0098
Assessment of Pulmonary Arteries Hemodynamics in Athletes with 4D Flow MRI1Department of Radiology, The Affiliated Hospital of Southwest Medical University, Luzhou, China, 2MR Research Collaboration, Siemens Healthineers, Chengdu, China
Synopsis
Keywords: Flow, Heart, Athlete; Pulmonary artery; 4D flow
Motivation: Long-term intense training in athletes can lead to pathological cardiac remodeling (CR) and potential myocardial fibrosis (MF), raising cardiovascular risks.
Goal(s): Employ 4D flow MRI to study pulmonary arterial hemodynamics in athletes and explore correlations with CR and MF.
Approach: Scanned 121 athletes and 21 controls using 3 T MRI scanner; 4D flow data analysis on CVI42; built machine learning models for differentiation based on cardiovascular conditions.
Results: Found significant associations between the altered pulmonary arterial hemodynamics parameters and CR and/or MF. Machine learning models identified athletes with cardiac anomalies.
Impact: We indicated that exercise can induce remodeling of the pulmonary circulation in athletes. The evaluation of pulmonary arterial 4D flow hemodynamics parameters can be beneficial for clinical follow-up of athletes.
Introduction
Long-term intense exercise training may result in pathological cardiac remodeling (CR), which is difficult to differentiate from physiological CR1-3. Ultimately, this pathological remodeling can lead to myocardial fibrosis (MF), which serves as a substrate for right-sided ventricular