0102
Coronary Artery Wall Contrast Enhancement Imaging Impact on Disease Activity Assessment in IgG4-RD a direct marker of coronary involvement1Department of Radiology, The First Hospital of China Medical University, Shenyang, China
Synopsis
Keywords: Vessel Wall, Cardiovascular, IgG4-related cardiovascular disease, cardiac magnetic resonance, coronary wall contrast enhancement, IgG4-RD responder index
Motivation: The coronary wall involvement in IgG4-related disease (IgG4-RD) is overlooked in conventional imaging, more sensitive approach is needed.
Goal(s): To investigate the feasibility of quantifying contrast enhancement (CE) to detect coronary involvement in IgG4-RD and the influence on disease activity assessment based on the IgG4-RD Responder Index (RI).
Approach: The coronary artery wall images of the IgG4-RD, systemic lupus erythematosus (SLE) patients and healthy subjects were analyzed and IgG4-RD-RI scores were collected for correlations analysis.
Results: Coronary artery wall CE can be a direct marker of coronary artery injury and may improve disease activity assessment in IgG4-RD.
Impact: Coronary artery wall CE can serve as an objective indicator of disease activity. Considering coronary artery wall CE in the IgG4-RD-RI scoring has the potential to enhance the comprehensiveness of disease activity assessment and enable more appropriate treatment decisions.
Introduction
Coronary arteries are the second most commonly affected extra-aortal arteries in IgG4-related disease (IgG4-RD) with periarteritis. 1 It is crucial to identify coronary wall remodeling in the early stages to prevent adverse events. Due to the lack of significant clinical symptoms and specific laboratory markers, early detection of coronary involvement in patients with IgG4-RD is challenging and relies heavily on imaging evidence. Previous studies have demonstrated the feasibility of coronary artery wall contrast enhancement (CE) using cardiac magnetic resonance (CMR) to detect coronary vasculitis in systemic lupus erythematosus (SLE). 2 Nevertheless, it remains uncertain whether the introduction of delayed imaging is feasible for detecting early subclinical coronary vessel wall involvement in patients with IgG4-RD.Changes in the IgG4-RD-Responder Index (RI) scores reflect disease exacerbation or improvement, indicating the requirement for increased or decreased treatment, respectively. 3 However, there are currently no studies specifically investigating the use of the RI to evaluate cardiovascular involvement. It remains uncertain as to whether the introduction of coronary wall imaging would influence the interpretation of disease activity based on the IgG4-RD RI.
Method
A total of 93 subjects (IgG4-RD = 31; SLE = 29; control = 33) without history of coronary artery disease (CAD) were prospectively recruited in the study. (Table1) All patients underwent CMR imaging using a 3.0T MR scanner (Siemens Healthcare, Erlangen, Germany).(Table2) The Coronary Atherosclerosis T1-Weighted Characterization with Integrated Anatomical Reference (CATCH) sequence was employed to obtain both dark-blood and bright-blood coronary images. 4 CATCH sequence was executed with the following parameters: 3-dimensional transverse slab covering the entire heart with field-of-view = 322 ×242 ×108mm3; matrix size = 248 ×188 ×84; acquired spatial resolution = 1.3 × 1.3 × 1.3 mm3 (interpolated to 0.7 × 0.7 × 1.3 mm3); flip angle = 12°; repetition time/echo time = 4.6/2.3 ms; the optimal inversion time interval typically ranging from 100 ms to 300 ms , applied every other heartbeat; bandwidth = 721 Hz/pixel. 