0106
Associations between atherosclerotic luminal stenosis in the distal internal carotid artery and diffuse wall thickening in its upstream segment1Radiology, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China, 2Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Vessel Wall, Atherosclerosis
Motivation: Significant atherosclerotic stenosis or occlusion in the distal carotid artery may induce diffuse wall thickening (DWT) in the upstream arterial wall.
Goal(s): This study aimed to assess the association of atherosclerotic steno-occlusive diseases in the distal internal carotid artery (ICA) with DWT in the upstream ipsilateral ICA.
Approach: Individuals with atherosclerotic stenosis in the distal ICA, detected by carotid MR vessel wall imaging, were enrolled.
Results: Significant correlations were found between distal ICA stenosis and DWT in the petrous ICA, DWT severity, the longitudinal extent of DWT in the ICA, enhancement in the petrous ICA) and enhancement degree.
Impact: Diffuse wall thickening is a common secondary change in atherosclerotic steno-occlusive disease in the intracranial carotid. This phenomenon constitutes a confounding factor in the distinction between atherosclerosis and inflammatory vasculopathies, and could be reversed after alleviated atherosclerotic stenosis.
Introduction
We previously demonstrated diffuse wall thickening (DWT) of the petrous ICA is common in patients with atherosclerotic steno-occlusive disease in the proximal ICA [1]. In daily clinical practice, we have found a similar phenomenon of DWT in individuals with atherosclerotic steno-occlusive