arrhythmias, particularly right ventricular outflow tract ventricular tachycardia, and increases cardiovascular risk2-4. Early detection of hemodynamic changes in the pulmonary arteries among athletes on an individual basis could prove beneficial in the early detection of CR and MF, thus helping adjust the frequency of clinical follow-up of athletes5,6. Four-dimensional (4D) flow MRI is a promising noninvasive technique for evaluating blood flow velocity and volume with high consistency, with results comparable to catheterization. It has been widely applied in various cardiovascular conditions. We aimed to investigate the hemodynamics of pulmonary arteries in athletes using 4D flow MRI and its relationship with CR and/or MF by combining machine learning (ML) methods.Methods
Athletes (n = 121) and sedentary healthy controls (n = 21) were enrolled and underwent examination with a 3 T scanner (Siemens Healthineers, Eriangen, Germany) equipped with an 18-channel body coil. The cine images was employed to acquire with breath-holding and scanning parameters of repetition time (TR) = 3.31 ms, echo time (TE) = 1.46 ms, field of view (FOV) = 340 × 270 mm², matrix size = 256 × 186 pixels, and segments = 20. Data from 4D flow MRI were acquired during free breathing using a prospectively electrocardiography-gated, time-resolved, three-dimensional, Cartesian phase-contrast MR sequence. The imaging volume encompassed the heart and pulmonary arteries in a sagittal plane. Typical imaging parameters were TR = 