4 Coronary wall total CE area and contrast-to-noise ratio (CNR) were obtained after post-processed using CVI42 software(Version 5.6.3, Circle Cardiovascular Imaging, Calgary, Canada).(Figure1) Comparison of CMR coronary wall imaging results in three groups were performed using 1-way analysis of variance (ANOVA), Kruskal-Wallis or chi-squared test with Bonferroni post-hoc and Fisher exact tests, as appropriate for the type of the data. A paired t-test was conducted to assess the differences between the updated RI scores (RI´) with consideration of coronary wall CE and the prior RI scores without. Associations between coronary wall CE and RI scores were explored by simple linear analyses. Cut-off values for the discrimination between health and disease were derived using receiver-operating characteristic curve analysis using the point that maximized the trade-off between specificity and sensitivity. All tests were two-tailed, and P<0.05 was deemed significant.Result
Both CE quantification measures have good diagnostic efficiency to discriminate between control subjects and (all) patients (total CE area: sensitivity 85%, specificity 85%, area under the curve: 0.87, odds ratio = 3.65, p < 0.001; CNR: sensitivity 68%, specificity 91%, area under the curve: 0.86, odds ratio = 2.14, p < 0.001). Coronary wall CE was observed in 29 (94%) IgG4-RD patients and 22 (76%) SLE patients with a predominately diffuse pattern. (Figure2) CNR and total CE area were significantly higher in patient groups compared to controls (P < 0.001). In the IgG4-RD group, CNR and total CE area were correlated with the RI (CNR: r = 0.60, P < 0.001; total CE area: r = 0.39, P = 0.031). RI´ scored considering coronary involvement by CE, differed significantly from RI scored without consideration of CE (P < 0.001). (Figure3)Discussion
CE of coronary artery wall on MR images, as a novel non-invasive and radiation-free imaging marker, helps to discern quiescent lesions in the coronary artery. Our data suggest that visualization and quantification of coronary CE may provide a potential new marker of IgG4-RD coronary wall remodeling and offer a new tool for more accurate assessment of disease activity. The possibility of adding CMR coronary artery wall CE to IgG4-RI is worthy of future exploration.Conclusion
CNR and the total CE area could be utilized to detect subclinical and clinical coronary wall involvement, which is prevalent in IgG4-RD and contributes to the IgG4-RD RI. The potential inclusion of coronary artery wall CE in the assessment of disease activity in IgG4-RD is worthy of further investigation.Acknowledgements
None.References
1. Peng L, Zhang P, Li J, Liu Z, Lu H, Zhu L et al. IgG4-related aortitis/periaortitis and periarteritis: a distinct spectrum of IgG4-related disease. Arthritis Res Ther. 2020 May 4;22(1):103.
2. Varma N, Hinojar R, D'Cruz D, Arroyo Ucar E, Indermuehle A, Peel S et al. Coronary vessel wall contrast enhancement imaging as a potential direct marker of coronary involvement: integration of findings from CAD and SLE patients. JACC Cardiovasc Imaging. 2014 Aug;7(8):762-70.
3. Wallace ZS, Khosroshahi A, Carruthers MD, Perugino CA, Choi H, Campochiaro C et al. An International Multispecialty Validation Study of the IgG4-Related Disease Responder Index. Arthritis Care Res (Hoboken). 2018 Nov;70(11):1671-1678.
4. Xie Y, Kim YJ, Pang J, Kim JS, Yang Q, Wei J et al. Coronary Atherosclerosis T1-Weighed Characterization With Integrated Anatomical Reference: Comparison With High-Risk Plaque Features Detected by Invasive Coronary Imaging. JACC Cardiovasc Imaging. 2017 Jun;10(6):637-648.
