0105
Association of Dynamic Contrast Enhanced (DCE) MRI of Abdominal Aortic Aneurysm (AAA) Wall with Progression: A Prospective Study1Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 2Department of Radiation Oncology, University of California Los Angeles, Los Angeles, CA, United States, 3Department of Radiology, University of Washington, Seattle, WA, United States, 4Department of Surgery, University of California San Francisco, San Francisco, CA, United States
Synopsis
Keywords: Vascular, Cardiovascular
Motivation: Abdominal Aortic Aneurysms (AAAs) are common, and rupture has >80% mortality. The standard of care is regular surveillance and repair when maximum diameter thresholds are reached. Many ruptures occur before AAA reach these thresholds at surveillance.
Goal(s): The goal of this prospective study was to determine if AAA wall contrast kinetics using DCE MRI, presumably associated with inflammatory microvasculature, independently predict progression.
Approach: 23 AAA patients were followed over a mean follow-up interval of 14±6 months.
Results: Ktrans was significantly associated with progression after controlling for AAA maximum diameter. This suggests that DCE MRI may provide useful information regarding future AAA progression.
Impact: Contrast kinetics in AAA wall tissue assessed by DCE MRI may be useful for improving AAA risk stratification.
INTRODUCTION
AAA, a dilatation of the abdominal aorta to greater than 3cm diameter, has a pooled global prevalence of 4.8%1. AAA rupture has 80–90% mortality2. AAA maximum diameter (Dmax) remains the best-known predictor of rupture risk and is the primary factor used to time elective repair. Nonetheless, 10% of AAA rupture before reaching repair thresholds and 40% of ruptured AAAs are below repair thresholds at last surveillance3. AAA wall microvasculature has been identified as a source of inflammatory cells and matrix metalloproteinases that lead to wall strength loss and AAA progression4. Dynamic contrast enhanced (DCE) MRI, which quantifies the uptake of gadolinium-based contrast agent in tissue, has been used to study AAA wall microvasculature5. Specifically, quantitative AAA DCE MRI analyses are feasible, reproducible6 and microvascular density as assessed by both AUC and initial uptake slope is independently associated with a preceding period of faster AAA growth5. The purpose of this study was to explore the association of the DCE MRI with prospective AAA growth rate.METHODS
