0101
Chronic Obstructive Pulmonary Disease is Associated with Impaired Cardiac Hemodynamics: A SPIROMICS HF Study1Department of Radiology, Northwestern University, Chicago, IL, United States, 2Department of Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 3Department of Radiology, Columbia University Medical Center, New York, NY, United States, 4Department of Pediatrics, Columbia University Medical Center, New York, NY, United States, 5Department of Radiology, University of Wisconsin-Madison, Madison, WI, United States, 6Columbia University Medical Center, New York, NY, United States, 7Department of Radiology, Johns Hopkins University, Baltimore, MD, United States, 8Department of Radiology, University of Michigan School of Medicine, Ann Arbor, MI, United States, 9University of Alabama at Birmingham Heersink School of Medicine, Birmingham, AL, United States, 10Department of Radiology, University of California Los Angeles, Los Angeles, CA, United States, 11Departments of Medicine and Physiology, University of California Los Angeles, Los Angeles, CA, United States, 12Department of Radiology, University of California San Francisco, San Francisco, CA, United States, 13Department of Radiology, University of Utah School of Medicine, Salt Lake City, UT, United States, 14Department of Cardiology, Wake Forest University, Winston-Salem, NC, United States, 15Department of Medicine, Columbia University Medical Center, New York, NY, United States
Synopsis
Keywords: Flow, Velocity & Flow, COPD, Lung, hemodynamics
Motivation: Previous studies have suggested impaired cardiovascular function in patients with chronic obstructive pulmonary disease (COPD). However, the association between lung disease severity and the degree of cardiac hemodynamic impairment is not well understood.
Goal(s): We aimed to characterize the hemodynamic changes seen in COPD in order to gain insight into the mechanisms relating COPD and heart failure.
Approach: We analyzed 4D-flow derived hemodynamics in a preliminary sample of 72 participants from the SPIROMICS-HF study.
Results: We found that impaired hemodynamics in the right atrium (blood flow kinetic energy and velocity) and pulmonary artery (flow stasis and velocity) are associated with greater COPD severity.
Impact: This study represents a key step in exploring the cardiopulmonary hemodynamic interaction in chronic obstructive pulmonary disease.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) prevalence and mortality have been increasing over the past decades. Morbidity and mortality from heart failure with preserved ejection fraction have risen in parallel1. Studies have found impaired left ventricular filling in COPD and emphysema2. In addition, pulmonary vascular changes have been linked to the impaired filling suggesting an upstream mechanism affecting cardiac function3,4. Thus, studying the hemodynamic consequences that COPD dictates on cardiac chambers and venous return is crucial to understanding the relationship between COPD and heart failure.4D-flow (3D + time) MRI is a reliable and reproducible imaging technique that allows a time-resolved comprehensive assessment of heart and vessels’ hemodynamics5,6. Previous assessments in the Multi-Ethnic Study of Atherosclerosis (MESA) COPD study have demonstrated the reliability and internal consistency of 4D-flow MRI in COPD7. The ability to, retrospectively and adequately, assess simultaneous 4D-flow derived pulmonary and cardiac flow may enable deeper understanding of cardiopulmonary interactions in COPD. The aim of this study is to characterize the association of physiologic metrics and COPD severity with important right heart hemodynamic parameters (blood flow velocity, stasis, viscous energy loss (VEL), and kinetic energy) in the right atrium (RA), right ventricle (RV), and main pulmonary artery (MPA).
