatively. This study demonstrates the feasibility of using advanced diffusion models to predict MTM subtype HCC [12-15]. The IVIM model could separate estimation of microcirculation in the capillaries and molecular diffusion, and has been widely used in the diagnosis, treatment and prognosis of tumors. The SEM, FROC and CTRW model could reveal the distributed diffusion effect of water molecules in the tumor and identify the presence of intravoxel heterogeneity of water molecule diffusion in space and time. The decrease of diffusion-related metrics in MTM HCC might be caused by the cell proliferation, increased cell density and nucleocytoplasmic ratio. The structural complexity (e.g., intertumoral hemorrhagic necrosis) of MTM might lead to differences in heterogeneity indicators [13-15].Conclusion
Advanced diffusion model may provide noninvasive potential tool for identifying MTM subtype in HCC.Acknowledgements
None.References
[1] Nagtegaal ID, Odze RD, Klimstra D, et al; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020 Jan;76(2):182-188.
[2] Li X, Yao Q, Liu C, et al. Macrotrabecular-Massive Hepatocellular Carcinoma: What Should We Know? J Hepatocell Carcinoma. 2022 May 5;9:379-387.
[3] Ziol M, Poté N, Amaddeo G, et al. Macrotrabecular-massive hepatocellular carcinoma: A distinctive histological subtype with clinical relevance. Hepatology. 2018 Jul;68(1):103-112.
[4] Jeon Y, Benedict M, Taddei T, et al. Macrotrabecular Hepatocellular Carcinoma: An Aggressive Subtype of Hepatocellular Carcinoma. Am J Surg Pathol. 2019 Jul;43(7):943-948.
[5] Calderaro J, Couchy G, Imbeaud S, et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J Hepatol. 2017 Oct;67(4):727-738.
[6] Liu LL, Zhang SW, Chao X, et al. Coexpression of CMTM6 and PD-L1 as a predictor of poor prognosis in macrotrabecular-massive hepatocellular carcinoma. Cancer Immunol Immunother. 2021 Feb;70(2):417-429.
[7] Luo M, Liu X, Yong J, et al. Preoperative prediction of macrotrabecular-massive hepatocellular carcinoma based on B-Mode US and CEUS. Eur Radiol. 2023 Jun;33(6):4024-4033.
[8] Feng Z, Li H, Zhao H, et al. Preoperative CT for Characterization of Aggressive Macrotrabecular-Massive Subtype and Vessels That Encapsulate Tumor Clusters Pattern in Hepatocellular Carcinoma. Radiology. 2021 Jul;300(1):219-229.
[9] Hu S, Xie Y, Yang T, et al. Tumor metabolism derived from 18F-FDG PET/CT in predicting the macrotrabecular-massive subtype of hepatocellular carcinoma. Quant Imaging Med Surg. 2023 Jan 1;13(1):309-319.
[10] Mulé S, Serhal A, Pregliasco AG, et al. MRI features associated with HCC histologic subtypes: a western American and European bicenter study. Eur Radiol. 2023 Feb;33(2):1342-1352.
[11] Liang Y, Xu F, Wang Z, Tan C, Zhang N, Wei X, Jiang X, Wu H. A gadoxetic acid-enhanced MRI-based multivariable model using LI-RADS v2018 and other imaging features for preoperative prediction of macrotrabecular-massive hepatocellular carcinoma. Eur J Radiol. 2022 Aug;153:110356.
[12] Le Bihan D. Apparent diffusion coefficient and beyond: what diffusion MR imaging can tell us about tissue structure. Radiology. 2013 Aug;268(2):318-22.
[13] Guo Y, Chen J, Zhang Y, et al. Differentiating Cytokeratin 19 expression of hepatocellular carcinoma by using multi-b-value diffusion-weighted MR imaging with mono-exponential, stretched exponential, intravoxel incoherent motion, diffusion kurtosis imaging and fractional order calculus models. Eur J Radiol. 2022 May;150:110237.
[14] Liu G, Lu Y, Dai Y, et al. Comparison of mono-exponential, bi-exponential, kurtosis, and fractional-order calculus models of diffusion-weighted imaging in characterizing prostate lesions in transition zone. Abdom Radiol (NY). 2021 Jun;46(6):2740-2750.
[15] Mao C, Hu L, Jiang W, et al. Discrimination between human epidermal growth factor receptor 2 (HER2)-low-expressing and HER2-overexpressing breast cancers: a comparative study of four MRI diffusion models. Eur Radiol. 2023 Sep 6. doi: 10.1007/s00330-023-10198-x. Epub ahead of print. PMID: 37672055.
Figures