disease in or above the clinoid segment, defined as the distal ICA in this work. The current study aimed to verify the reliability of the presence and spread of DWT, and to investigate the association of DWT with atherosclerotic steno-occlusive diseases in the distal ICA.Methods
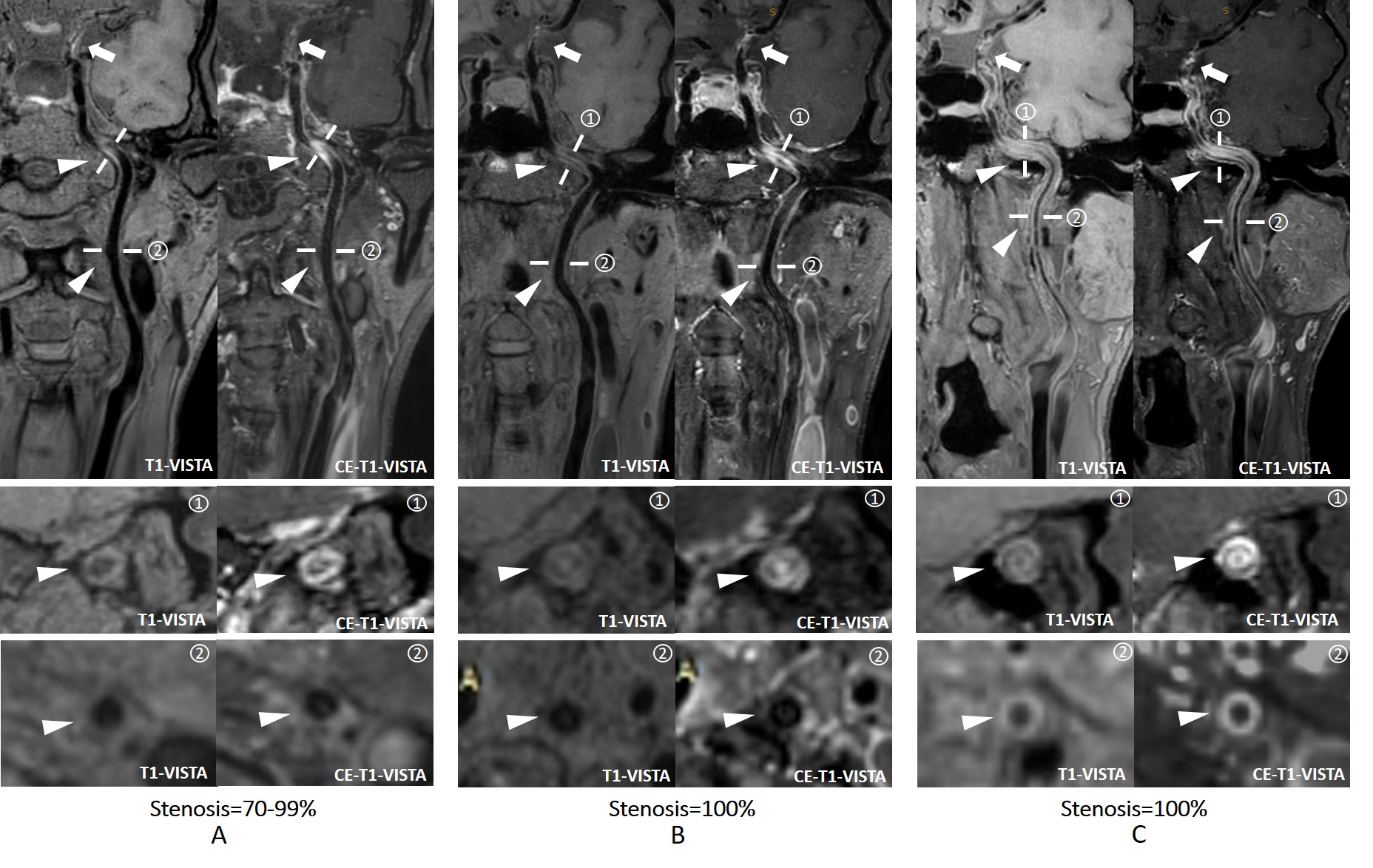
Patients with recent cerebrovascular symptoms and atherosclerotic stenosis in the distal ICA, which were detected by carotid MR imaging with T1-VISTA sequence[2-6], were retrospectively enrolled. The features of DWT in the upstream ipsilateral ICA, including longitudinal extent, wall thickness, enhancement degree, and distal ICA stenosis, were reviewed on the original T1-VISTA images. As we found that DWT does not occur only in the petrous segment, we also evaluated the longitudinal extent of DWT, which was divided into two categories: 1) focal DWT, which was limited to the petrous segment; 2) spread DWT, which went beyond the petrous segment to the cervical or lacerum segment and above.Results
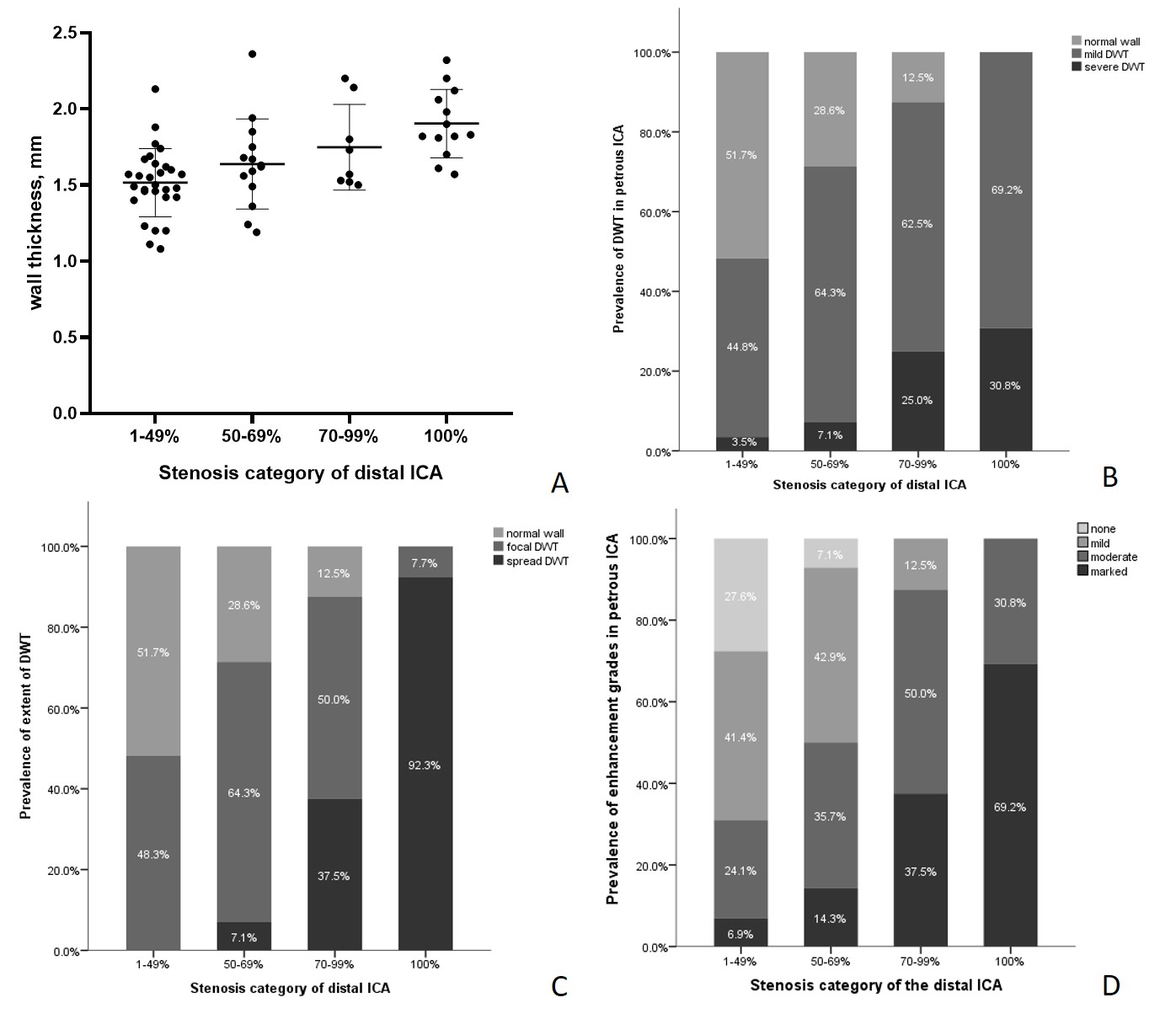
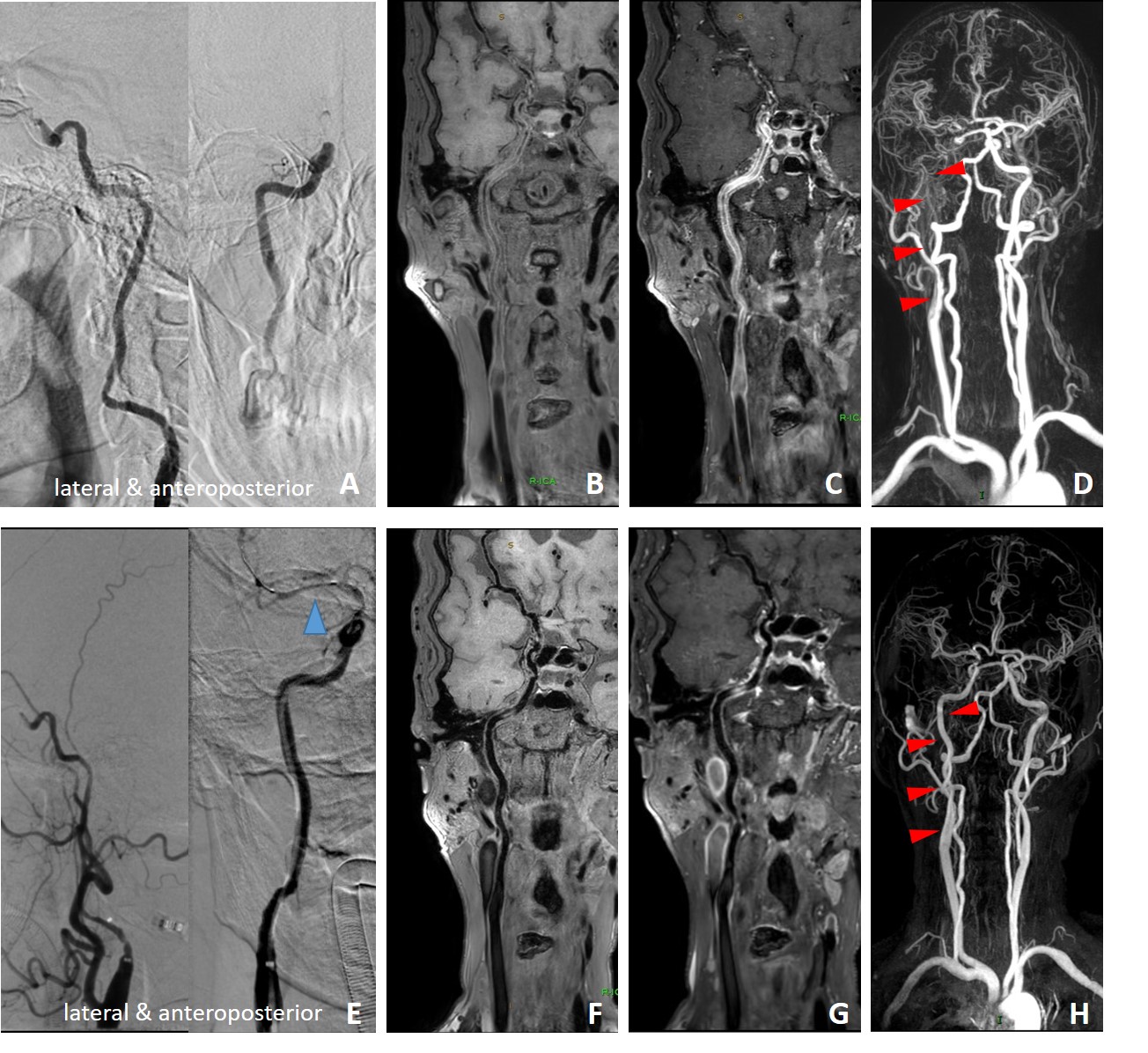
Of the 64 ipsilateral petrous ICAs, 31.3% had normal walls, 56.2% showed mild DWT, and 12.5% had severe DWT. For the longitudinal extent of DWT, there were 63.6% and 36.4% were focal and spread DWT, respectively. All cases of spread DWT involved the cervical segment, and only 25.0% involved the lacerum segment or above. The wall thicknesses of petrous ICA in the 1-49%, 50-69%, 70-99%, and 100% stenosis groups were 1.52 ± 0.22 mm, 1.64 ± 0.30 mm, 1.75 ± 0.28 mm, and 1.90 ± 0.22 mm, respectively (Figure 