0095
Differentiating Pulmonary Hypertension Groups by 3D Vortex-contained energetics from 4D Flow MRI and Correlation with Right Heart Function1Radiology, Northwestern University, Chicago, IL, United States, 2Cardiology, Northwestern University, Chicago, IL, United States
Synopsis
Keywords: Flow, Cardiovascular, Pulmonary Hypertention
Motivation: There is a lack of noninvasive methods to differentiate between different Pulmonary Hypertension Groups/types. Such differentiation is clinically critical because treatments of one group can be harmful to another.
Goal(s): We investigated a new noninvasive 4D Flow MRI-based method to differentiate between Pulmonary Arterial Hypertension (PAH) and Pulmonary Venous Hypertension (PVH), currently distinguished conclusively only through invasive catheterization.
Approach: Our study focused on analyzing 3D vortex flow and its energetics in the left pulmonary artery (LPA) using 4D Flow MRI.
Results: We found significant differences in vortex characteristics between PVH and PAH patients, with PVH showing larger vortex cores and higher energetics.
Impact: These findings suggest the potential of LPA vortex flow analysis as a noninvasive diagnostic marker for distinguishing between PAH and PVH and possibly assessing disease severity.
Purpose:
Pulmonary hypertension (PH) is a life-threatening condition with elevated blood pressure in the main pulmonary artery. It is crucial to differentiate between two types: Pulmonary Arterial Hypertension (PAH; WHO Group 1) and Pulmonary Venous Hypertension (PVH; WHO Group 2) because PAH treatments can be harmful to PVH patients [1]. Invasive right heart CATH pressure remains the only method for conclusive diagnosis based on the elevation of pulmonary capillary wedge pressure (PCWP) [1]. Previous 4D Flow studies focused on the main pulmonary artery (MPA) flow found differences between PH patients and controls but could not distinguish between PAH and PVH groups [2, 3]. Here, we aim to differentiate these two groups by quantifying advanced flow changes in the left pulmonary artery (LPA) instead of MPA. Our hypothesis is that given that PCWP is wedged by Cath from the LPA, PCWP pressure changes would alter vortex flow dynamics and its vortex-contained energetics of kinetic energy (KE) and viscous energy loss (EL) – in the LPA. We further hypothesize that such LPA vortex flow changes would correlate with right heart (dys)function characterized by right ventricular (RV) stroke volume (RVSV) and ejection fraction (RVEF).Methods:
We retrospectively evaluated a total of 33 patients, including 22 PVH patients (age: 59.60 ± 12.20 yrs, 11 female) and 11 PAH patients (age: 52.00 ± 10.88 yrs, 9 female) who underwent whole-heart 4D Flow MRI Table.1. PVH and PAH patients were diagnosed based on invasive right heart Cath pressures per guidelines [1]. Our analysis methodology is illustrated in Fig.1. In short, 4D Flow MRI-derived 3D PC angiogram was computed and used to segment the 3D LPA. Using the lambda2 method, the largest instantaneous 3D vortex core in the segmented LPA was identified mathematically over each of the systolic time frames as previously described [4] – see vortex cores in Fig.1. The peak vortex volume over the systole was calculated. Next, we computed the total sum of kinetic energy (KE) and viscous energy loss (EL) within each vortex for each time frame [5]. We then determined the peak vortex-contained KE (vortex KE) and vortex-contained EL (vortex EL) over the systolic time frames. Additionally, we evaluated the correlation to right heart function, as quantified by RVSV and RVEF from standard cine short-axis MR images.Results:
The PVH patients group showed significantly higher LPA 3D vortex volume (p=0.03), and vortex flow-contained energetics including vortex KE (p=0.04), and vortex EL (p=0.02) compared to PAH patients group (Fig2,3). In PAH patients, there were high correlations in LPA vortex flow-contained energetics with right heart function as characterized by correlations of vortex KE with RVSV (Spearman rho=0.86; p<0.01), Vortex EL with RVSV (rho=0.80; p<0.01), vortex KE with RVEF (rho=0.67; p=0.02), vortex EL with RVEF (rho=0.61; p=0.05) (Fig4.a). Likewise, PVH patients showed significant correlations in vortex EL with RVSV (rho=0.70; p<0.01), as well as vortex KE with RVSV (rho=0.55; p<0.01) (Fig4.b).Discussion and conclusions:
The results of this study demonstrate significant differences in LPA 3D vortex characteristics between PVH and PAH patients. PVH patients have a larger vortex core and vortex-contained energetics of KE and EL in their LPA compared to PAH patients. This suggests that altered vortex flow dynamics in the LPA may help differentiate between PAH and PVH groups. These results are promising since prior 4D Flow studies that focused on MPA flow were unable to differentiate between the two groups [2, 3]. The study suggests that it is the vortex flow in the LPA that may be differentiated, which could be a result of the PCWP changes. Currently, only invasive Cath can conclusively differentiate the two groups, but these results suggest a promising noninvasive technique to differentiate the two PH groups. Notably, there were correlations of vortex flow energetics to RV stroke volume and RV ejection fraction in both PAH and PVH patients. This suggests that alterations in vortex flow energetics may not only be a differentiator but might also allow quantifying flow changes associated with right heart function deterioration in these patients. This may help assess the severity of the disease. Larger cohort studies are warranted to validate these findings, suggesting that a 3D vortex flow energetics within the LPA could be used as a novel noninvasive diagnostic marker for distinguishing between PAH and PVH, and possibly assessing disease severity.Acknowledgements
No acknowledgement found.References
[1] Galiè N, Humbert M, Vachiery J-L, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). European heart journal. 2015;37:67-119.