22.68 ms, TE = 2.88 ms, velocity encoding = 150 cm/s in all three velocity-encoding directions, spatial resolution = 1.8 × 1.8 × 3.5 mm3, and segments = 2. Approximately 10 minutes after intravenous injection of a gadolinium contrast agent, late gadolinium enhancement imaging was performed. The parameters were TR = 18.22 ms, TE = 1.24 ms, FOV = 340 × 270 mm2, matrix = 256 × 186, and segments = 51. All images were transferred to a CVI42 (cmr 42, v. 5.12.4; Circle Cardiovascular Imaging, Calgary, Canada) workstation and analyzed independently by four independent investigators. An analysis comparing basic clinical features, cardiac function parameters, the 4D flow parameters of the pulmonary arteries between athletes and controls and between athletes with and without CR and/or MF was conducted. And the construction of four ML models, including gradient-boosting machine, support vector machine, logistic regression, and classification and regression tree, were conducted in R software (version 3.6.3).Results
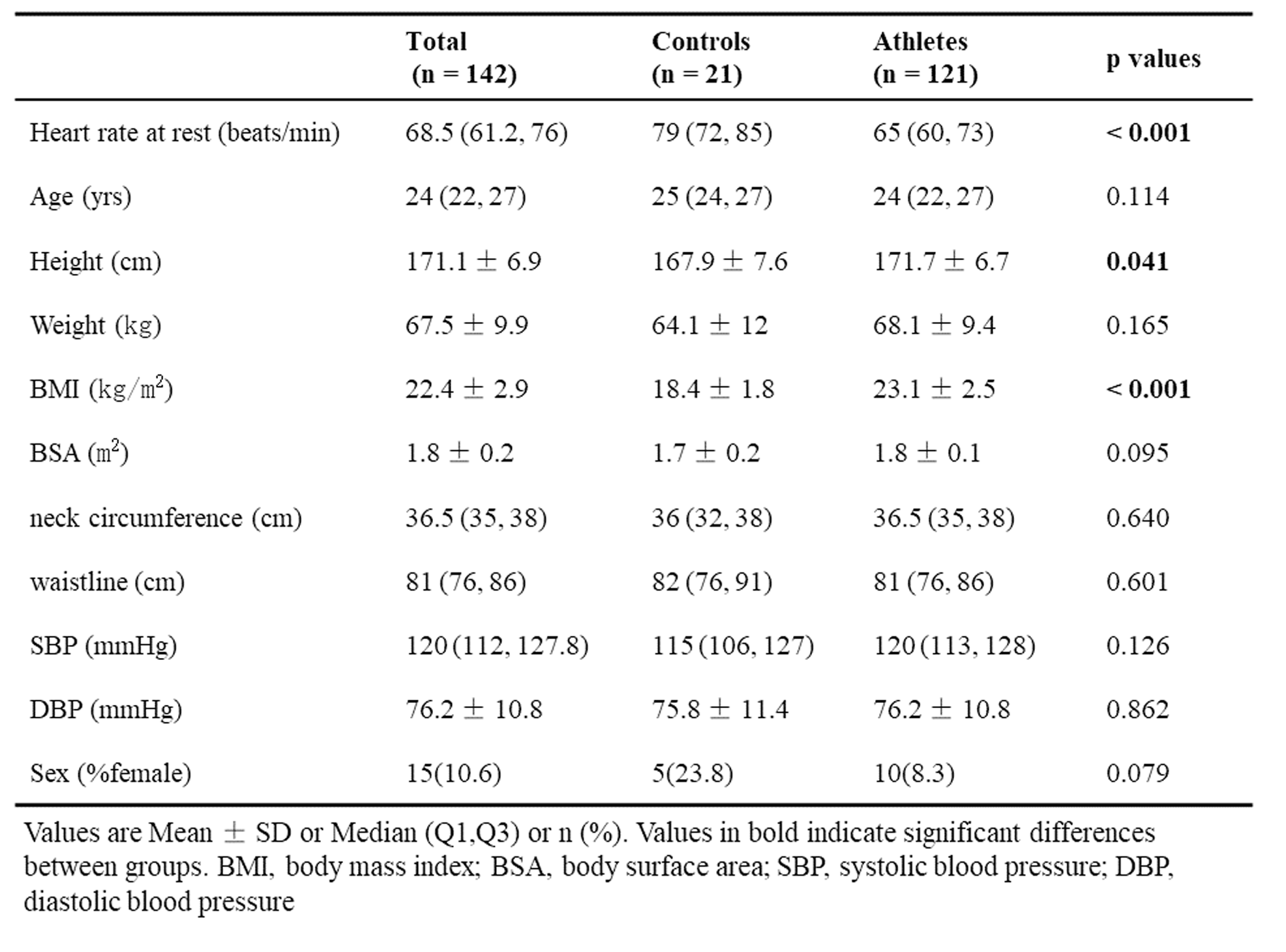
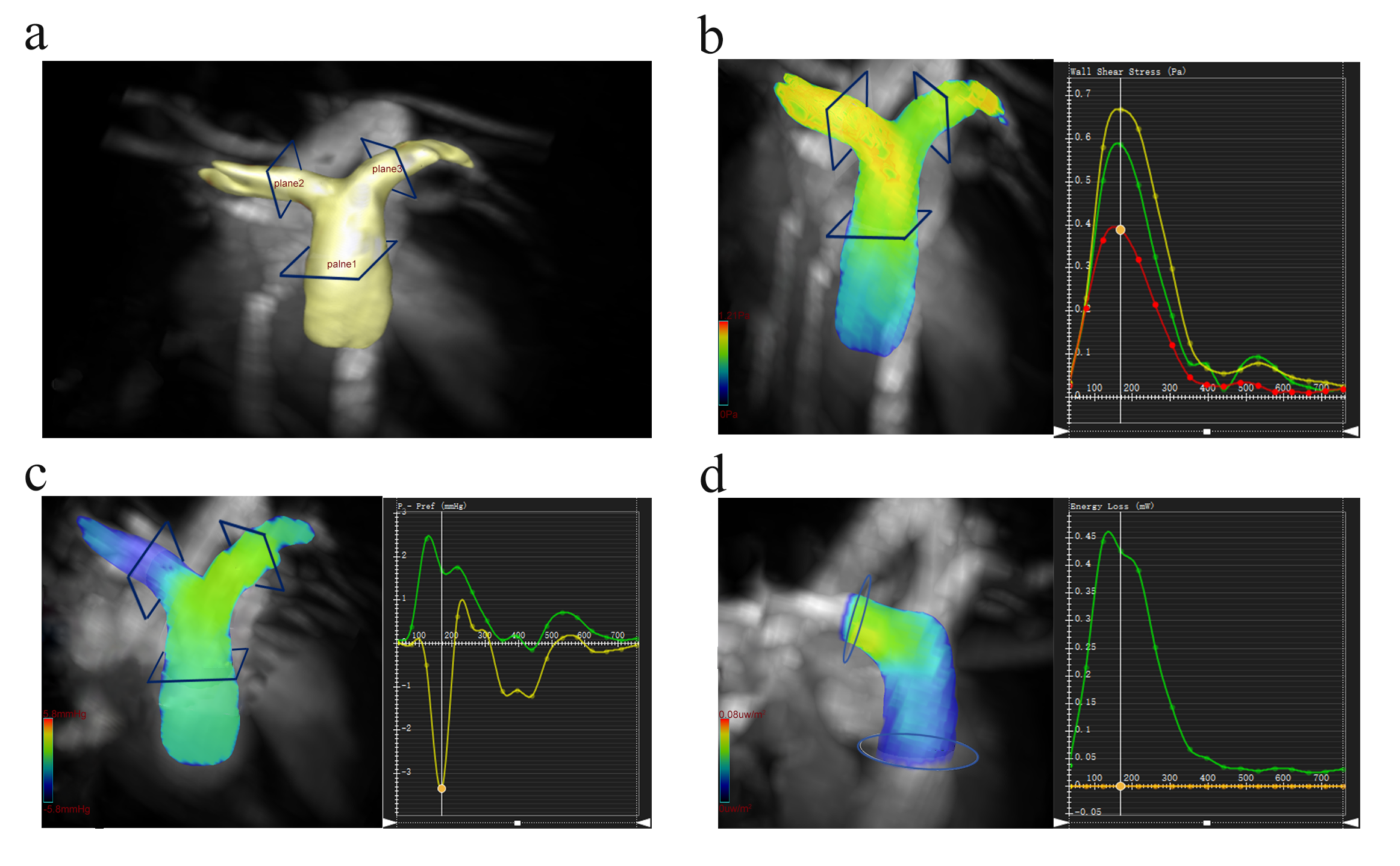
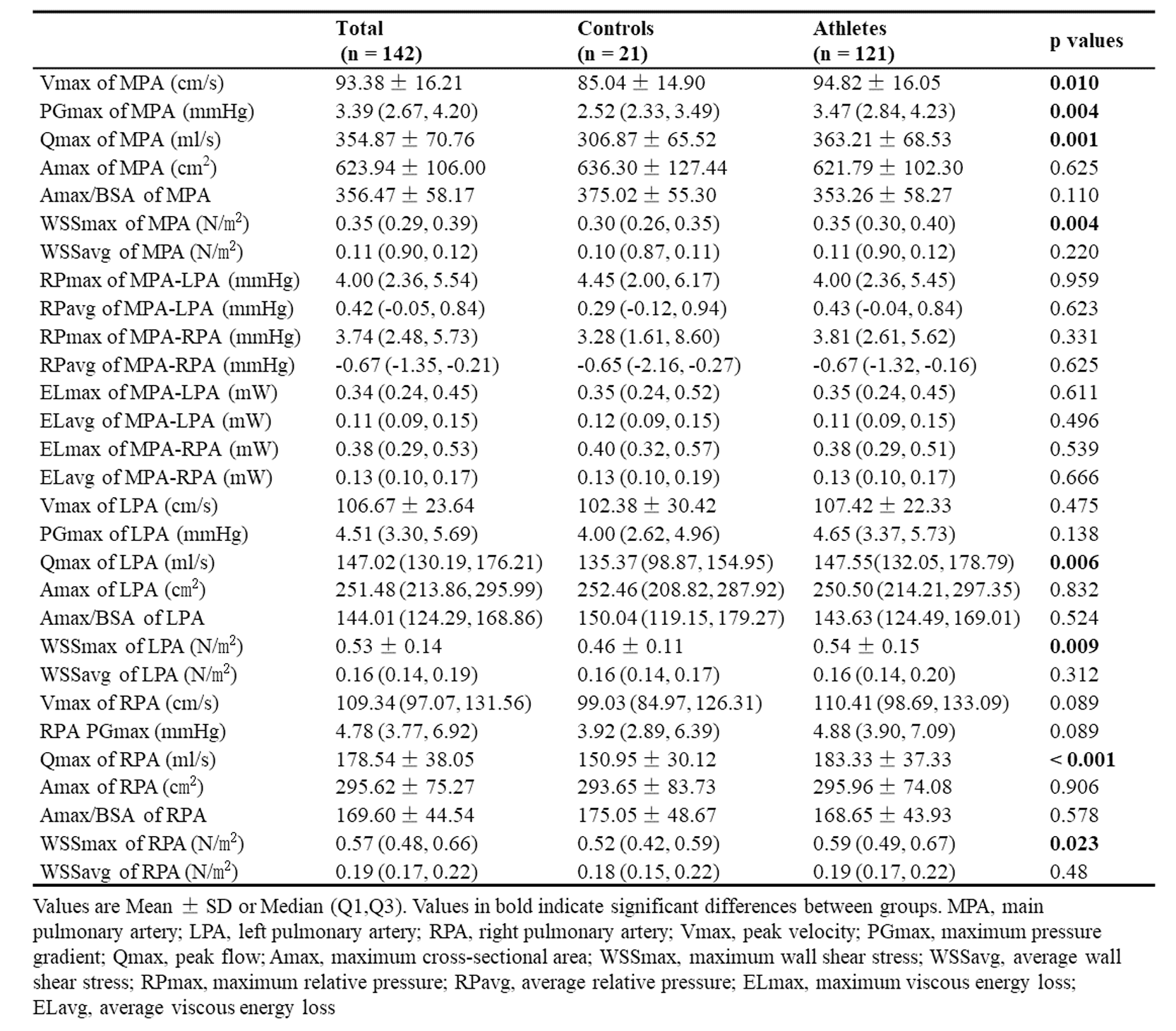
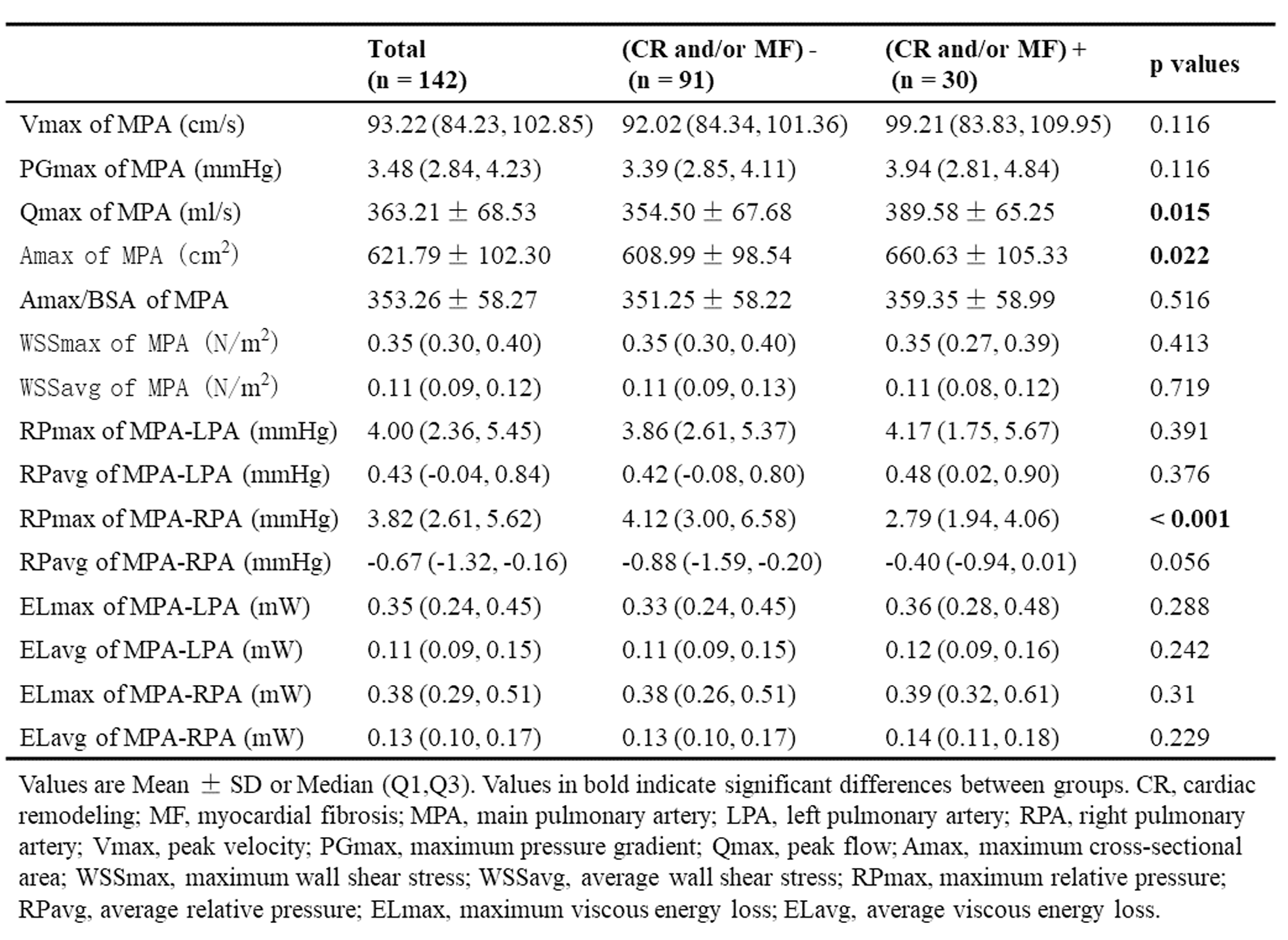
The basic clinical characteristics of the athletes and control group are shown in Figure 1. There were 30 male athletes with CR and/or MF (26 athletes with CR solely, 2 athletes with CR and MF, and 2 athletes with MF solely). Figure 2 shows an exemplary image of the 4D flow data analysis on CVI42 software from an athlete. The