Methods
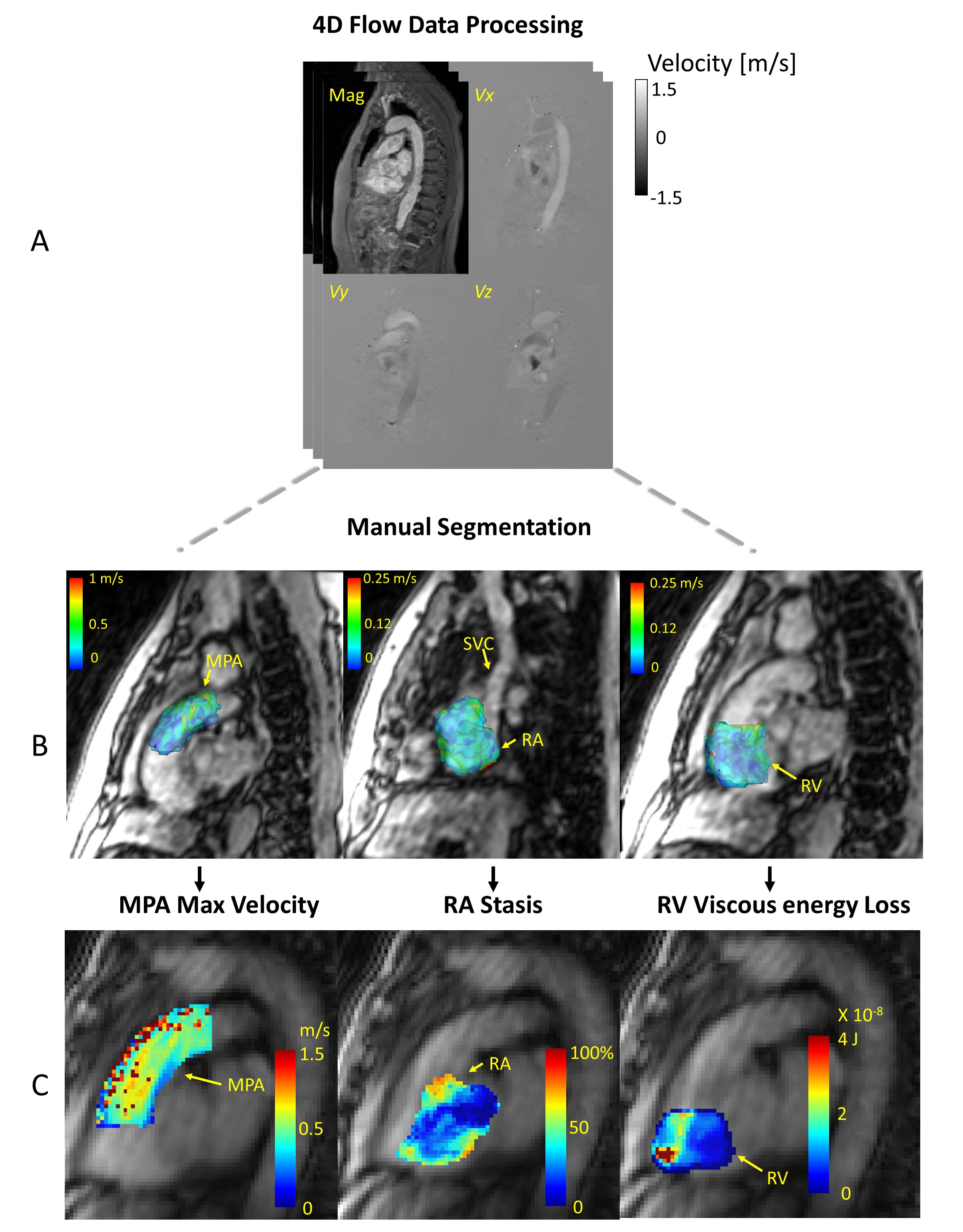
SPIROMICS is a multicenter, longitudinal case-control study that recruited COPD cases with 20+packyears of smoking and controls. SPIROMICS-HF is adding detailed cardiac phenotyping including lung CTs and cardiac MRIs in up to 700 participants. The MRI protocol includes 4D-flow MRI following a standardized protocol and central reading centers. All 4D-flow data were processed for background phase correction, noise masking and velocity anti-aliasing using a previously described algorithm8-10 (Figure 1A). A phase-contrast MR angiogram (MRA) was calculated from the flow and magnitude data and used to manually segment the RA, RV, and MPA using a dedicated software (Mimics, Materialize, Belgium). The segmentations were used for the calculation of mean and maximum velocity, blood stasis, VEL and kinetic energy (Figure 1C). COPD severity was defined by Global Initiative for Obstructive Lung Disease (GOLD) criteria. Percent emphysema, functional small airway disease, total lung capacity, and residual volume were assessed on lung CTs at a central reading center. Crude and adjusted associations between MRI and CT measures were assessed.Results
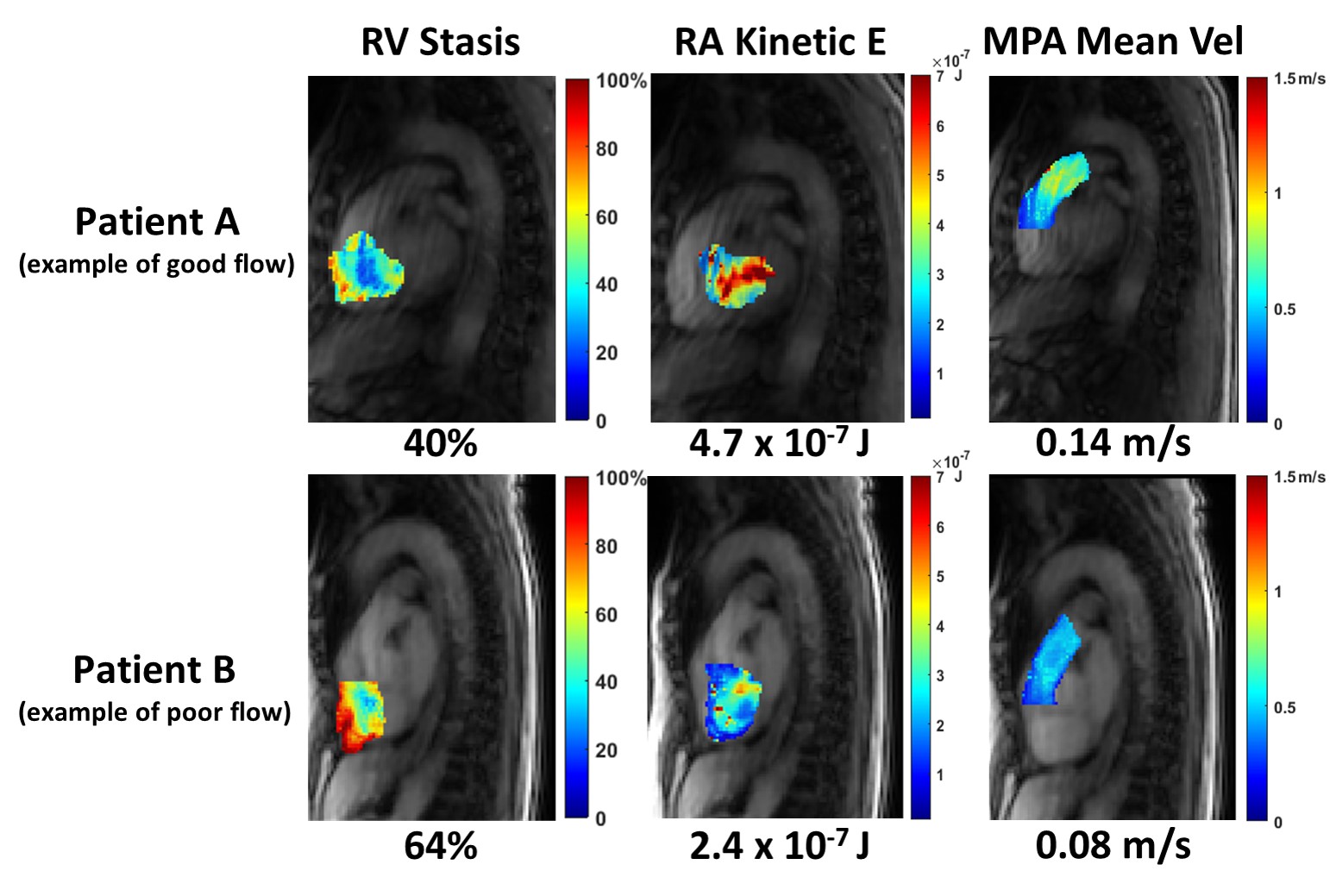
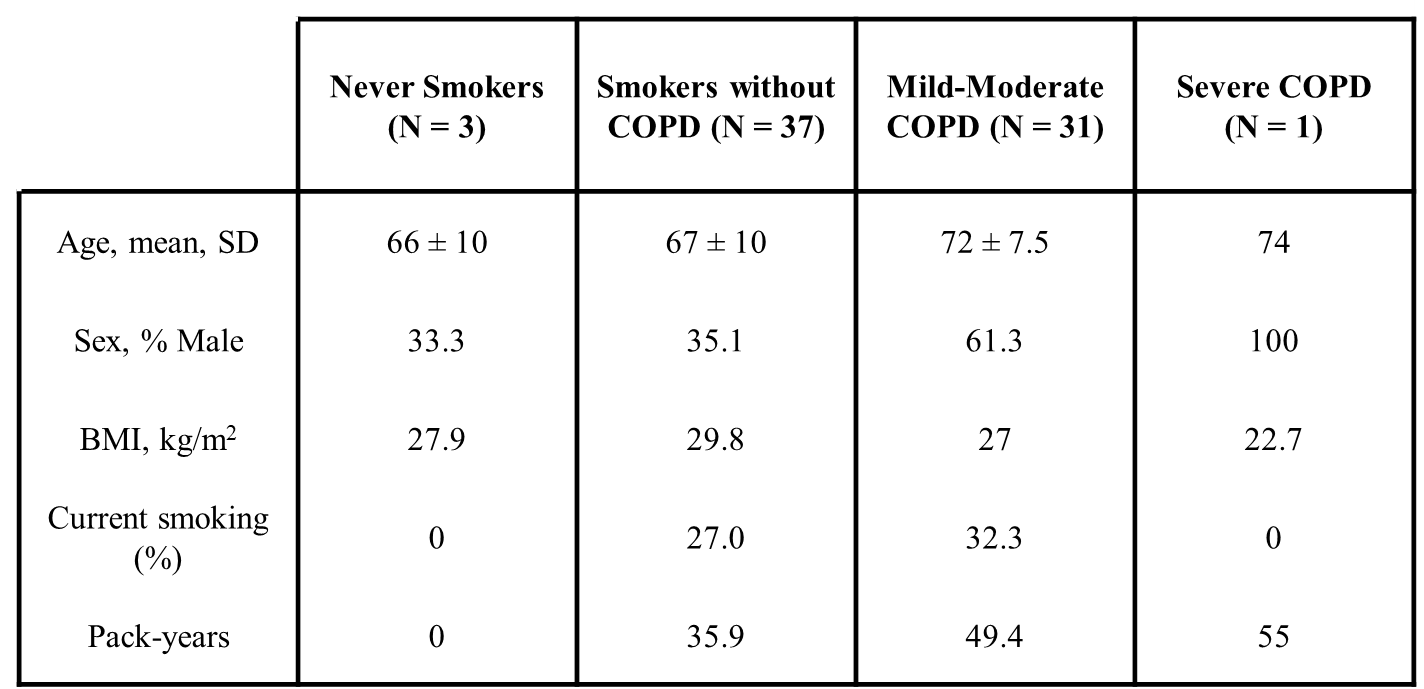
In the preliminary analysis of 72 participants, 32 had COPD (31 mild-moderate and 1 severe), 37 were controls with smoking history, and 3 were controls without smoking history. Table 1 summarizes the participants’ characteristics.Examples of RA, RV, and MPA hemodynamic parameters are illustrated in Figure 2. Participant A exemplifies relatively higher RA kinetic energy, lower RV stasis and higher MPA mean velocity, when compared to the mean findings. Participant B exemplifies poor flow where opposite findings were observed.