[2] Reiter G, Reiter U, Kovacs G, Olschewski H, Fuchsjäger M. Blood flow vortices along the main pulmonary artery measured with MR imaging for diagnosis of pulmonary hypertension. Radiology. 2015;275:71-79.
[3] Cerne JW, Pathrose A, Gordon DZ, Sarnari R, Veer M, Blaisdell J, Allen BD, Avery R, Markl M, Ragin A. Evaluation of pulmonary hypertension using 4D flow MRI. Journal of Magnetic Resonance Imaging. 2022;56:234-245.
[4] Elbaz MS, Calkoen EE, Westenberg JJ, Lelieveldt BP, Roest AA, van der Geest RJ. Vortex flow during early and late left ventricular filling in normal subjects: quantitative characterization using retrospectively-gated 4D flow cardiovascular magnetic resonance and three-dimensional vortex core analysis. Journal of Cardiovascular Magnetic Resonance. 2014;16:78.
[5] Elbaz MS, van der Geest RJ, Calkoen EE, de Roos A, Lelieveldt BP, Roest AA, Westenberg JJ. Assessment of viscous energy loss and the association with three‐dimensional vortex ring formation in left ventricular inflow: In vivo evaluation using four‐dimensional flow MRI. Magnetic resonance in medicine. 2017;77:794-805.
Figures
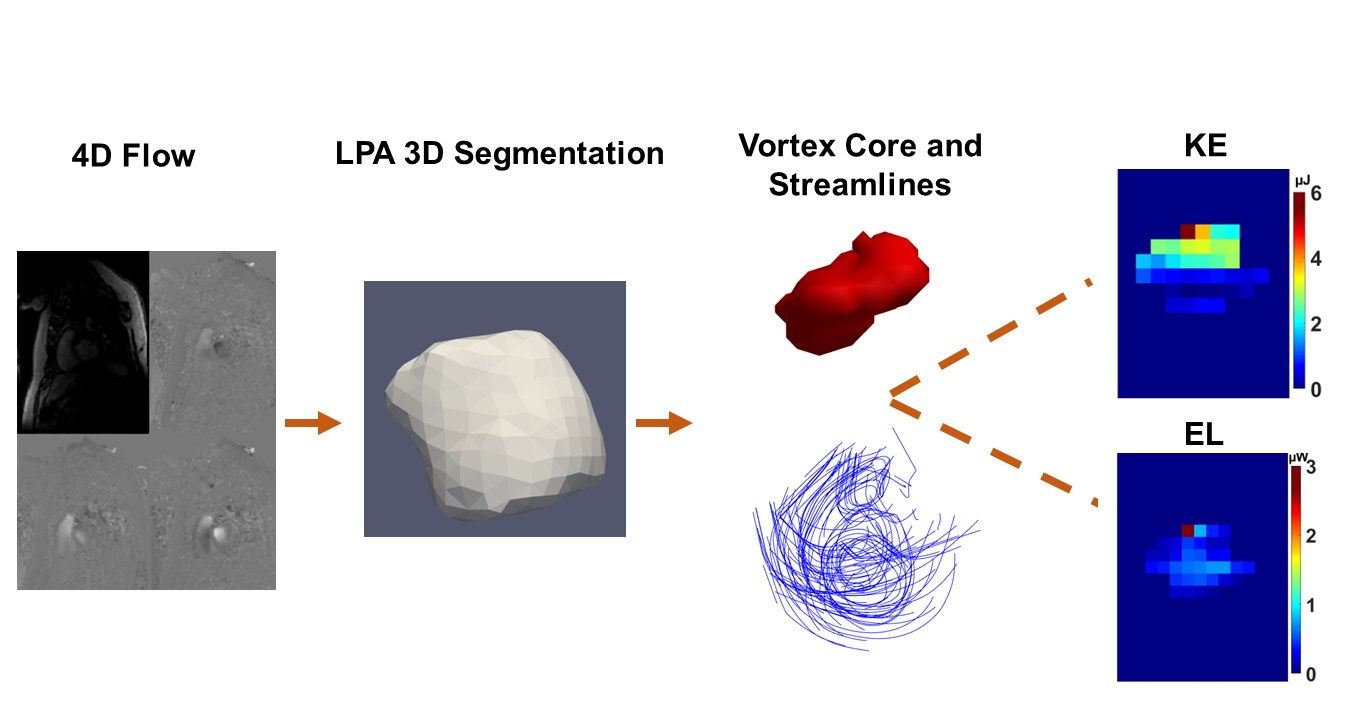
Fig.1 indicates the steps from 4D flow images to segment the left pulmonary artery (LPA) and calculate the vortex core and related streamlines by lambda 2 method.