1A). Pearson correlation analysis showed that the grade of distal ICA stenosis was significantly correlated with the degree of wall thickness in the petrous ICA (r = 0.482, P < 0.001). In the distal ICAs with the stenosis categories of 1-49%, 50-69%, 70-99% and 100%, the respective prevalence rates of spread DWT were 0.0%, 7.1%, 37.5% and 92.3%, respectively (Figure 1C). Spearman’s correlation analysis revealed distal ICA stenosis was significantly correlated with the longitudinal extent of DWT (r = 0.671, P < 0.001). Figure 2 was the cases with longitudinal extent of DWT. DWT remission or regression was found in all three arteries underwent endovascular treatment. Figure 4 is an example case. Totally 3 months after balloon dilation plus stent implantation, spread DWT subsided significantly (Figure 3F-G) and the formerly slender ICA returned to normal (Figure 3H).Discussion
We found that the phenomenon of DWT in the petrous ICA became more common with increasing stenosis severity in the distal ICA. Additionally, the extent of DWT usually goes beyond the petrous ICA in patients with severe stenosis (≥70%) in the distal ICA, especially with distal ICA occlusion. As for atherosclerosis plaques, many studies assessing neovascularization and enhancement focused on plaques, while not too many of them paid attention to vascular beds upstream and downstream of lesions[7]. Previous findings showed that DWT of the petrous ICA is common among patients with atherosclerosis in the proximal ICA [1]. In the present study, DWT also occurred in patients with steno-occlusive atherosclerosis disease in the distal