Figures
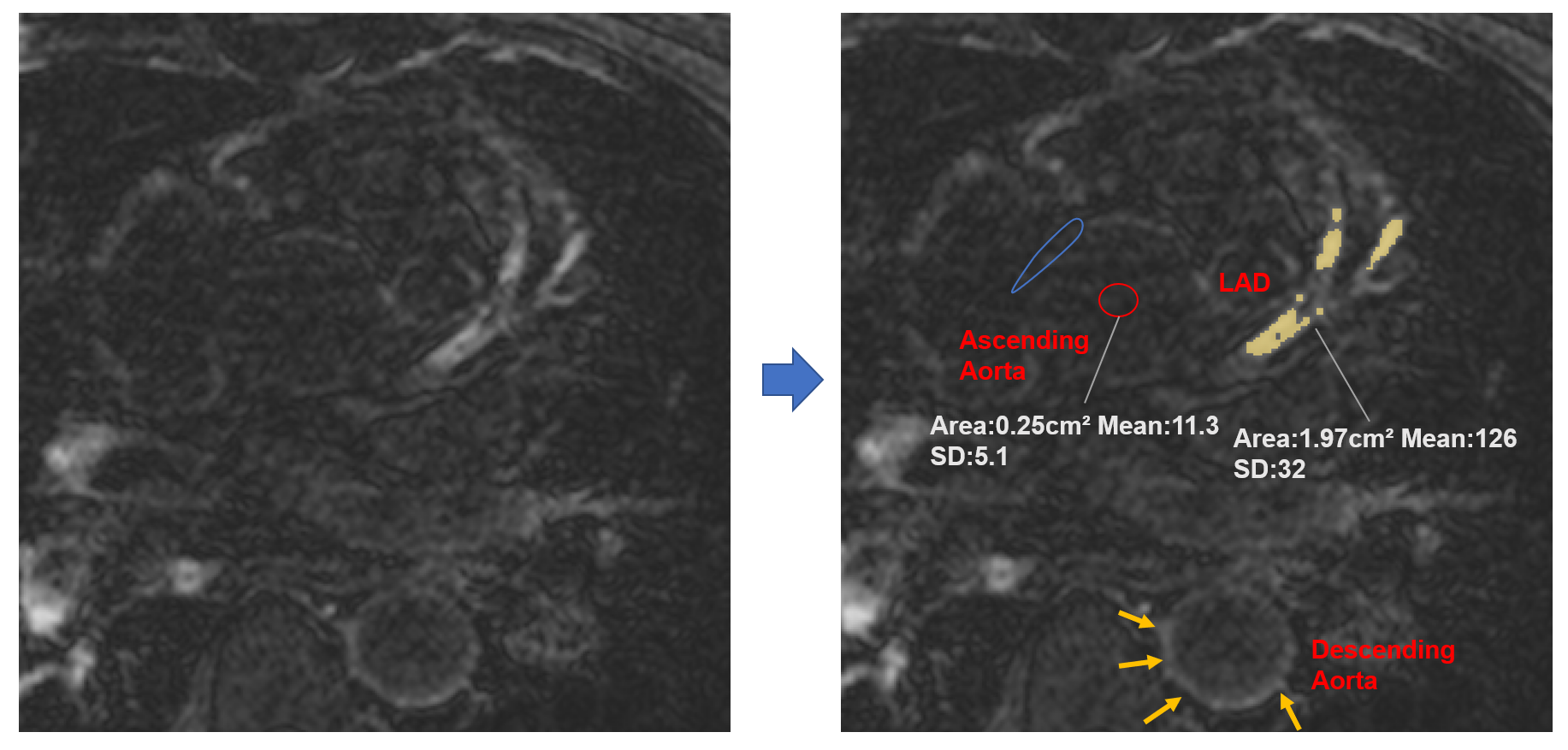
Figure 1. Quantification of Coronary CE
Contrast enhancement (CE) in the left anterior descending (LAD) coronary artery wall (yellow area): signal intensities (SIs) >2 SDs of the non-enhancing aortic wall (blue circle).
Contrast to noise ratio (CNR): based on measuring SIs of the LAD vessel wall and blood pool (red circle).
Quantitative parameter values at this slice: Total CE area=1.97cm². CNR=(SIwall-SIblood)/ mean SD noise=6.2
Yellow arrows indicate the thickened and enhanced descending aorta wall.