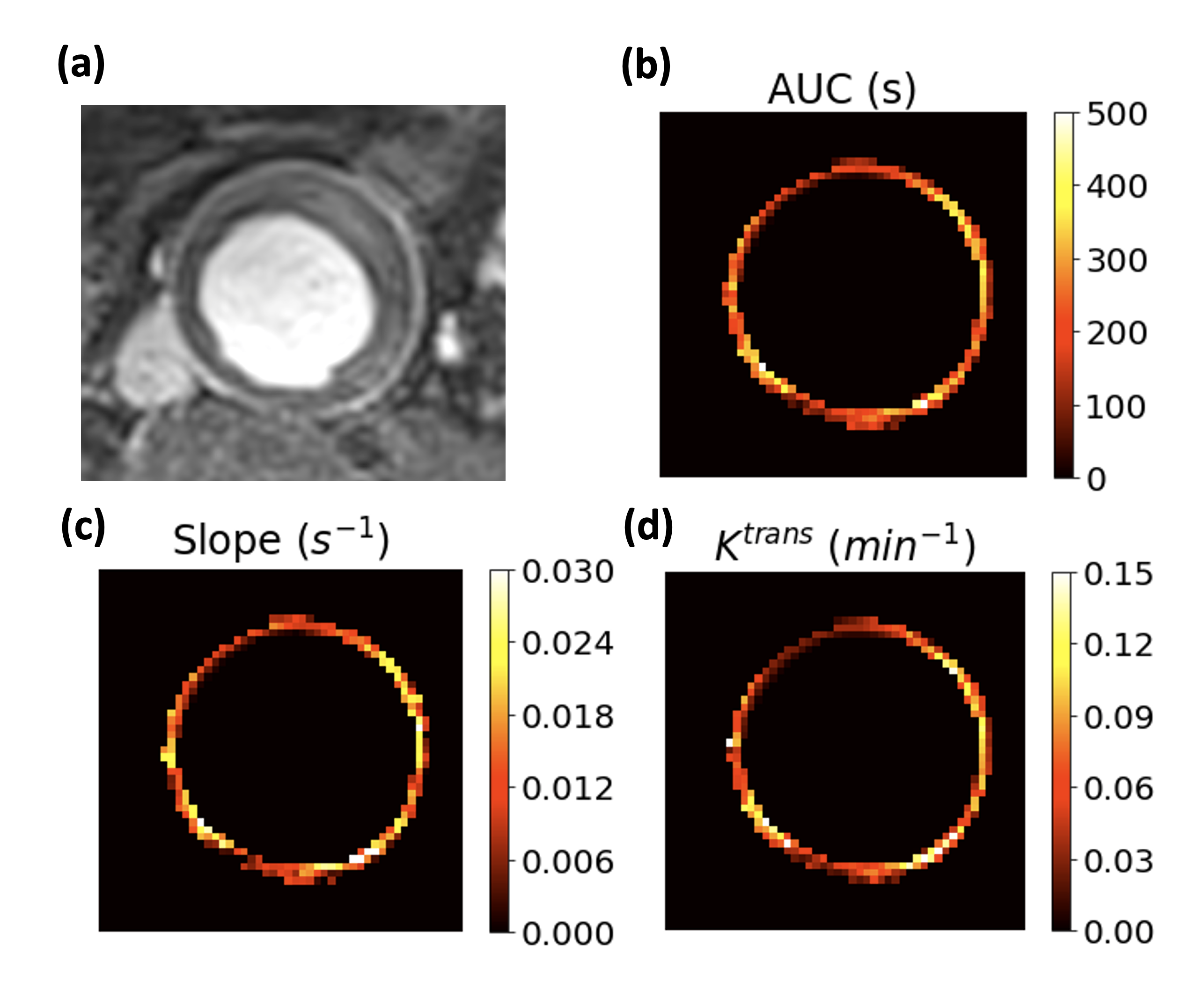
DCE MRI was acquired at 3T in 23 AAA subjects using a 3D fast gradient-echo (Star-VIBE) sequence. Sequence parameters were: 5mm slice thickness, 1.5mm in-plane resolution, 13-15s temporal resolution, and a total of 21-30 phases. Two axial slices at the level of maximum AAA diameter were selected for analysis per case. AAA wall tissue was manually isolated for analysis, from which Ktrans using the Patlak pharmacokinetic model area under the curve (AUC) at 4-min and initial 1-min slope were obtained as previously described5. For AUC and slope, the peak AAA lumen mean relative enhancement was used as a normalization factor to account for inter-subject variation of blood contrast concentration. Each DCE measurement was averaged over all voxels of the isolated AAA wall. AAA growth rate was calculated from Dmax measurements of each subject’s subsequent MRI or CT AAA surveillance exams in the 2 years following the DCE study. Dmax was measured by two independent reviewers on an axial image slice corresponding to the analyzed DCE image slices. Linear mixed effects model was used to assess the association of Dmax and aneurysm prospective growth rate (PGR) with the DCE metrics.RESULTS
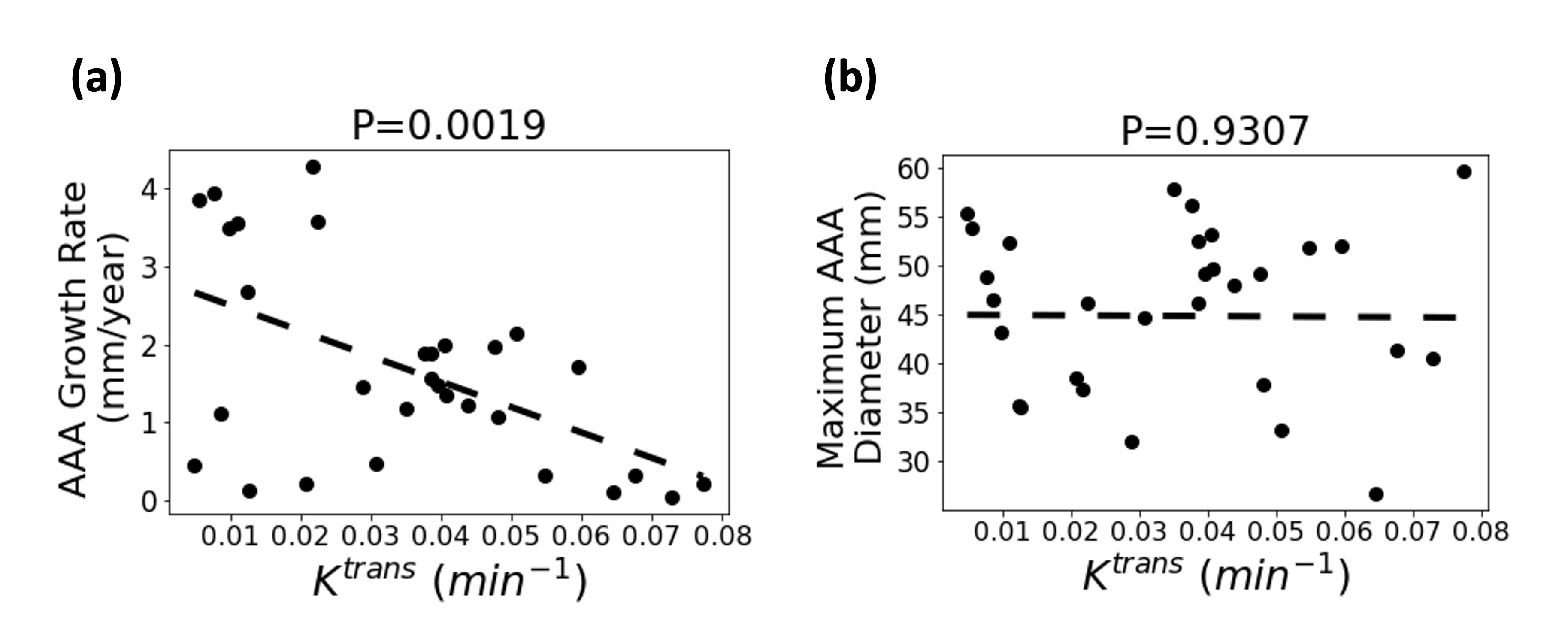
The 23 patients (all male, mean age: 75±5 years) had a total of 30 DCE studies through baseline imaging and during the follow-up period. Visually, AUC, slope and Ktrans showed significant variation over the circumference of the AAA wall (Figure 1). The average AAA maximum diameter in the 30 DCE MRI studies was 45.8±8.4 mm. Dmax was not significantly associated with any DCE measurement (PAUC=0.7544, Pslope=0.9577 and PKtrans=0.9307). The average follow-up interval following DCE imaging was 430±179 days. The average AAA growth rate observed in that interval was PGR=1.7±1.3 mm per year. A negatively significant association was only observed between Ktrans and the PGR (PAUC=0.1003, Pslope=0.091 and PKtrans=0.0014). After controlling for Dmax, Ktrans remained statistically significantly associated with PGR (PKtrans=0.0019; Figure 2a), while AUC and slope were still not significantly associated with PGR (PAUC=0.1162 and Pslope=0.1021).DISCUSSION
