0099
MRI-based analysis of the blood flow in the left ventricle: 2D geometry-prescribed Cine-MRI based model versus 4D-Flow CMR1Mechanical Engineering, Polytechnique Montreal, Montreal, QC, Canada
Synopsis
Keywords: Flow, Cardiovascular, Analysis/Processing, Data Processing, Flow, Heart, In Silico, Modelling, Simulation/Validation, Simulations, Velocity & Flow
Motivation: 4D-Flow CMR allows to analyze 3D blood flow patterns in the left ventricle, however it requires time-consuming acquisitions and complex pre and post-processing.
Goal(s): The objective is to develop a method to analyze blood flow patterns in the left ventricle without these disadvantages.
Approach: Using Cine-MRI and patient-specific modelling techniques, we introduced a new and semi-automated method to simulate the blood flow inside the left ventricle. Accuracy of the developed method was evaluated by comparing the results to 4D-Flow CMR analysis performed on one healthy subject.
Results: Both techniques showed similar blood flow patterns and comparable hemodynamics parameters.
Impact: This patient-specific model is a relatively simple and time-saving method allowing blood flow analysis in the left ventricle based on Cine-MRI acquisition. It may be used to characterize blood flow in patients with heart disease at rest or under stress.
Introduction
Doxorubicin-based chemotherapy, used in childhood acute lymphoblastic leukemia (cALL), has been proven to induce cardiomyopathy 1. Its side effects on cardiac muscles has been associated with heart failure in several patients 2. Early diagnosis of this cardiotoxicity remain a challenge. Hemodynamics in the left ventricle is a known biomarker of cardiac health 3. Therefore, we aim to characterize blood flow in the left ventricle in these patients, using MRI data and modelling techniques. 4D-Flow CMR is a recent technique allowing to extract velocity in 3D, but its application is still limited in clinical studies due to long acquisition time, reduced temporal and space resolution and complex pre and post-processing. Thus, a new method based on Cine MRI and modelling techniques was developed to study blood flow in the left ventricle. To verify the feasibility, the developed method is compared to 4D Flow CMR.Methods
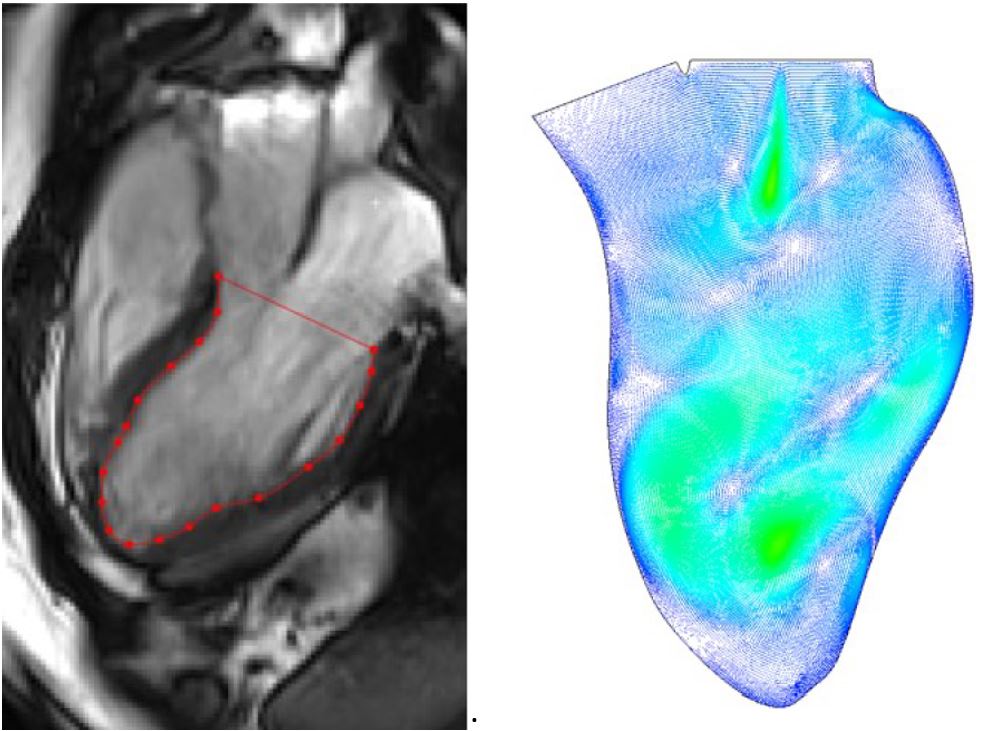