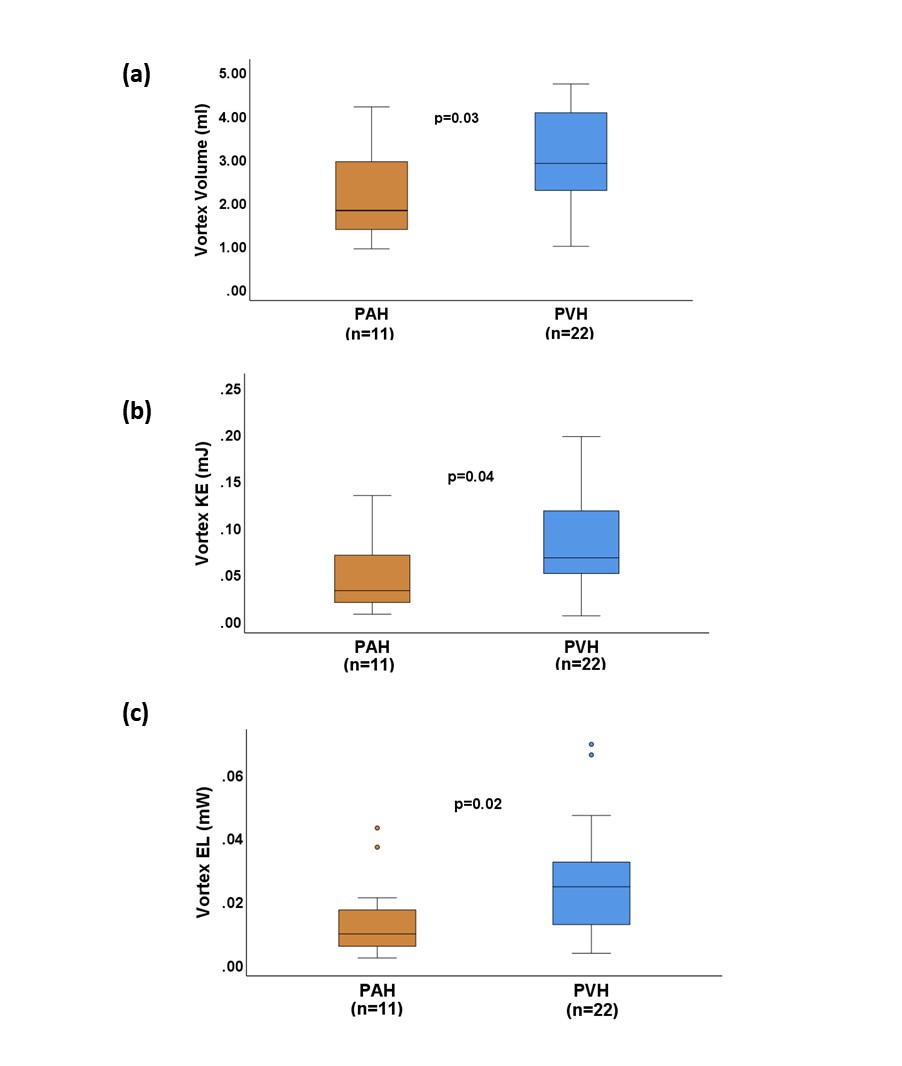
Fig.2 Summarized vortex characteristics comparison between two groups of Pulmonary Arterial Hypertension (PAH) and Pulmonary Venous Hypertension (PVH), (a) indicated that the vortex volume is higher in PVH (b) showed that vortex kinetic energy (KE) is more in PVH group and (c) showed the vortex energy loss (EL) is also higher in PVH.