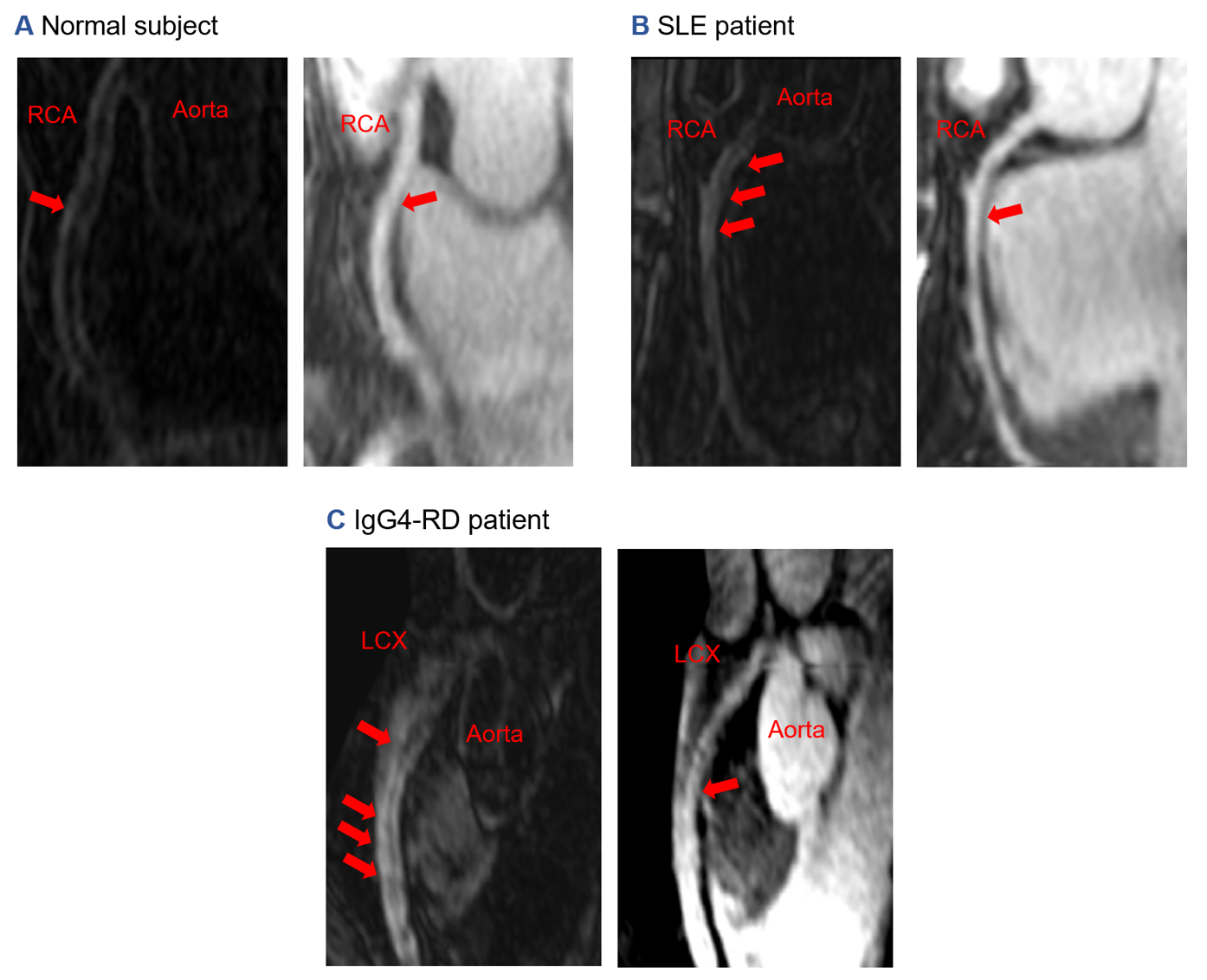
Figure 2. Representative coronary images in normal control subject, systemic lupus erythematosus (SLE) patient and IgG4-related disease (IgG4-RD) patient.
Coronary CE (contrast enhancement) and wall thickening were observed in both IgG4-RD (C) and SLE patient (B) with a diffuse pattern without luminal stenosis while control subject manifested as mild patchy coronary CE (A).
