0097
Non-invasive Assessment of Left Ventricular Hemodynamic Forces in Mitral Patients using 4-Dimensional Flow Magnetic Resonance Imaging1Biomedical Engineering, University of Calgary, Calgary, AB, Canada, 2Radiology, University of Calgary, Calgary, AB, Canada
Synopsis
Keywords: Valves, Quantitative Imaging, Mitral Valve Regurgitation, Hemodynamic Force, Novel Biomarker
Motivation: This study aims to address shortcomings in assessing mitral regurgitation (MR) by introducing left ventricular hemodynamic force (HDF) as a novel biomarker.
Goal(s): The primary objective of this study is to assess HDF's reliability through 4D flow MRI in distinguishing MR patients from healthy controls and stratifying severity, offering a more precise diagnostic tool.
Approach: This retrospective analysis used 4D flow MRI data to compute HDF in three directions, evaluating its correlation with MR.
Results: MR patients exhibit significantly altered HDF compared to controls. The HDF: peak systolic base-apex, E-wave inferior-anterior, E-wave base-apex, and peak diastolic septal-lateral suggest their potential as mitral biomarkers.
Impact: The introduction of hemodynamic force as a novel biomarker opens new research avenues, potentially reshaping cardiac non-invasive diagnostic techniques. This study may transform the assessment of mitral regurgitation, offering benefits to clinicians for early intervention and proper patient management.
Introduction
Mitral regurgitation (MR) is caused by the retrograde blood flow from the left ventricle (LV) to the left atrium (LA) due to a defective mitral valve. MR is one of the common types of valvular heart disease (VHD) in developed countries. It affects around 3% of the world’s population and the prevalence increases as people age1. Doppler echocardiography is the primary imaging assessment tool commonly used for assessing MR. However, echocardiography has limitations in determining the severity level and post-surgical outcomes. Recent studies have shown that cardiac magnetic resonance (CMR) and 4-dimensional flow magnetic resonance imaging (4D flow MRI) can provide a more accurate depiction of the regurgitant jet and flow patterns overcoming the limitations of echocardiography2. Recent cardiovascular studies have emphasized the importance of hemodynamic force (HDF) as a biomarker for cardiac diseases3. However, it is still not routinely used for the diagnosis or severity stratification of MR due to poor image quality from echocardiography and invasive procedures of catheterization4. In this study, we aimed to non-invasively assess and describe the LV-HDF in mitral patients using 4D flow MRI. We hypothesized that HDF may serve as a biomarker to identify MR and stratify its severity level.Methods
The 4D flow MRI-based data (collected from 3T MRI scanners) was retrospectively obtained for the controls (n=15, male=53%) and patients with ‘Trivial-Severe’ MR (n=26, male=54%) (aged 19-75 years). Severity levels were categorized according to the European and American imaging guidelines. The ‘Segment’ software v2.2 R6410 (Sweden, Medviso) was used for HDF analysis. The HDF was computed in three directions (septal-lateral, inferior-anterior, and basal-apical) using the Navier-Stokes equation and integration of pressure gradients ‘g’ over LV volume5. The statistical analysis was performed by IBM SPSS Statistics software for Windows (v26). The P-value<0.05 was considered statistically significant.Results
Sex-matched differences were observed between controls and patients. In males: peak systolic inferior-anterior, peak systolic base-apex (PS B-A), E-wave septal-lateral, peak diastolic inferior-anterior, peak diastolic base-apex, and A-wave septal-lateral showed significant differences between controls and patients (0.66 vs. 0.88, 2.5 vs. 1.79, 0.34 vs. 0.57, 0.66 vs. 0.21, 1.93 vs. 0.79, and 1.67 vs. 0.37, P<0.05; respectively). In females: peak systolic base-apex, E-wave base-apex (E-W B-A), peak diastolic septal-lateral (PD S-L), peak diastolic inferior-anterior, and peak diastolic base-apex demonstrated significant differences between controls and patients (2.88 vs. 1.55, 2.49 vs. 1.54, 0.52 vs. 0.23, 0.81 vs. 0.36, 2.5 vs. 0.85, P<0.05; respectively). Among HDFs, PS B-A, E-wave inferior-anterior (E-W I-A), E-W B-A, and PD S-L, and among LV functions, LV end-diastolic volume (LVEDV), LVEDV indexed (LVEDVI), LV mass (LVM), LVM indexed (LVMI) showed a positive correlation with MR severity (ρ=0.45, ρ=0.40, ρ=0.59, ρ=0.47, ρ=0.54, ρ=0.55, ρ=0.60, ρ=0.55, P<0.05; respectively). From these variables, PS B-A, E-W B-A, LVMI, LVM, LVEDVI, and LVEDV demonstrated significant differences among MR severities (P<0.05). In mild-moderate MR, E-W I-A negatively correlated with age and LVMI (r=-0.714, r=-0.66, P<0.05; respectively). In contrast, LVMI and LVM showed a strong positive correlation with age (ρ=0.645, ρ=0.6, P<0.05; respectively). In moderate-severe MR, PS B-A showed a strong positive correlation with age (r=0.876, P<0.05).Discussion
