0117
High-resolution Fluid-suppressed Diffusion Tractography Shows Altered Fornix Volume and Diffusion Metrics in Pediatric Multiple Sclerosis1Biomedical Engineering, University of Alberta, Edmonton, AB, Canada, 2Pediatric Neurology, University of Alberta, Edmonton, AB, Canada, 3Radiology and Diagnostic Imaging, University of Alberta, Edmonton, AB, Canada
Synopsis
Keywords: Tractography, White Matter, microstructure, brain, adolescents, MS
Motivation: It is unknown if the fornix (main output tract of the hippocampus) is affected in pediatric multiple sclerosis (MS), which would suggest its early involvement.
Goal(s): Are the volume and diffusion metrics of the fornix affected in pediatric MS as it is in adult MS, and does fornix injury precede damage to the hippocampus?
Approach: Fornix diffusion tensor imaging and whole-brain MPRAGE were acquired from pediatric MS patients and controls. The fornix was identified with tractography.
Results: Pediatric MS showed a much (29%) smaller fornix with abnormal diffusion metrics indicative of early injury, but had no difference in hippocampus volume, compared to controls.
Impact: Diffusion tractography identifies marked injury to the fornix, a small white matter tract important for cognition, in children and adolescents with multiple sclerosis, while the hippocampus volume is unaffected, implicating the fornix as an early brain target in this disease.
Introduction
The fornix is a small white matter tract that interconnects the hippocampus and other structures of the limbic system, playing an important role in episodic memory and other cognitive functions1,2. Diffusion tensor imaging (DTI) has shown lower volume and altered diffusion metrics of the fornix in adults with multiple sclerosis (MS)3-7. The fornix is difficult to identify and measure with diffusion tractography, but it can be improved by using high-resolution fluid-attenuated inversion recovery (FLAIR) DTI which suppresses confounding cerebrospinal fluid (CSF)8. FLAIR-DTI showed marked abnormalities of the fornix in adult MS, which were greater than losses in white or gray matter volume and were most affected in those with cognitive impairment9. DTI of pediatric-onset MS (POMS) individuals scanned as children/adolescents have identified altered diffusion metrics in normal-appearing white matter10-13. Only one POMS study mentioned the fornix with elevated mean diffusivity (MD)12, but it used low spatial resolution and a voxel-based analysis not ideal for this structure14. The goal here was to use CSF-suppressed, high-resolution FLAIR-DTI tractography to determine if the fornix is affected in POMS, which would provide evidence for its early involvement.Methods