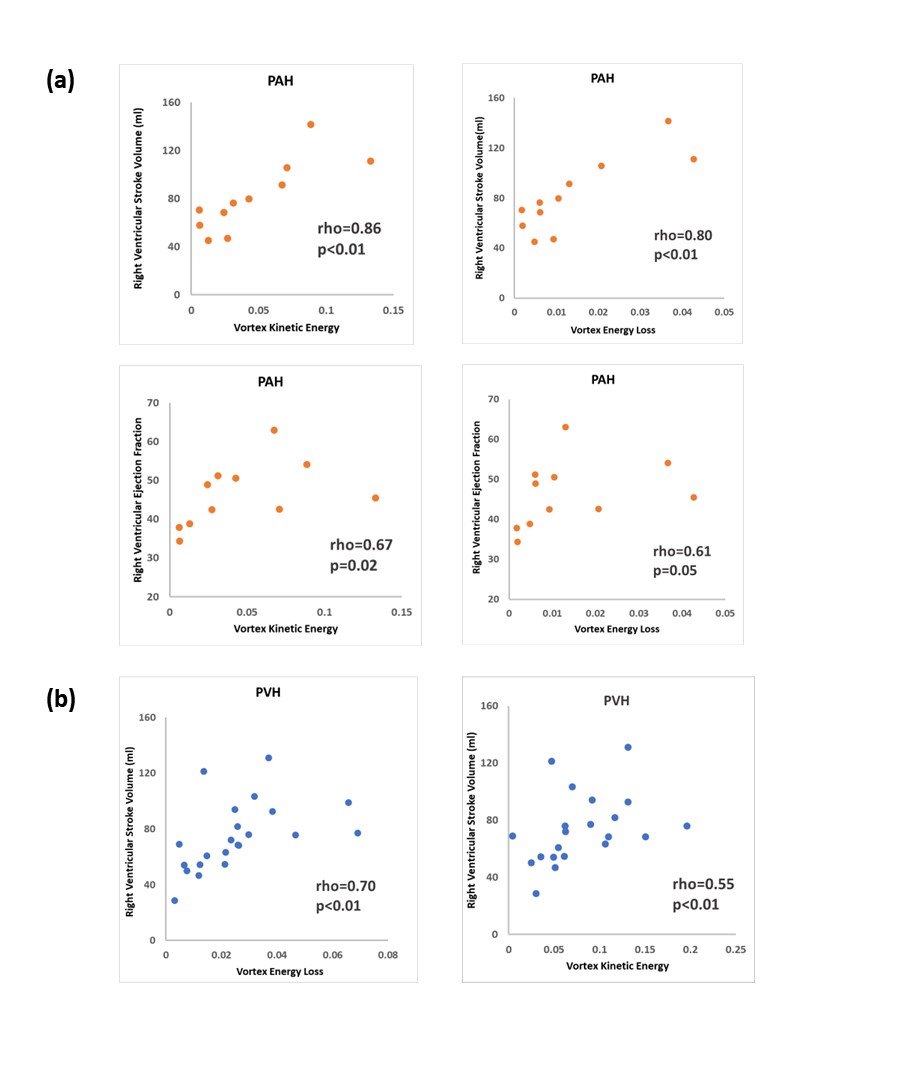
Fig.4 (a) showed a positive correlation in LPA vortex flow-contained energetics such as KE and EL with right ventricular stroke volume (RVSV) and right ventricular ejection fraction (EF) in PAH patients, (b) indicated PVH group has significant correlations in their vortex EL with RVSV, as well as vortex KE with RVSV.
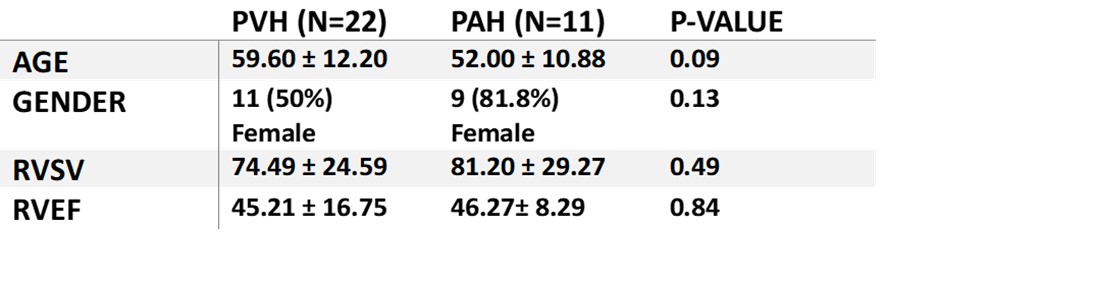
Table.1 Characteristic data