Lower lung function (i.e., lower forced expiratory volume in one second/forced vital capacity of the lung [FEV1:FVC ratio]) was associated with lower maximum velocity and kinetic energy of blood flow in the RA (r=0.52 and 0.48, respectively, both p<0.05).
Increasing COPD severity was associated with lower mean velocity (p=0.04) and with greater blood stasis (p=0.03) in the MPA. Greater percent emphysema on CT was also associated with lower mean blood velocity in the MPA (r=-0.43, p<0.05) (Table 2).
VEL was inversely correlated with total lung volume and residual volume (r= -0.29, p= 0.02 and r= -0.26, p= 0.04, respectively). VEL was also negatively correlated with MPA stasis (r= -0.33, p< 0.01).
Discussion
These 4D flow MRA results in 72 SPIROMIC-HF subjects highlight the altered cardiac blood flow and function in COPD. Our results suggest that more severe pulmonary disease is associated with slower velocities and increased stasis in the MPA as well as slower velocities and lower kinetic energy in the RA. COPD-induced chronic hypoxia is associated with pulmonary vascular remodeling11. The impaired flow could be attributed to COPD-induced increased pulmonary vascular resistance as a result of the remodeling process11,12.The inverse relation between VEL and stasis in the MPA is interesting since stasis was also associated with increased disease severity. This might indirectly imply that more energy is lost in the MPA with more severe lung pathology however a more comprehensive hemodynamic assessment is needed.