A very recent study by K. Pola et al. demonstrated the ratio of HDF as a potential biomarker for identifying patients with heart failure (HF)6. Another study by M. Per et al. showed the ability of HDF to discriminate between controls and patients with HF and preserved ejection fraction (pEF)7. Similarly, our study revealed a significant difference in HDF between controls and patients through a sex-matched analysis (P<0.05). Our study only focused on HDF without exploring HDF ratios. Therefore, future work should investigate ratio effects. The study by M. Per et al. showed no correlation between EF and HDF. However, our study demonstrated a strong negative correlation between LVMI and E-W I-A in mild-moderate MR (P<0.05). This gives strong evidence for our aim as LVMI is a vital biomarker for evaluating VHD8,9. Prior studies showed that age is a powerful predictor of VHD, and the severity increases as people age10. Our study found that age is negatively correlated with E-W I-A and positively correlated with PS B-A in mild-moderate and moderate-severe MR, respectively (P<0.05). Moreover, the substantial variations in HDF across different degrees of MR underscore its capacity to discern MR severity.Conclusion
This study revealed that MR exhibits significantly altered HDF compared to controls, substantial sex-matched variations, and correlation with age across different MR severities. The findings of this study propose HDF (particularly PS B-A, E-W I-A, E-W B-A, and PD S-L) as a potential biomarker for evaluating the severity of MR.Acknowledgements
The authors thank all investigators, clinical staff, and patient participants of the Cardiovascular Imaging Registry of Calgary (CIROC) for their valuable contributions.References
1. Enriquez-Sarano, M., Akins, C. W. & Vahanian, A. Mitral regurgitation. The Lancet 373, 1382–1394.
2. Geeraert, P. et al. Four-Dimensional Flow Magnetic Resonance Imaging and Applications in Cardiology. www.intechopen.com.
3. Loke, Y. H. et al. Abnormal Diastolic Hemodynamic Forces: A Link Between Right Ventricular Wall Motion, Intracardiac Flow, and Pulmonary Regurgitation in Repaired Tetralogy of Fallot. Front Cardiovasc Med 9, (2022).
4. Laenens, D. et al. Introduction to hemodynamic forces by echocardiography. Int J Cardiol 370, 442–444 (2023).
5. Töger, J. et al. Hemodynamic forces in the left and right ventricles of the human heart using 4D flow magnetic resonance imaging: Phantom validation, reproducibility, sensitivity to respiratory gating and free analysis software. PLoS One 13, (2018).
6. Pola, K. et al. Hemodynamic forces from 4D flow magnetic resonance imaging predict left ventricular remodeling following cardiac resynchronization therapy. Journal of Cardiovascular Magnetic Resonance 25, (2023).
7. Arvidsson, P. M. et al. Hemodynamic force analysis is not ready for clinical trials on HFpEF. Sci Rep 12, (2022).
8. Stein, E. J. et al. Left Ventricular Hypertrophy and Biomarkers of Cardiac Damage and Stress in Aortic Stenosis. J Am Heart Assoc 11, (2022).
9. Song, B. G. et al. Preoperative N-terminal pro-B type natriuretic peptide level can predict the regression of left ventricular mass after valvular surgery in patients with chronic severe mitral regurgitation: One-year follow-up. Int J Cardiol 145, 203–208 (2010).
10. Levy, D. Left Ventricular Hypertrophy Epidemiological Insights from the Framingham Heart Study. Drugs (1988).
Figures
Average left ventricular hemodynamic forces over a fraction of the cardiac cycle between sex-matched controls and MR patients (male = A-C, female = D-F).
Indicator Circles: Green = early systole; Red = early diastole; Blue = late systole; Yellow = late diastole.
Indicator Lines: Blue = septal-lateral; Green = inferior-anterior; Red = base-apex; Orange = positive-negative standard deviation (SD).
Abbreviations: MR = mitral regurgitation; S-L = septal-lateral; I-A = inferior-anterior; B-A = base-apex.
Box
plots illustrate the differences in significantly correlated LV functions and HDFs among MR severity levels. (A) LV functions:
LVEDVI and LVEDV; (B) LV functions: LVMI and LVM; (C) HDFs (PS B-A, E-W
I-A, E-W B-A, PD S-L).