Participants were scanned on a 3T Siemens Prisma with a 64 channel head/neck RF coil and included POMS (n=5, all female, all RRMS, age=16.2±1.9 years, age range=13-19 years, EDSS=1.5±1.3, total lesion volume=11.8±9.7 cm3, time since diagnosis=2.5±1.5 years), as well as controls (n=9, all female, age=16.7±4.0 years, age range=13-19 years). The FLAIR-DTI protocol was the same as used in a previous adult MS study9: 2D single-shot EPI, 35 2 mm transverse slices centered for fornix coverage, 1.2x1.2 mm2 zero-filled to 0.6x0.6 mm2 in-plane resolution, GRAPPA R=2, phase partial Fourier 6/8, TI 2300 ms, TR 9000 ms, TE 70 ms, 5 b=0 and 20 b=1000 s/mm2, total scan time 4.2 minutes. A 0.9 mm isotropic 3D T1-weighted MPRAGE scan of the whole brain was acquired in 3.7 min. DTI processing and deterministic tractography of the fornix (FA threshold 0.15, maximum turning angle 65°, step size 0.64 mm, minimum fiber length 10 mm)9 was performed in MRtrix3. This tract yielded a whole fornix volume, as well as average fractional anisotropy (FA), MD, axial (AD) and radial diffusivity (RD) with left and right sides combined. Hippocampus volume (sum of left and right) was measured using volBrain on the 3D T1-weighted images. These metrics were compared between POMS and controls using a two-sample unpaired t-test (p<0.05).Results
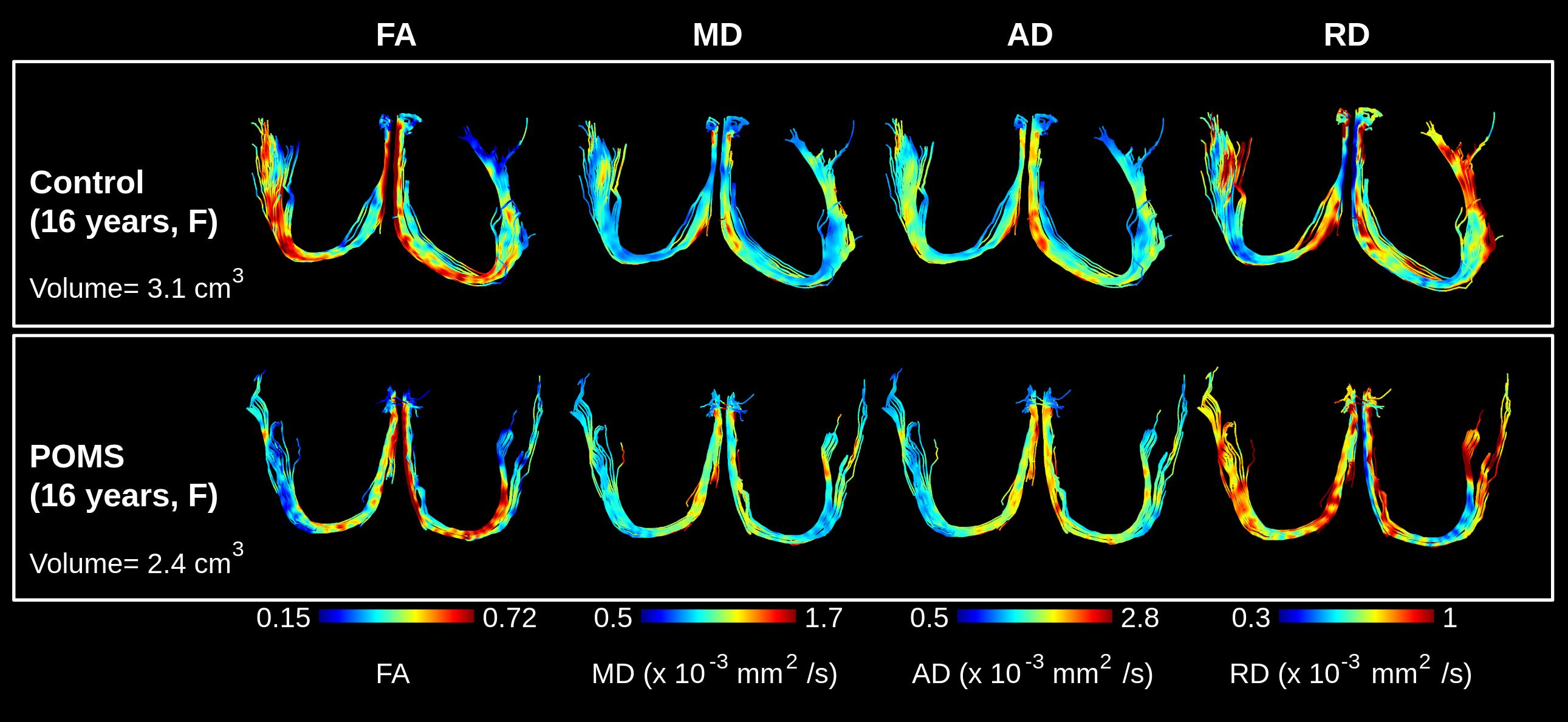
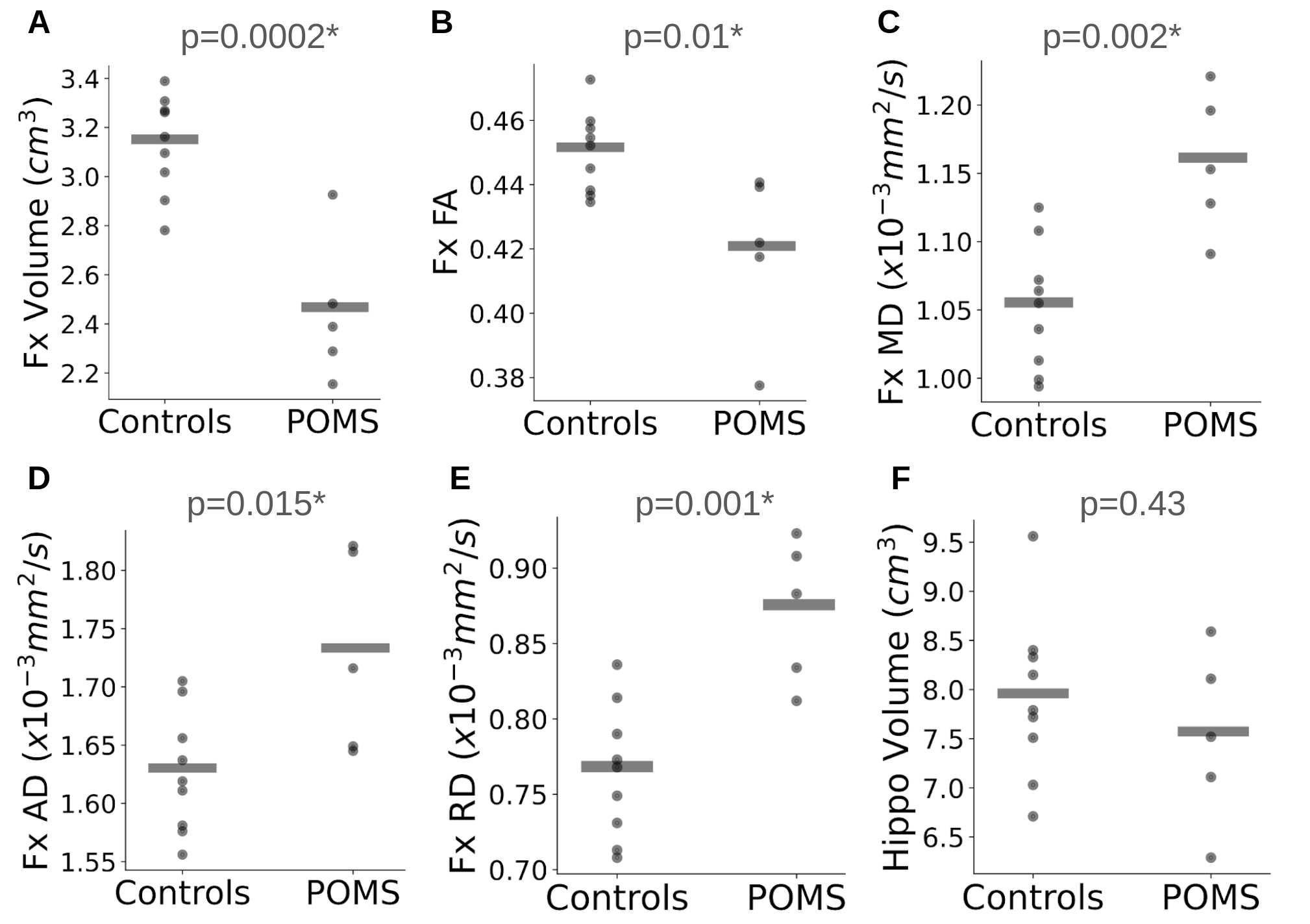
Tractography using high-resolution and CSF suppression depicted the full fornix in all 5 POMS and 9 control participants, showing visibly thinner fornix with bilateral regions of lower FA and elevated diffusivities (MD, AD, RD) along the crus and body in POMS (Figure 1). Relative to controls, the fornix in POMS had 29% lower volume (3.1±0.2 vs 2.4±0.3 cm3, p=0.0002), 7% lower FA (0.45±0.01 vs 0.42±0.03, p=0.01), 11% higher MD (1.05±0.05 vs 1.16±0.05 x10-3 mm2/s, p=0.002), 6% higher AD (1.63±0.05 vs 1.73±0.09 x10-3 mm2/s, p=0.015) and 15% higher RD (0.76±0.04 vs 0.87±0.05 x10-3 mm2/s, p=0.001) (Figure 2A-E). However, hippocampus volume was not significantly different (controls 7.9±0.8 vs POMS 7.5±0.9 cm3, p=0.43) (Figure 2F).Discussion and Conclusions