RCA: Right coronary artery; LCX: left circumflex artery
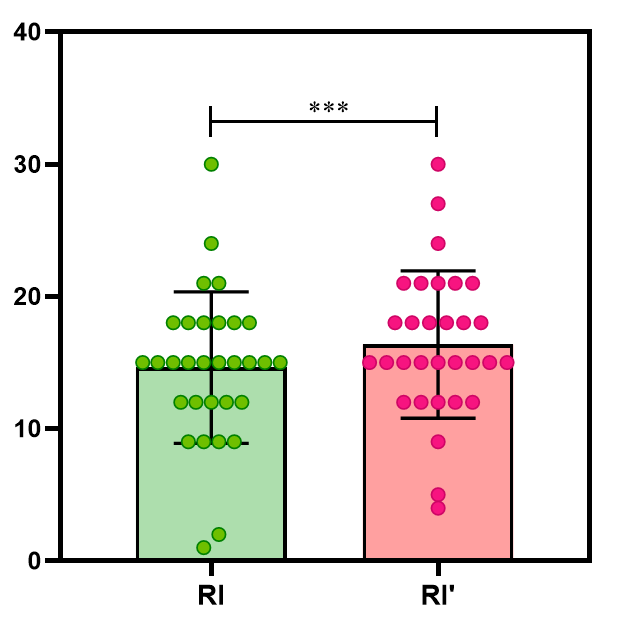
Figure 3. Paired t-test between the updated response index (RI) scores with consideration of coronary wall contrast