ICA, and the prevalence of 68.8% showed DWT was not a rare phenomenon. In this work, spread DWT, which showed a slender lumen accompanied by ring-like enhancement, was detected in 25.0% of patients with atherosclerotic stenosis in the distal ICA. Previously, the phenomena of ring-like enhancement and diffuse constriction of the vascular lumen have been described in Moyamoya diseases, Takayasu aortitis, vasculitis, etc., but rarely reported in carotid atherosclerosis [8; 9]. When similar imaging findings are observed, carotid atherosclerosis should also be included in the diagnostic scheme. Moreover, the slender lumen and thickened wall may increase the odds of vessel injury and false lumen generation in endovascular interventions. Preoperative diagnosis may prompt clinicians to select a more suitable guidewire, which should be applied through the edema segment more softly and carefully. In a follow-up case, we found DWT reversed after the removal of distal ICA stenosis. Although further follow-up is needed to be more conclusive, DWT does appear to differ from the pathophysiological processes of vasculitis, etc.Conclusion
Diffuse wall thickening of the petrous ICA is commonly found in patients with atherosclerotic steno-occlusive disease in the distal ICA, especially in occluded distal ICA. Stenosis degree in the distal ICA is associated with wall thickening and its longitudinal extent in upstream segments.Acknowledgements
NoneReferences
1 Chen X, Zhao H, Chen Z et al (2017) Association between proximal internal carotid artery steno-occlusive disease and diffuse wall thickening in its petrous segment: a magnetic resonance vessel wall imaging study. Neuroradiology 59:485-490