Tractography enables the virtual identification of the fornix, which can be used to output volume, something not possible in voxel-based DTI analyses. This identified that the fornix volume was markedly reduced by 29% in POMS children/adolescents, which is comparable to the 26% volume reduction in adult MS using the same high-resolution, FLAIR-DTI protocol9. Fornix DTI metrics in POMS were also similarly affected relative to controls as in the previously published adult MS study using the same protocol: FA -7% vs -7%, MD +11% vs +9%, AD +6% vs +6%, and RD +15% vs +12%9. The largest percent change in RD of the fornix is suggestive of demyelination and axonal loss15. The fornix may be especially susceptible to injury in MS as it is a small tract bathed in CSF that may contain soluble inflammatory factors16. The observation that the fornix is affected early on in POMS, but the hippocampus volume is not different between POMS and controls (similar to adult MS9) supports the hypothesis that white matter injury precedes damage to connected gray matter17. The limited sample size of 5 POMS prevented the assessment of correlations with cognitive or clinical disability. CSF-suppressed, high-resolution FLAIR-DTI has identified fornix injury as an early hallmark of MS.Acknowledgements
No acknowledgement found.References
- Senova S, Fomenko A, Gondard E, Lozano AM. Anatomy and function of the fornix in the context of its potential as a therapeutic target. J Neurol Neurosurg Psychiatry. 2020;91:547-559
- Douet V, Chang L. Fornix as an imaging marker for episodic memory deficits in healthy aging and in various neurological disorders. Front Aging Neurosci. 2014;6:343
- Fink F, Eling P, Rischkau E, Beyer N, Tomandl B, Klein J, Hildebrandt H. The association between california verbal learning test performance and fibre impairment in multiple sclerosis: evidence from diffusion tensor imaging. Mult Scler. 2010;16:332-341
- Kern KC, Gold SM, Lee B, Montag M, Horsfall J, O’Connor MF, Sicotte NL. Thalamic-hippocampal-prefrontal disruption in relapsing-remitting multiple sclerosis. Neuroimag Clin. 2015;8:440-447
- Keser Z, Hasan KM, Mwangi B, Gabr RE, Steinberg JL, Wilken J, Wolinsky JS, Nelson FM. Limbic pathway correlates of cognitive impairment in multiple sclerosis. J Neuroimaging. 2017;27:37-42
