0100
Referenceless 4D Flow MR for cardiac imaging1Department of Health, Medicine and Caring Sciences (HMV), Linköping University, Linköping, Sweden, 2Center for Medical Image Science and Visualization (CMIV), Linköping, Sweden, 3Linköping University, Linköping, Sweden, 4Analytic Imaging Diagnostics Arena (AIDA), Linköping, Sweden, 5Department of Clinical Physiology, and Department of Health, Medicine and Caring Sciences (HMV), Linköping University, Linköping, Sweden
Synopsis
Keywords: Flow, Data Processing, Image reconstruction
Motivation: Scan times for clinical 4D Flow MRI are still around 5-10 mins, which is too long for ideal integration in clinical practice.
Goal(s): To investigate the possibility to reduce scan time by reconstructing three-directional velocity without the acquisition of reference scan in cardiac applications.
Approach: Training a conditional generative adversarial network (cGAN) to estimate the reference scan from the three-velocity encoded scan segments.
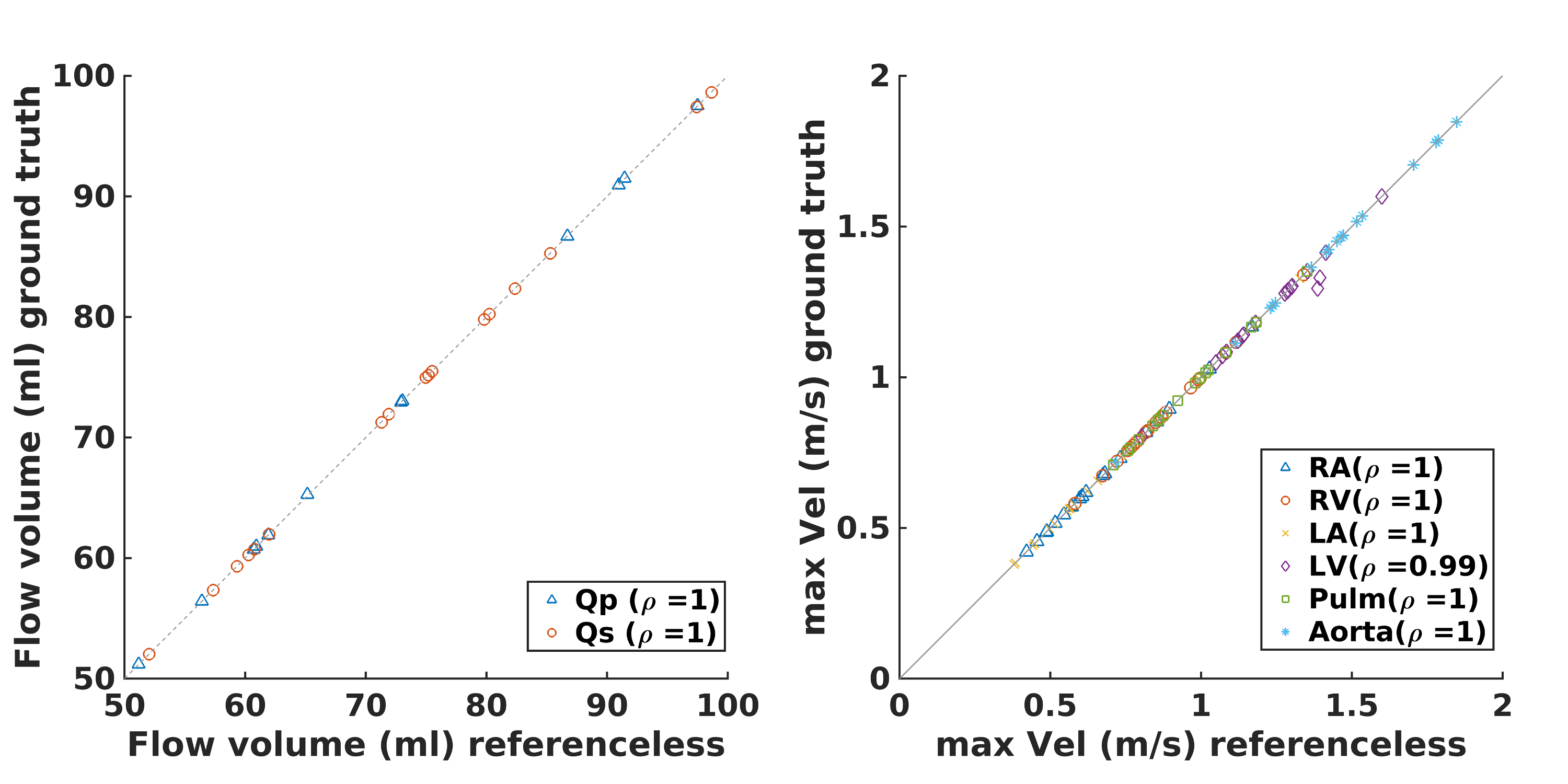
Results: Correlation coefficients for the pulmonary and systemic flow volumes and for maximum velocities were higher than 0.99, showing an excellent agreement between the cGAN-enabled referenceless 4D Flow MRI and conventional 4D flow MRI, thus potentially reducing scan time.