Our previous studies have demonstrated that vascular remodeling in COPD is linked to reduced left ventricular filling, reduced stroke volume, and lower cardiac output3,13,14. Our work suggests that COPD also affects upstream blood flow. This warrants further investigation of right-sided cardiac hemodynamics as well as venous return.
Our findings highlight associations between cardiac blood flow and pulmonary function which adds to the growing evidence of a complex cardiopulmonary hemodynamic interplay in COPD.
Acknowledgements
SPIROMICS HF was supported by grants from the NIH/NHLBI (R01-HL093081, R01-HL121270). SPIROMICS was supported by contracts from the NIH/NHLBI (HHSN268200900013C, HHSN268200900014C, HHSN268200900015C, HHSN268200900016C, HHSN268200900017C, HHSN268200900018C, HHSN268200900019C, HHSN268200900020C) and grants from the NIH/NHLBI (U01 HL137880, U24 HL141762, R01 HL182622, and R01 HL144718), supplemented by contributions made through the Foundation for the NIH and the COPD Foundation from Amgen; AstraZeneca/MedImmune; Bayer; Bellerophon Therapeutics; Boehringer-Ingelheim Pharmaceuticals, Inc.; Chiesi Farmaceutici S.p.A.; Forest Research Institute, Inc.; Genentech; GlaxoSmithKline; Grifols Therapeutics, Inc.; Ikaria, Inc.; MGC Diagnostics; Novartis Pharmaceuticals Corporation; Nycomed GmbH; Polarean; ProterixBio; Regeneron Pharmaceuticals, Inc.; Sanofi; Sunovion; Takeda Pharmaceutical Company; and Theravance Biopharma and Mylan/Viatris.References
1. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL and Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006; 355:251-259.