The developed model relies on an automated approach, using ®MATLAB and ANSYS FLUENT, to simulate the blood flow inside the left ventricle in 2D, based on the prescribed geometry method 4 and CMR imaging. The model takes as input the manual segmentation of 3-Chambers view, and gives as outputs the simulated blood flow, depending on chosen spatial and temporal resolution and interpolation parameter (Figure 1). The 3-Chambers view was acquired on a Siemens Skyra 3 Tesla system using a 18-channel body coil and a BSSFp sequence (10 mm slice thickness, 2mm Gap between slices, 2.0x2.0x10mm3 Voxel size, 25 Number of phases, 1 heartbeat per slice) on an healthy volunteer. The segmentation was performed manually on Segment (Medviso). Verification, validation and review of the model was performed using literature data and 4D Flow CMR imaging of the left ventricle in the same healthy volunteer.Results
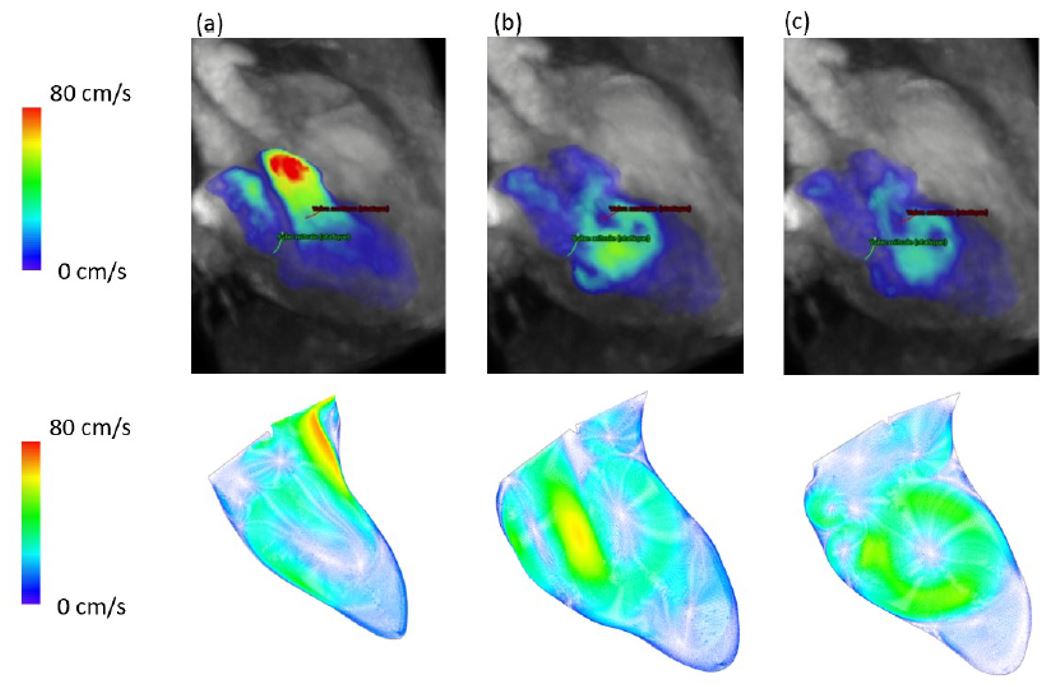
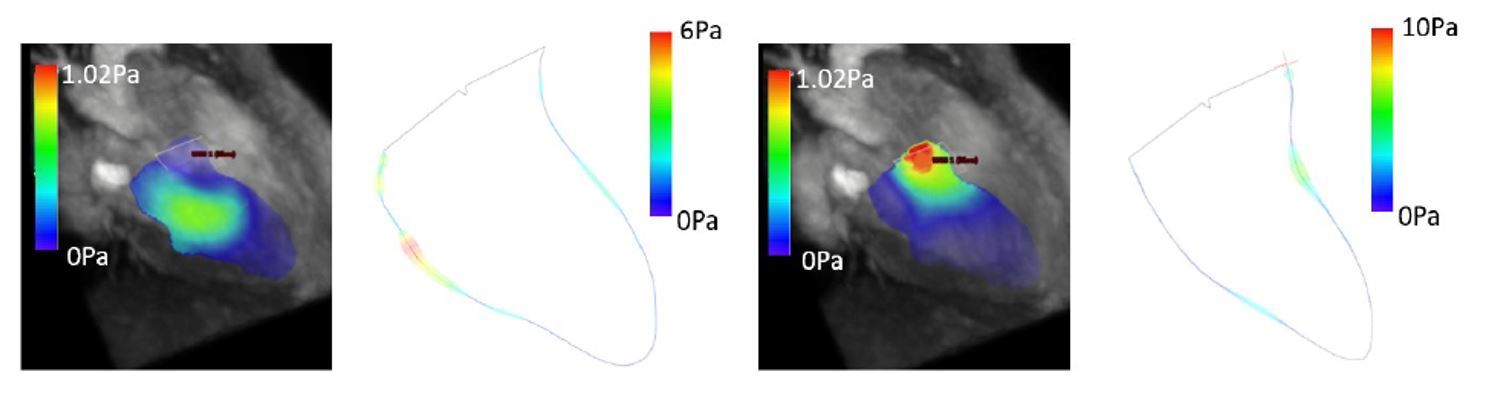
Results obtained with a simplified mobile indentation model were found to be identical to the literature, indicating a successful implementation. A sensitivity analysis of the temporal interpolation parameter was realized to assess the impact of a variation in the smoothing of the manual segmentation. Spatial resolution parameters, time-step, linearization residuals and the number of modeled cycles were identified to allow independent results, while reducing computation time. The developed model required only a few seconds of acquisition time, while the 4D Flow CMR required the patient to stay still and have a regular breathing for 20 minutes. Manual segmentation of the 3-Chambers view and 4D Flow MRI took roughly the same time. Spatial resolution of the simulation is 0.3mm, temporal resolution is T/1000, T being the duration of one cardiac cycle. Spatial resolution of the 4D Flow MRI was 2.1mm, and the temporal resolution was T/20. Temporal velocity at the aortic and mitral valve, and maximal speed in the left ventricle showed a similar pattern and order of magnitude, although maximal speed at the valves were slightly slower in our model compared to 4D Flow MRI data (Figure 2). A similar intraventricular diastolic vortex was found in both analyses. Finally, shear stress magnitude was found to be higher in our model (Figure 3), but of the same order of magnitude at similar locations of the ventricular walls.Discussion