Impact: By reconstructing the three-directional velocity without the reference scan it is possible reduce scan time of 4D Flow MRI, alleviating costs and patient discomfort, which especially is important for elderly and impaired subjects.
Introduction
Three-dimensional cine phase-contrast magnetic resonance imaging (4D Flow MRI) is an excellent tool for the assessment of hemodynamics in the cardiovascular system. However, scan times for clinical 4D Flow MRI are still around 5-10 mins, which is too long for ideal integration in clinical practice1. One approach to reduce scan time is to only acquire three of the four flow encodings, whereby the acquisition of the reference scan used to correct for inhomogeneities in the static magnetic field is omitted. Recently, a convolutional neural network was used to reconstruct three-directional velocity without the reference scan in the brain2. In this study, we investigated the possibility to reconstruct three-directional velocity from referenceless 4D Flow MRI for cardiac applications.Methods
The set of 4D Flow data used in this study comprised 97 subjects, including healthy individuals and patients with different types of cardiomyopathy. Free-breathing, respiratory motion-navigated, sagittal 4D Flow MRI with a non-symmetric flow encoding scheme were acquired on a 3T scanner (Philips Ingenia, Philips Healthcare, Best, the Netherlands). The dataset was divided into 70% training (n=70), 10% validation (n=8) and 20% test set (n=19). For each subject, the uncorrected scans SS1-4 were reconstructed, where SS1 represents the reference scan and SS2-4 the flow encoded scans.A 2D conditional generative adversarial network (cGAN) was trained to predict the correction (i.e. the SS1 reference scan). The model was adapted from a previously publish model implemented for image-to-image translation3, to have a six channel input, i.e. the real and imaginary part of the MRI signal for the three velocity encoded scans, and a two channel output, i.e. the real and imaginary part for the reference scan. Half of the timeframes (n=20) were used for training and each slice in the 4D Flow dataset was input separately. On the test subjects, all timeframes in the 4D Flow data were used.
The velocity encoded scans were corrected with the SS1 reference scan generated by the cGAN (“referenceless data”) and with the SS1 reference scan acquired on the scanner (“ground truth data”). Pearson’s correlation coefficient was used to assess the agreement between velocity in the whole heart in the ground truth versus referenceless 4D Flow MRI velocity data. Bland Altman analysis was performed for whole-heart velocity each timeframe to assess the presence of bias in the referenceless velocity data. Additionally, all data were corrected for background phase offset and phase-wraps to compute pulmonary flow volume (Qp) and systemic flow volume (Qs). Moreover, the maximum peak systolic velocity was extracted for all cardiac chambers and major vessels4.
Results
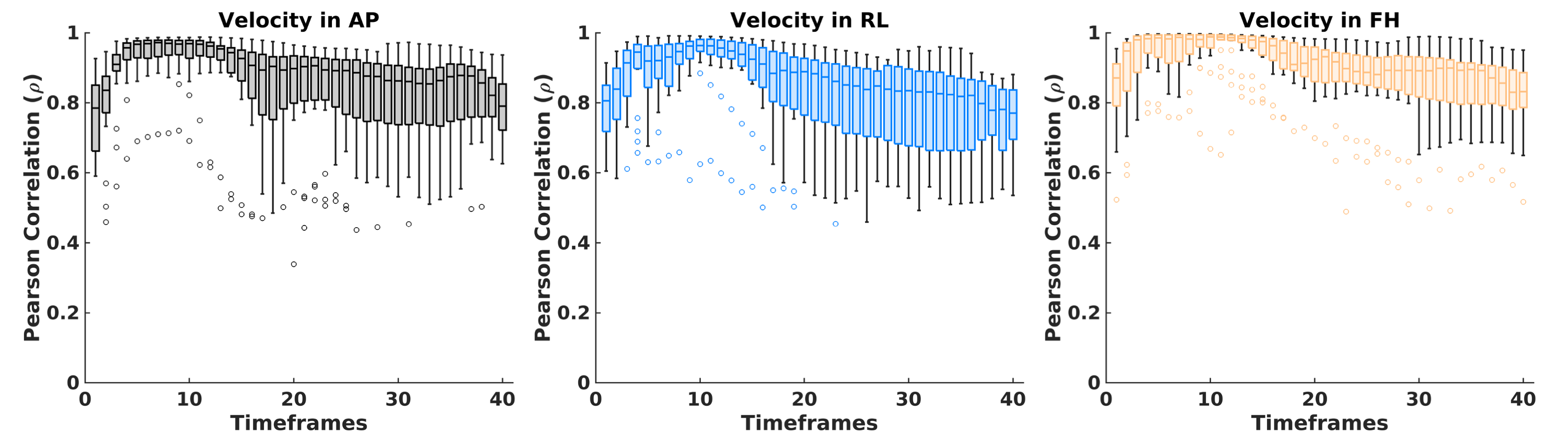