enhancement (CE) (RI’) and the prior RI
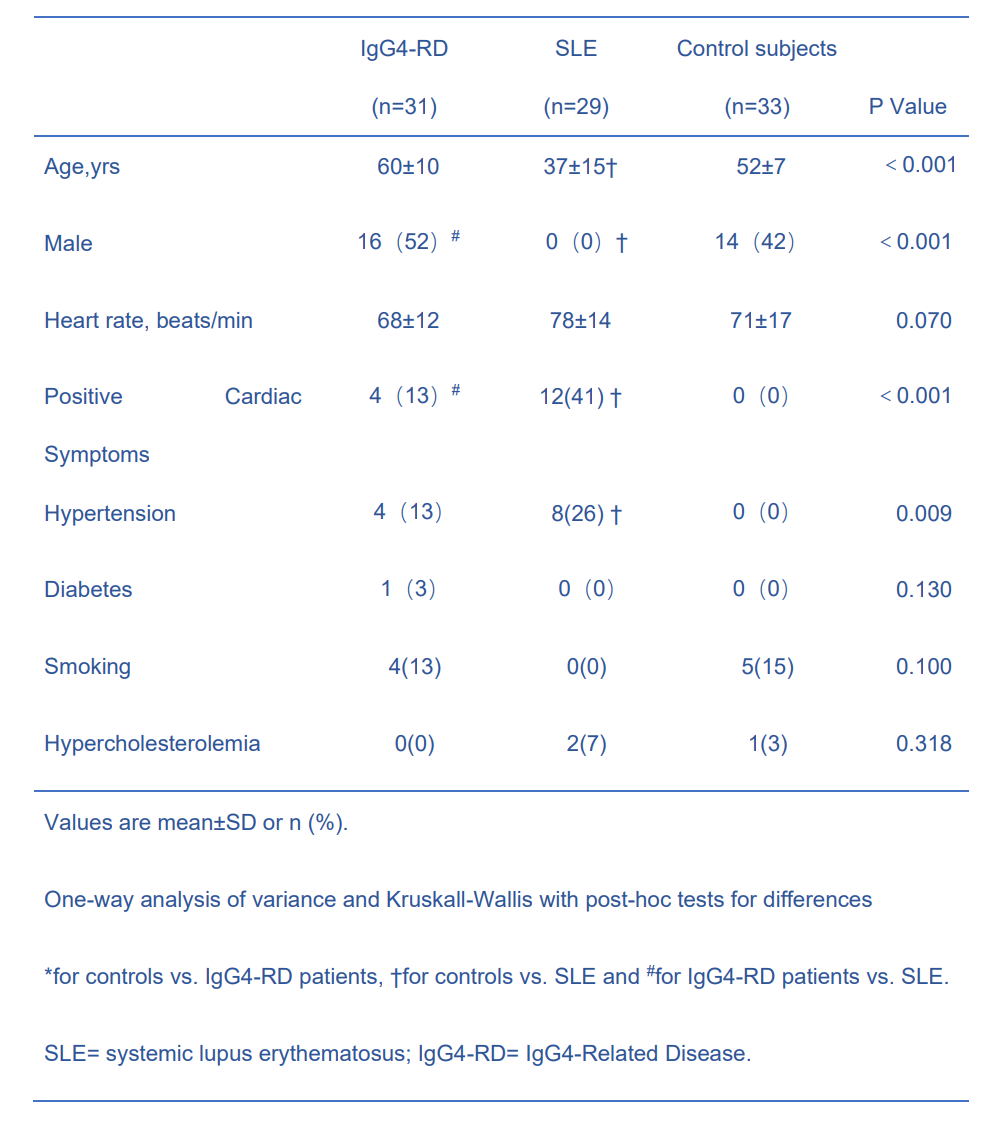
Table1. Patient Characteristics
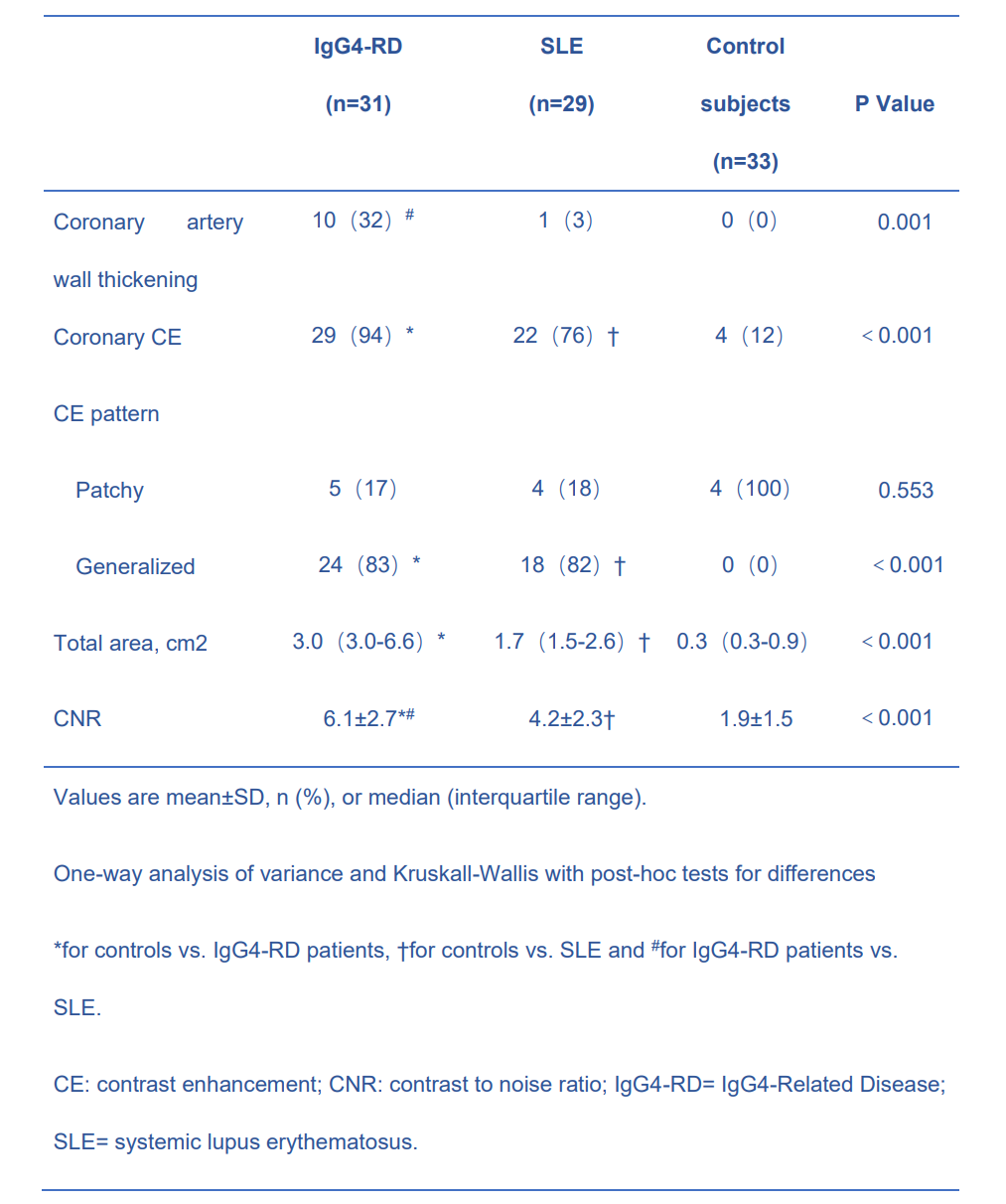
Table2. Coronary wall CE characteristics by Cardiac Magnetic Resonance