Abbreviations: LV = left ventricle; LVEDVI = left ventricle end-diastolic volume indexed; LVEDV = left ventricle end-diastolic volume; LVMI = left ventricle mass indexed; LVM = left ventricle mass; HDF = hemodynamic force; PS B-A = peak systolic base-apex; E-W I-A = E-wave inferior-anterior; E-W B-A = E-wave base-apex; PD S-L = peak diastolic septal-lateral.
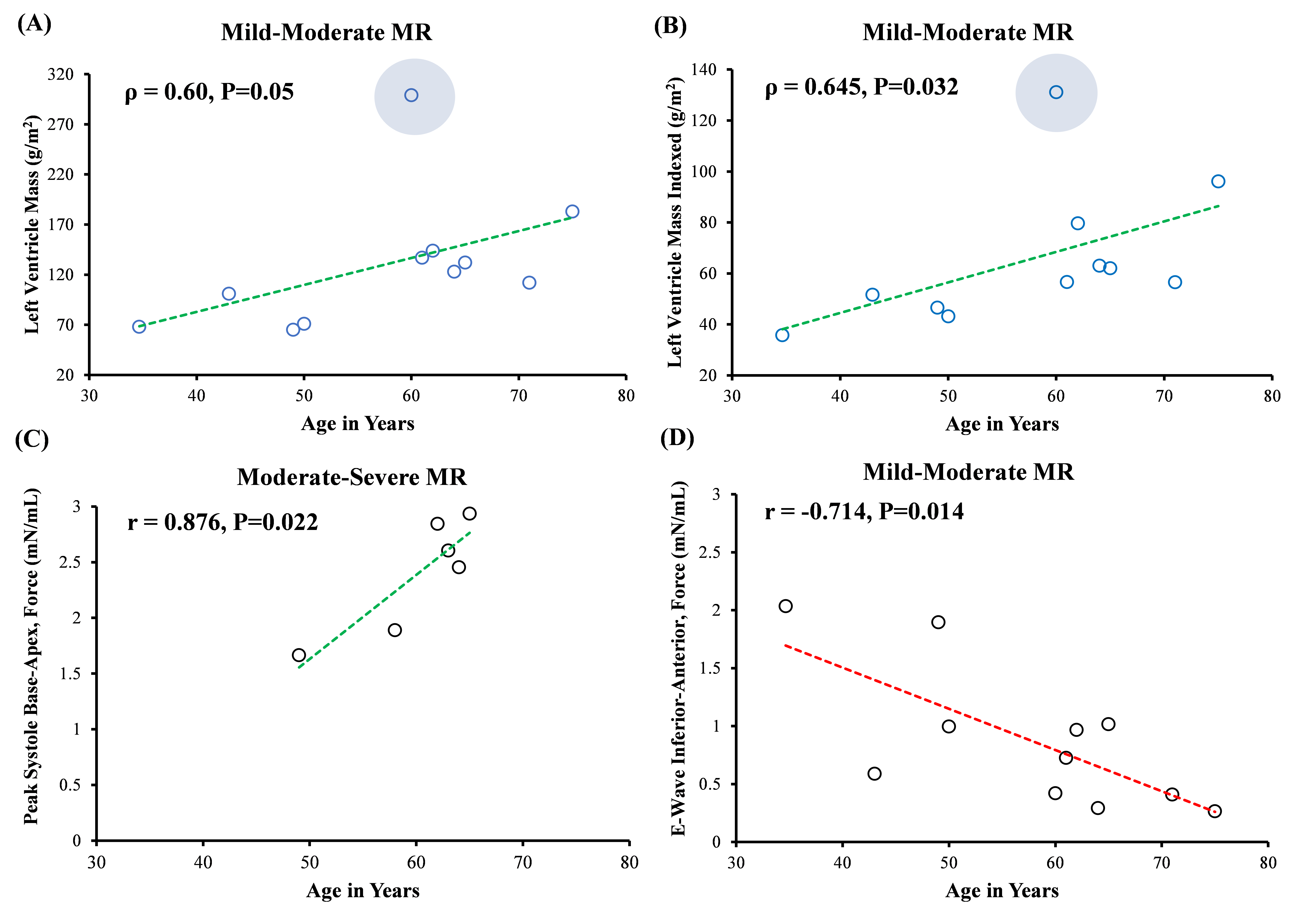
Scatter plots illustrate the correlation between A) Age and LVM in mild-moderate MR; B) Age and LVMI in mild-moderate MR; C) Age and PS B-A in moderate-severe MR; D) Age and E-W I-A in mild-moderate MR.
Notes: The Blue shaded circle indicates the outlier. Correlation coefficient: Pearson's = r; Spearman's = ρ. P<0.05 was considered statistically significant.
Linear Correlation: Green = positive; Red = negative.
Abbreviations: LV = left ventricle; HDF = hemodynamic force; PS B-A = peak systolic base-apex; E-W I-A = E-wave inferior-anterior; LVM = left ventricle mass; LVMI = LVM index.