2. Smith, B. M., Prince, M. R., Hoffman, E. A., Bluemke, D. A., Liu, C. Y., Rabinowitz, D., ... & Barr, R. G. (2013). Impaired left ventricular filling in COPD and emphysema: is it the heart or the lungs?: the multi-ethnic study of atherosclerosis COPD study. Chest, 144(4), 1143-1151.
3. Aaron, C. P., Hoffman, E. A., Lima, J. A., Kawut, S. M., Bertoni, A. G., Vogel-Claussen, J., ... & Barr, R. G. (2017). Pulmonary vascular volume, impaired left ventricular filling and dyspnea: The MESA Lung Study. PloS one, 12(4), e0176180.
4. Barr, R. G., Bluemke, D. A., Ahmed, F. S., Carr, J. J., Enright, P. L., Hoffman, E. A., ... & Watson, K. E. (2010). Percent emphysema, airflow obstruction, and impaired left ventricular filling. New England Journal of Medicine, 362(3), 217-227.
5. Markl, M., Frydrychowicz, A., Kozerke, S., Hope, M., & Wieben, O. (2012). 4D flow MRI. Journal of Magnetic Resonance Imaging, 36(5), 1015-1036.
6. Markl, M., Kilner, P. J., & Ebbers, T. (2011). Comprehensive 4D velocity mapping of the heart and great vessels by cardiovascular magnetic resonance. Journal of Cardiovascular Magnetic Resonance, 13, 1-22.
7. Rahman, O., Markl, M., Balte, P., Berhane, H., Blanken, C., Suwa, K., Dashnaw, S., Wieben, O., Bluemke, D. A., Prince, M. R., Lima, J., Michos, E., Venkatesh, B. A., Hoffman, E. A., Gomes, A. S., Watson, K., Sun, Y., Carr, J., & Barr, R. G. (2019). Reproducibility and changes in vena caval blood flow by using 4D flow MRI in pulmonary emphysema and chronic obstructive pulmonary disease (COPD): the multi-ethnic study of atherosclerosis (MESA) COPD substudy. Radiology, 292(3), 585-594.
8. Frydrychowicz, A., François, C. J., & Turski, P. A. (2011). Four-dimensional phase contrast magnetic resonance angiography: potential clinical applications. European journal of radiology, 80(1), 24-35.
9. Walker, P. G., Cranney, G. B., Scheidegger, M. B., Waseleski, G., Pohost, G. M., & Yoganathan, A. P. (1993). Semiautomated method for noise reduction and background phase error correction in MR phase velocity data. Journal of Magnetic Resonance Imaging, 3(3), 521-530.
10. Bernstein, M. A., Zhou, X. J., Polzin, J. A., King, K. F., Ganin, A., Pelc, N. J., & Glover, G. H. (1998). Concomitant gradient terms in phase contrast MR: analysis and correction. Magnetic resonance in medicine, 39(2), 300-308.
11. Sakao S, Voelkel N, Tatsumi K. The vascular bed in COPD: pulmonary hypertension and pulmonary vascular alterations. European Respiratory Review. 2014; 23: 350-355.
12. Sommer N, Dietrich A, Schermuly R.T., Ghofranu H.A., Guderman T, Schulz R, Seeger W, Grimminger F, Weissmann N. Regulation of hypoxic pulmonary vasoconstriction: basic mechanisms. European Respiratory Journal. 2008; 32(6): 1639-1651.
13. Smith, B. M., Prince, M. R., Hoffman, E. A., Bluemke, D. A., Liu, C. Y., Rabinowitz, D., ... & Barr, R. G. (2013). Impaired left ventricular filling in COPD and emphysema: is it the heart or the lungs?: the multi-ethnic study of atherosclerosis COPD study. Chest, 144(4), 1143-1151.
14. Barr, R. G., Bluemke, D. A., Ahmed, F. S., Carr, J. J., Enright, P. L., Hoffman, E. A., ... & Watson, K. E. (2010). Percent emphysema, airflow obstruction, and impaired left ventricular filling. New England Journal of Medicine, 362(3), 217-227.
Figures