comparisons of 4D flow hemodynamics parameters and sizes of main, right and left pulmonary arteries (MPA, RPA and LPA, respectively) between groups are shown in Figure 3 and Figure 4. Athletes had significantly higher maximum wall shear stress (WSSmax) of MPA, RPA, and LPA than the control group. Athletes with CR and/or MF had significantly larger maximum cross-sectional area (Amax) of MPA and significantly lower maximum relative pressure (RPmax) from MPA to RPA than athletes without CR and/or MF. The four ML models had excellent performance, with areas under the curve of 0.90, 0.75, 0.79, and 0.89, respectively.Discussion
This was a preliminary feasibility study of 4D flow MRI for the evaluation of the hemodynamics of athletes' pulmonary arteries. Based on our data, we speculate that exercise may decrease resistance and pressure in pulmonary circulation, thereby increasing pulmonary circulation capacity, which is beneficial for physical activity. However, enlarged pulmonary arteries may lead to adverse vascular remodeling5,6. Therefore, based on the 4D flow parameters of the pulmonary arteries, four ML models were established for the early detection of CR and/or MF, both of which are associated with cardiovascular adverse events2-4. This personalized assessment of pulmonary vascular response to exercise could potentially assist the optimization of the clinical follow-up frequency of athletes and may facilitate their management and care5.Conclusion
