0103
3D non-enhanced coronary MRA combined with wall imaging in the diagnosis of coronary artery stenosis1Geriatric Hospital of Nanjing Medical University, NANJING, China, 2Department of Radiology,Geriatric Hospital of Nanjing Medical University,Nanjing,, NANJING, China, 3Department of Radiology, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, CHIAN, China, 4Nanjing, ChinaPhilips Healthcare, Shanghai, SHANGHAI, China, 5Philips Healthcare, Shenyang, China., SHENYANG, China, 6Department of Radiology, Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, NANJING, China
Synopsis
Keywords: Vessel Wall, Cardiovascular, Coronary artery disease
Motivation: Advancements in coronary MR angiography (CMRA) have optimized the visualization of coronary anatomical structures, subsequently enhancing coronary artery stenosis, dilation, and certain anatomical variations【1-3】.Current meta-analysis shows that coronary MRA has a 79% accuracy rate for detecting obstructive CAD compared with gold-standard ICA
Goal(s): Thus,the combining wall imaging may potentially enhances the diagnosis performance of coronary artery stenosis
Approach: compare diagnostic performance of 3D -non enheanced CMRA with combined wall imaging
Results: Our study suggest that combining these two techniques may improve the accuracy of coronary stenosis.
Impact: CMRA has unique diagnostic in detecting coronary artery stenosis, and the improvement of diagnostic accuracywill further promote its clinical application.
Introduction
Previous studies revealed that non-enhenced CMRA has a lower sensitivity and specificity for coronary artery stenosis.The purpose of this study was to design an optimal non-contrast CMRA scan protocol combining wall imaging to evaluate its diagnostic performance for coronary artery stenosis.Methods
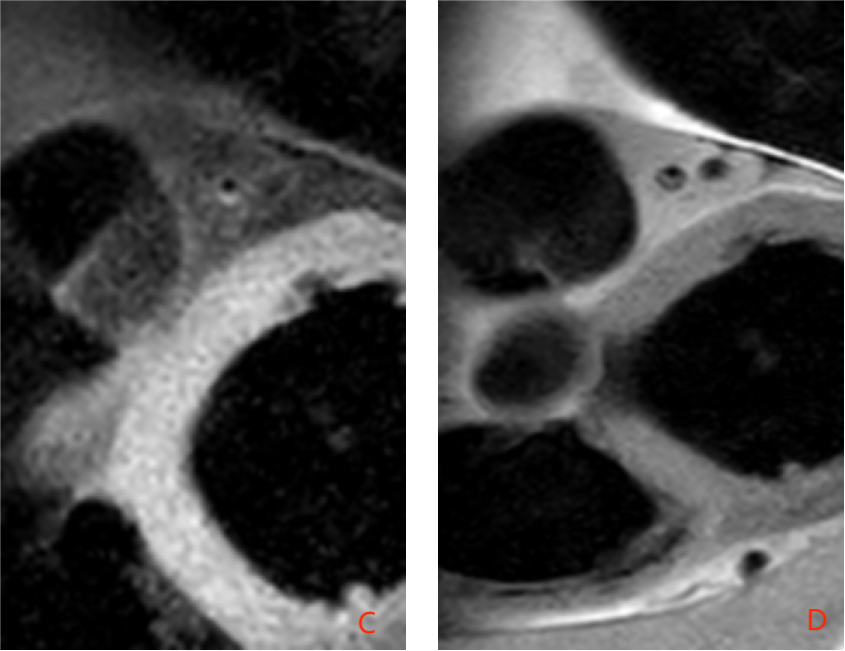
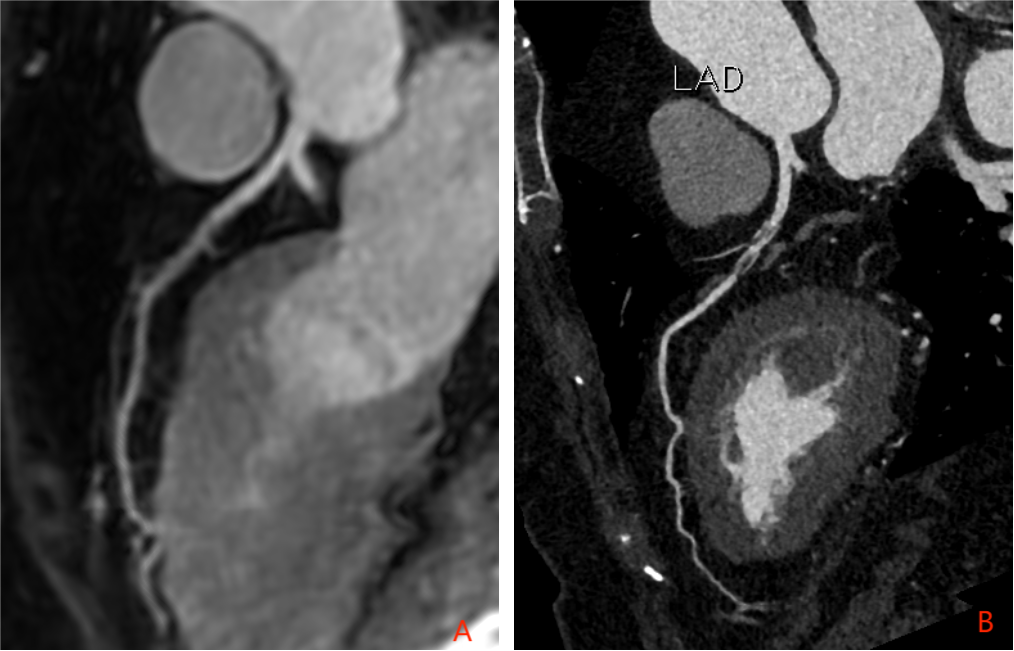
32 patients who were diagnosed with coronary stenosis in the proximal-mid segment of the left anterior descending artery (LAD)and the RCA during CTA examination were enrolled at the Jiangsu Geriatric Hospital between July 2023 and October 2023. Each patient underwent 3D non-enhanced coronary MRA, which provided comprehensive visualization of the coronary artery tree. CMRA and Wall imaging was performed on a 3T Philips scanner (Elition, Philips Healthcare, Best, the Netherlands)using a 32-channel dStream Torso phased array coil combined with an integrated flex-coverage posterior coil. .Each 2D black-blood cross-sectional image was individually prescribed based on double oblique multiplanar reformations to be orthogonal to the local longitudinal axis of the coronary wall—a double inversion recovery, ECG-triggered navigator-gated, fat-suppressed, turbo spin echo (TSE) sequence, utilizing non-coplanar excitation and REST slabs for suppressing fold-over artifacts. Imaging parameters were: TR =1 RR interval, TE = 32 ms, echo train length = 11, bandwidth = 271 Hz/pixel, matrix size = 400 x 99, field of view = 280 x 70 mm, and slice thickness = 2 mm with a gap of 2 mm.MRCA images were transferred to a three-dimensional image analysis workstation (IntelliSpace Portal; Philips Medical Systems).2D black-blood wall images were measured by VPD Software(Vp diagnostics Inc,V3.0_Build1038).To compare the diagnostic performance using two strategies:(1) by whole-heart MRCA alone and (2) by combined black-blood wall imaging. For combined MRCA analysis, only location-matched stenosis presented in both modes was determined to be positive. The diagnostic performance for significant stenosis (≥ 50% diameter reduction) was evaluated and compared using CTA as a reference standard.All statistical analyses were performed with SPSS software (version 21.0) and MedCalc software (version 18.2).Result:
CMRAs were acquired in 41 segments of 32 patients were evaluated .For CMRA alone ,23 segments were identified significant(≥ 50% diameter reduction).The stenosis were located in the LM (n = 2), proximal and middle LAD (n = 18), and RCA (n = 1).The CMRA's positive percent agreement(PPA),negative percent agreement(NPA) and overall percent agreement(OPA) for detecting significant stenosis (≥ 50% diameter reduction) are 78.9%,61.9%,and 70.7%.Out of 41 segments of 32 patients who completed coronary artery MRA wall imaging. The maximal wall thickness, wall area, lumen area, NWI in the coronary coronary stenosis more than 50% were greater compared with the coronary stenosis less than 50% ,coronary wall (2.65 ± 0.55mm versus 1.70 ± 0.39mm; 22.51±4.66 mm2versus 16.85 ± 5.26mm2; 3.05 ± 1.55 mm2 versus 6.02 ± 3.21mm2; 74.21±5.7% versus 88.47 ±4.4% respectively, P < 0.001). The difference in maximum wall thickness, wall area, lumen area, and NWI between the stenosis levels greater than 50% and less than 50% was statistically significant (P<0.001). Therefore, in this scenario, selecting wall maximum thickness≥2.03mm and NWI≥0.81 as the positive cutoff value for black blood sequences.Compared with 3D-non-enhanced MRCA, the combined wall imaging had equally high PPA for significant stenosis on a per segment (78.9 % versus 94.9%,P<0.05), while the NPA and OPA of combined CMRA were significantly elevated on a per segment(61.9% versus 81%,P<0.05;70.7%versus87.5%,P<0.05). The AUC values of combined wall imaging were significantly higher than those of CMRA on stenosis segment (P<0.05).Discussion
Our study originally evaluated the diagnostic percent agreement to detect coronary obstructions of ≥ 50% in 3.0 T non-enhenced CMRA referenced as CTA,because of combining black-blood wall imaging. The observers overestimated or underestimated stenosis in CMRA alone resulted from focal mild to moderate cardiac and motion artifacts or low lumen signal to noise ratio and low spatial resolution compared to coronary CTA【6-7】.However, the signal from static tissue is maximized and suppression of the blood signal leading to display of lumen and wall preferably that were added to the stenosis judgment.Apart from lumen depiction,wall imaging can provide plaque characterization to define the degree and nature of coronary artery disease【8】Conclusion:
Our results demonstrates that the combination of 3D non-enhanced coronary MRA and wall imaging significantly improved the accuracy of coronary artery stenosis diagnosis compared to conventional MRA.Summary of main finding
In conclusion, the integration of 3D non-enhanced coronary angiography and wall imaging represents a promising tool for improving the diagnosis of coronary artery stenosis. Its enhanced accuracy makes it a valuable addition to the clinical decision. Further research is warranted to validate these findings in larger patient cohorts and assess long-term clinical outcomes.Acknowledgements
No acknowledgement found.References
1.Fayad ZA, Fuster V, Fallon JT, Jayasundera T, Worthley SG, Helft G, Aguinaldo JG, Badimon JJ, Sharma SK: Noninvasive in vivo human coronary artery lumen and wall imaging using black-blood magnetic resonance imaging. Circulation 2000, 102:506-5102.Fernandes JL, Serrano CV Jr, Blotta MH, Coelho OR, Nicolau JC, Avila LF, Rochitte CE, Parga Filho JR: Regression of coronary artery outward remodeling in patients with non-ST-segment acute coronary syndromes: a longitudinal study using noninvasive magnetic resonance imaging. Am Heart J 2006, 152:1123-11323.McConnell MV, Meyer CH, Putz EJ, Nishimura DG, Hu BS: Spiral coronary wall imaging: Patient studies. Ninth annual meeting of the International Society for Magnetic Resonance in Medicine; Glasgow, Scotland 2001, 1969.4.Kim WY, Stuber M, Bornert P, Kissinger KV, Manning WJ, Botnar RM: Threedimensional black-blood cardiac magnetic resonance coronary vessel wall imaging detects positive arterial remodeling in patients with nonsignificant coronary artery disease. Circulation 2002, 106:296-299 5.Botnar RM, Stuber M, Kim WY, Danias PG, Manning WJ: Magnetic resonance coronary lumen and vessel wall imaging. Rays 2001, 26:291-303.6.Botnar RM, Stuber M, Kissinger KV, Kim WY, Spuentrup E, Manning WJ: Noninvasive coronary vessel wall and plaque imaging with magnetic resonance imaging. Circulation 2000, 102:2582-2587.7.Liu X, Zhao X, Huang J, Francois CJ, Tuite D, Bi X, Li D, Carr JC: Comparison of 3 D free-breathing coronary MR angiography and 64-MDCT angiography for detection of coronary stenosis in patients with high calcium scores. AJR Am J Roentgenol 2007, 189:1326-1332.8.Mézquita AJV, Biavati F, Falk V, Alkadhi H, Hajhosseiny R, Maurovich-Horvat P, Manka R, Kozerke S, Stuber M, Derlin T, Channon KM, Išgum I, Coenen A, Foellmer B, Dey D, Volleberg RHJA, Meinel FG, Dweck MR, Piek JJ, van de Hoef T, Landmesser U, Guagliumi G, Giannopoulos AA, Botnar RM, Khamis R, Williams MC, Newby DE, Dewey M. Clinical quantitative coronary artery stenosis and coronary atherosclerosis imaging: a Consensus Statement from the Quantitative Cardiovascular Imaging Study Group. Nat Rev Cardiol. 2023 Jun 5. doi: 10.1038/s41569-023-00880-4. Epub ahead of print. PMID: 37277608.Figures