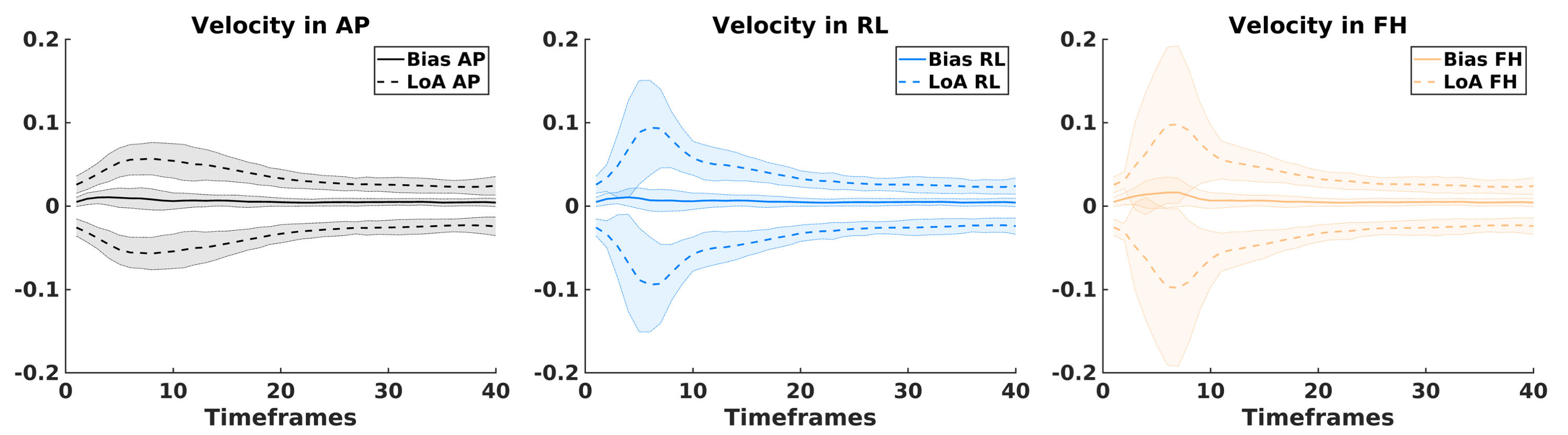
Person’s correlation coefficients reported as median in the test set at peak systole were 0.97, 0.93, and 0.99 for the anterior-to-posterior, right-left, and foot-to-head velocity components, respectively (p<0.001). Correlations coefficients were higher in systole, and lower in the diastolic timeframes, as expected from the different distribution of velocities (Figure 1). At peak systole, the median velocity bias was 0.0092, 0.0066, and 0.0163 and the median limits of agreements were ±0.0560, ±0.0930, and ± 0.0978 for the anterior-to-posterior, right-left, and foot-to-head velocity components, respectively. The bias was constant in time, while the limits of agreement were larger in the systolic timeframes (Figure 2). Person correlations for flow volumes and maximum peak velocities were all higher than 0.99 (p<0.001) (Figure 3).Discussion
There was excellent agreement between 4D Flow MRI velocity data estimated with cGAN-enabled referenceless 4D Flow MRI and ground truth. A previous study employed convolutional neural network for referenceless 4D Flow MRI noted an underestimation of velocity with the referenceless approach2. We did not note such an underestimation with our cGAN approach. A potential advantage of using a cGAN is that velocity-based weighting of the loss function is not needed. Velocity-based weighting could be problematic in diastole when velocities are low. In a 4D Flow sequence with a k-space segmentation factor of 2 and repetition time of 4 ms, referenceless 4D Flow could either be used to improve the temporal resolution from 32 ms to 24 ms or, by increasing the k-space segmentation factor to 3, to reduce the scan time by 33% with a temporal resolution of 36 ms.Conclusion
cGAN-enabled estimation of the reference scan permits 4D flow MRI with only the three velocity encodings. Reduced scan time leads to reduced costs and patient discomfort, which is especially important for elderly and impaired patients. Future research should be directed at training referenceless 4D Flow MRI with a broader representation of different scanner manufacturers, acquisition schemes, field strengths, with and without contrast agents, as well as different pathologies.Acknowledgements
We acknowledge support received from Philips Clinical Science, Sweden.References
1. Bissell, M. M. et al. 4D Flow cardiovascular magnetic resonance consensus statement: 2023 update. J. Cardiovasc. Magn. Reson. 25, 40 (2023).
2. Kim, D., Jen, M.-L., Eisenmenger, L. B. & Johnson, K. M. Accelerated 4D-flow MRI with 3-point encoding enabled by machine learning. Magn. Reson. Med. n/a, (2022).
3. Isola, P., Zhu, J.-Y., Zhou, T. & Efros, A. A. Image-to-Image Translation with Conditional Adversarial Networks. in 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR) 5967–5976 (IEEE, 2017). doi:10.1109/CVPR.2017.632.
4. Bustamante, M. et al. Atlas-based analysis of 4D flow CMR: Automated vessel segmentation and flow quantification. J. Cardiovasc. Magn. Reson. 17, 87 (2015).
Figures