2 Zhou F, Wang M, Cao L et al (2022) Association of contrast enhancement of proximal internal carotid artery wall and champagne bottle neck sign with ipsilateral stroke in moyamoya disease patients. Eur J Radiol 155:110501
3 Chen X, Wang J, Liu Y et al (2018) Proximal internal carotid artery stenosis associates with diffuse wall thickening in petrous arterial segment of moyamoya disease patients: a three-dimensional magnetic resonance vessel wall imaging study. Neuroradiology 61:29-36
4 Luo Y, Guo Z-N, Niu P-P et al (2016) 3D T1-weighted black blood sequence at 3.0 Tesla for the diagnosis of cervical artery dissection. Stroke Vasc Neurol 1:140-146
5 Takano K, Hida K, Kuwabara Y, Yoshimitsu K (2017) Intracranial arterial wall enhancement using gadolinium-enhanced 3D black-blood T1-weighted imaging. Eur J Radiol 86:13-19
6 Park CJ, Cha J, Ahn SS et al (2020) Contrast-Enhanced High-Resolution Intracranial Vessel Wall MRI with Compressed Sensing: Comparison with Conventional T1 Volumetric Isotropic Turbo Spin Echo Acquisition Sequence. Korean J Radiol 21:1334
7 Sadat U, Jaffer FA, van Zandvoort MAMJ, Nicholls SJ, Ribatti D, Gillard JH (2014) Inflammation and Neovascularization Intertwined in Atherosclerosis. Circulation 130:786-794
8 Gaballah M, Goldfisher R, Amodio JB (2017) The Utility of MRI in the Diagnosis of Takayasu Arteritis. Case Reports in Pediatrics 2017:1-4
9 Kerut CK, Sheahan C, Sheahan M (2019) Carotid artery fibromuscular dysplasia: Ultrasound andCTimaging. Echocardiography 36:971-974
Figures