- Syc SB, Harrison DM, Saidha S, Seigo M, Calabresi PA, Reich DS. Quantitative mri demonstrates abnormality of the fornix and cingulum in multiple sclerosis. Mult Scler Int. 2013;2013:838719
- Valdes Cabrera D, Stobbe R, Smyth P, Giuliana F, Emery D, Beaulieu C. Diffusion tensor imaging tractography reveals altered fornix in all diagnostic subtypes of multiple sclerosis. Brain Behav. 2020;10:e01514
- Concha L, Gross DW, Beaulieu C. Diffusion tensor tractography of the limbic system. AJNR Am J Neuroradiol. 2005;26:2267-2274
- Valdes Cabrera D, Smyth P, Blevins G, Emery G, Beaulieu C. Diffusion imaging of fornix and interconnected limbic deep gray matter is linked to cognitive impairment in multiple sclerosis. Eur J Neurosci. 2022;55:277-294
- Vishwas MS, Healy BC, Pienaar R, Gorman MP, Grant PE, Chitnis T. Diffusion tensor analysis of pediatric multiple sclerosis and clinically isolated syndromes. AJNR Am J Neuroradiol. 2013;34:417-423
- Rocca MA, Sonkin M, Copetti M, Pagani E, Arnold DL, Narayanan S, Sled JG, Banwell B, Filippi M. Diffusion tensor magnetic resonance imaging in very early onset pediatric multiple sclerosis. Mult Scler. 2016;22:620-627
- Blaschek A, Keeser D, Muller S, Koerte IK, Schroder AS, Muller-Felber W, Heinen F, Ertl-Wagnar B. Early white matter changes in childhood multiple sclerosis: a diffusion tensor imaging study. AJNR Am J Neuroradiol. 2013;34:2015-2020
- Longoni G, Brown RA, MomayyezSiahkal P, Elliot C, Narayanan S, Bar-Or A, Marrie RA, Yeh EA, Filippi M, Banwell B, Arnold DL. White matter changes in paediatric multiple sclerosis and monophasic demyelinating disorders. Brain. 2017;140:1300-1315
- Bach M, Laun FB, Leemans A, Tax CMW, Biessels GJ, Stieltjes B, Maier-Hein, KH. Methodological considerations on tract-based spatial statistics (TBSS). NeuroImage. 2014;100:358-369
- Klawiter EC, Schmidt RE, Trinkaus K, Liang HF, Budde MD, Naismith RT, Song SK, Cross AH, Benzinger TL. Radial diffusivity predicts demyelination in ex-vivo multiple sclerosis spinal cords. NeuroImage. 2011;55:1454-1460
- Ghasemi N, Razavi S, Nikzad E. Multiple sclerosis: pathogenesis, symptoms, diagnosis and cell-based therapy. Cell J. 2017;19:1-10
- Bodini B, Chard D, Altmann DR, Tozer D, Miller DH, Thompson AJ, Wheeler-Kingshott C, Ciccarelli O. White and gray matter damage in primary progressive ms: the chicken or the egg? Neurology. 2016;86:170-176
Figures