Comparison of the two methods showed similar patterns and the same order of magnitude in hemodynamic parameters. Observed differences could be explained by the large dissimilarity in spatial and temporal resolutions. The developed method is based on a simple acquisition, requiring only a few seconds. Indeed, 4D Flow MRI require a long acquisition time, which increases when good spatial and temporal resolution are needed. Moreover, conditions of the 4D Flow acquisition may not be suited for clinical purposes and for larger cohorts of patients. Finally, our model only requires 2D manual segmentation of the 3-Chambers view and a few seconds to launch the automated simulation process.Conclusion
This study presents a new MRI-based model to assess hemodynamics forces in the left ventricle. This model allows a patient-specific analysis and gives results that are comparable to those obtained using 4D Flow CMR. However, our method is based on a very short acquisition time and a better repeatability and reproducibility. Automated simulation allows to be more time-efficient. Finally, this model allows to perform new analysis, such as analysis of the blood flow in patients with left ventricular dysfunction. Our lab aims to use this model to characterize the blood flow at rest, and after an exercise performed directly in the MRI machine, which could allow to find early biomarkers of cardiac dysfunction and help identify patients at risk.Acknowledgements
Montreal Heart Institute (MHI) for providing MRI access and assistance in cine-MRI acquisition, Mechanical lab students for their availability and FRQNT, TransMedTech Institute and Polytechnique Montreal for financial supports.References
1. S. Marcoux, S. Drouin, C. Laverdière, N. Alos, G. Andelfinger, L. Bertout, D. Curnier, M. Friedrich, E. Kritikou, G. Lefebvre, E. Levy, S. Lippé, V. Marcil, M.-J. Raboisson, F. Rauch, P. Robaey, M. Samoilenko, C. Séguin, S. Sultan et D. Sinnett, “The PETALE study : Late adverse effects and biomarkers in childhood acute lymphoblastic leukemia survivors,” Pediatr Blood Cancer, vol. 64, 2016.
2. M. Aissiou, F. Cheriet, D. Curnier, T. Hafyane, M. Friedrich, C. Laverdiere, G. Andelfinger, M. Krajinovic, D. Sinnett et D. Perie, “Early detection of doxorubicin induced cardiotoxicity using myocardial t1 and t2 relaxation times,” Canadian 93 Journal of Cardiology, vol. 32, no. 10, p. S298, 2016.
3. G. Pedrizzetti, A. R. Martiniello, V. Bianchi, D. Antonio, P. Caso et G. Tonti, “Cardiac fluid dynamics anticipates heart adaptation,” J Biomech., 2015.
4. S. N. Doost, L. Zhong, B. Su et Y. S. Morsi, “Two-dimensional intraventricular flow pattern visualization using the image-based computational fluid dynamics,” Computer Methods in Biomechanics and Biomedical Engineering, vol. 20, no. 5, p. 492–507, 2017.
Figures