DCE MRI was used to associate contrast uptake dynamics in the AAA wall with future growth rate. Previous work had observed increased microvascular density, as assessed by uptake AUC and initial slope, after a period of faster AAA growth. The present study suggests that reduced contrast efflux into wall tissue may predict a faster future growth rate.CONCLUSION
Our study of contrast kinetics in AAA revealed that increased contrast efflux in AAA wall tissue as measured by Ktrans was independently associated with future AAA progression. In conjunction with previous results and histopathologic studies relating inflammatory infiltrates with AAA wall microvasculature, our results suggest a dynamic microvascular environment whose in vivo characterization may help improve AAA risk stratification.Acknowledgements
VA Merit Award. Grant Number: I01CX002071.References
1. Li, Xi, et al. "Prevalence and trends of the abdominal aortic aneurysms epidemic in general population-a meta-analysis." PloS one 8.12 (2013): e81260.
2. Bengtsson, Henrik, and David Bergqvist. "Ruptured abdominal aortic aneurysm: a population-based study." Journal of vascular surgery 18, no. 1 (1993): 74-80.
3. Ahmad, Mehtab, et al. "How quickly do asymptomatic infrarenal abdominal aortic aneurysms grow and what factors affect aneurysm growth rates? Analysis of a single centre surveillance cohort database." European Journal of Vascular and Endovascular Surgery 54.5 (2017): 597-603.
4. Reeps, Christian, et al. "Inflammatory infiltrates and neovessels are relevant sources of MMPs in abdominal aortic aneurysm wall." Pathobiology 76.5 (2009): 243-252.
5. Zhou, Ang, et al. "Dynamic Contrast‐Enhanced MRI in Abdominal Aortic Aneurysms as a Potential Marker for Disease Progression." Journal of Magnetic Resonance Imaging (2023).
6. Nguyen, V. Lai, et al. "Quantification of abdominal aortic aneurysm wall enhancement with dynamic contrast‐enhanced MRI: feasibility, reproducibility, and initial experience." Journal of Magnetic Resonance Imaging 39.6 (2014): 1449-1456.
Figures