Overall, exercise may induce remodeling of the pulmonary circulation in athletes. Based on the established ML model incorporating 4D flow parameters, athletes with CR and/or MF can be differentiated from those without, which can be beneficial for clinical follow-up of athletes.Acknowledgements
We wish to thank all the participants who kindly volunteered their time for this study.References
1. Parry-Williams G, Sharma S. The effects of endurance exercise on the heart: Panacea or poison?. Nat Rev Cardiol. 2020;17(7):402-412.
2. Venlet J, Piers SR, Jongbloed JD, et al. Isolated subepicardial right ventricular outflow tract scar in athletes with ventricular tachycardia. J Am Coll Cardiol. 2017;69(5):497–507.
3. van de Schoor FR, Aengevaeren VL, Hopman MT, et al. Myocardial fibrosis in athletes. Mayo Clin Proc. 2016;91(11):1617–1631.
4. O'Keefe JH, Patil HR, Lavie CJ, Magalski A, Vogel RA, McCullough PA. Potential adverse cardiovascular effects from excessive endurance exercise [published correction appears in Mayo Clin Proc. 2012 Jul;87(7):704]. Mayo Clin Proc. 2012;87(6):587–595.
5. Domenech-Ximenos B, Garza MS, Prat-González S, et al. Exercise-induced cardio-pulmonary remodelling in endurance athletes: Not only the heart adapts. Eur J Prev Cardiol. 2020;27(6):651–659.
6. Martínez V, Sanz-de la Garza M, Domenech-Ximenos B, et al. Cardiac and pulmonary vascular remodeling in endurance open water swimmers assessed by cardiac magnetic resonance: Impact of sex and sport discipline. Front Cardiovasc Med. 2021;8:719113.
Figures