0094
Free-running fat-suppressed radial whole-heart 4D flow using OptiPulse1Department of Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Switzerland, Lausanne, Switzerland, 2Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, Lausanne, Switzerland, 3Department of Radiology, Northwestern University, Feinberg School of Medicine, Chicago, IL, USA, Chicago, IL, United States
Synopsis
Keywords: Flow, Heart, Flow, Fat, Whole-heart, Congenital Heart Disease
Motivation: Free-running radial 4D flow has been shown to enable accurate whole-heart quantification and visualization of hemodynamics. However, unsuppressed fat signal can lead to artifacts, which may compromise image quality and cause errors in flow quantification.
Goal(s): Our study therefore aims to reduce fat signal in radial 4D flow MRI.
Approach: We integrated a novel b-splines iteratively optimized water-excitation RF pulse generated with a previously described framework (OptiPulse) into a radial 4D flow sequence to suppress the signal from fat.
Results: We successfully integrated OptiPulse in radial 4D flow to suppress fat signal and demonstrated comparable quantitative flow assessment to non-fat-suppressed 4D flow.
Impact: The integration of b-splines iteratively optimized water-excitation RF pulses (OptiPulse) into a free-running radial whole-heart 4D flow sequence leads to significantly reduced fat-signal in a promising step towards more robust hemodynamic assessment in patients with large amounts of adipose tissue.
Introduction
4D flow MRI enables dynamic quantification and visualization of hemodynamics, making it a useful complement to Doppler ultrasound and 2D flow MRI in diseases that affect the cardiovascular system [1]. However, in patients with large amounts of adipose tissue, image quality can suffer due to ghosting or streaking artifacts that may lead to flow quantification errors [2]. Various strategies have been developed to address these challenges, including spatial selective excitations [3], multi-echo fat-water separation [4], and intermittent fat saturation [2]. Recently, a novel numerical optimization framework, known as OptiPulse, was introduced for generating spectrally selective water excitation (WE) RF pulses [5]. OptiPulse offers significant improvements by optimizing pulse shapes in a high-dimensional parameter space. In this study, we integrated an optimized b-spline interpolated pulse created with OptiPulse into a previously established free-running radial whole-heart flow acquisition [6] with respiratory motion-corrected reconstruction [7]. Our aim was to demonstrate the feasibility of combining OptiPulse with radial 4D flow for reducing fat signal and obtaining precise measurements of net volume and peak flow in a cohort of healthy volunteers. We compared this method to previously reported approaches for free-running radial 4D flow [7] and respiratory-navigated Cartesian 4D flow [2].Methods
A previously described free-running 3D radial phase-contrast MRI sequence was modified by replacing the 0.3ms slab-selective half-sinc RF pulses [Figure 1] with a 2.5ms non-selective WE pulse that has been optimized to have a broad suppression bandwidth rendering it less sensitive to B0 inhomogeneities [5]. Five healthy volunteers (2 male, ages 25-39 years, BMI of 20.3 to 32.5) were scanned on a 1.5T clinical MRI (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany). All subjects provided written informed consent compliant with our institutional guidelines and approved by the local research ethics committee. For each volunteer, three sequences were acquired: the previously described free-running radial flow [6,7] which we refer to hereafter as radial 4D flow, the proposed free-running radial OptiPulse flow variant (radial Opti 4D flow), and respiratory navigator-gated Cartesian 4D flow (Cartesian 4D flow) for reference. Scan parameters are provided in Table 1. All scans were performed free-breathing, and a pulse oximeter signal was recorded throughout the scan for retrospective cardiac gating. Both radial sequences were reconstructed using focused navigation for respiratory motion correction and compressed sensing [7]. To assess the performance of the proposed fat suppression, the fat-to-blood contrast ratio was calculated by CR = Sfat/Sblood with Sfat, Sblood being the averaged magnitude of the complex signal within a manually selected ROI in the chest and in the heart. The CR was compared between the two radial sequences. Statistical analysis of all contrast-ratio measurements was performed using a paired Student’s t-test. All three sequences were additionally analyzed by measuring flow curves using Circle cvi42 (Calgary, Canada). For each volunteer and dataset, 2D planes in the ascending aorta (AAo), descending aorta (DAo), and main pulmonary artery (MPA) were manually chosen for calculation of net volume and peak flow. The agreement between the 3 sequences was assessed by Pearson correlation coefficients and Bland-Altman analysis.Results
The proposed integration of OptiPulse and free-running radial 4D flow shows a clear reduction in fat signal when compared to the previously published method [Figure 1].For the assessment of fat suppression, the fat-to-blood contrast ratio (CR) was 2.87±0.61 for the radial 4D flow and 0.52±0.20 for the radial Opti 4D flow (P=0.0009). Overall, we found moderate to strong correlation [Figure 2] when comparing reference Cartesian 4D flow measurements of net-volume and peak flow to radial 4D flow with (rnet-volume=0.8, rpeak-flow=0.8) and without OptiPulse (rnet-volume=0.78, rpeak-flow=0.82). We did note a slightly better correlation when comparing the two radial sequences to each other (rnet-volume=0.83, rpeak-flow=0.86). However, we found significant biases with relatively large limits of agreement when comparing the three techniques [Figure 3]. Streamline analysis was comparable between the three sequences [Figure 4].
Discussion and Conclusion
In this preliminary study, we successfully integrated fat suppression with an optimized water excitation-pulse (OptiPulse) into a free-running radial whole-heart 4D flow sequence. This integration achieved clear reduction of fat signal in the chest wall region without significantly affecting blood flow measurements in healthy subjects. These promising initial results warrant further study in a flow phantom, a larger cohort of healthy volunteers to better define the limits of agreement, and a cohort of obese subjects, where the amount of streaking artifact generated by adipose tissue is likely to significantly deteriorate the diagnostic quality of the cardiac flow assessment. In this way we will be able to assess the importance of fat suppression and show the impact of the proposed technique.Acknowledgements
Christopher Roy is the PI on Swiss National Science Foundation Grant PZ00P3_202140 that funded part of this research. Matthias Stuber is the PI on the Swiss National Science Foundation Grants 320030_173129 and 201292 that funded part of this research.References
[1] Bissell, M.M., Raimondi, F., Ait Ali, L. et al. 4D Flow cardiovascular magnetic resonance consensus statement: 2023 update. J Cardiovasc Magn Reson. 2023 Jun; 25(40).
[2] Shamim AMKM, Panagiotopoulos N, Spahic A, Harris DT, Roldán-Alzate A et. al. Fat mitigation strategies to improve image quality of radial 4D flow MRI in obese subjects. Magn Reason Med. 2023 Apr;90(2).
[3] Feinberg DA, Hoenninger JC, Crooks LE, Kaufman L, Watts JC, Arakawa M. Inner volume MR imaging: technical concepts and their application. Radiology. 1985 Sep;156(3):743-7.
[4] Cheng et al Contrast-Enhanced 4D Flow Imaging with Reduced Fat Signal. ISMRM abstract. 2016; Number:2712.
[5] Sieber X et al. Efficient fat suppression in free-running whole-heart CMR using OptiPulse. ISMRM abstract. 2023; Number:1487.
[6] Ma LE, Yerly J, Piccini D, Di Sopra L, Roy CW, Carr JC, Rigsby CK, Kim D, Stuber M, Markl M. 5D Flow MRI: A Fully Self-gated, Free-running Framework for Cardiac and Respiratory Motion-resolved 3D Hemodynamics. Radiol Cardiothorac Imaging. 2020 Nov;2(6).
[7] Falcão MBL, Rossi GMC, Rutz T, et al. Focused navigation for respiratory–motion-corrected free-running radial 4D flow MRI. Magn Reson Med. 2023 Mar; 90: 117-132.
Figures

Table1: Scan parameters for radial 4D flow and Cartesian 4D flow.
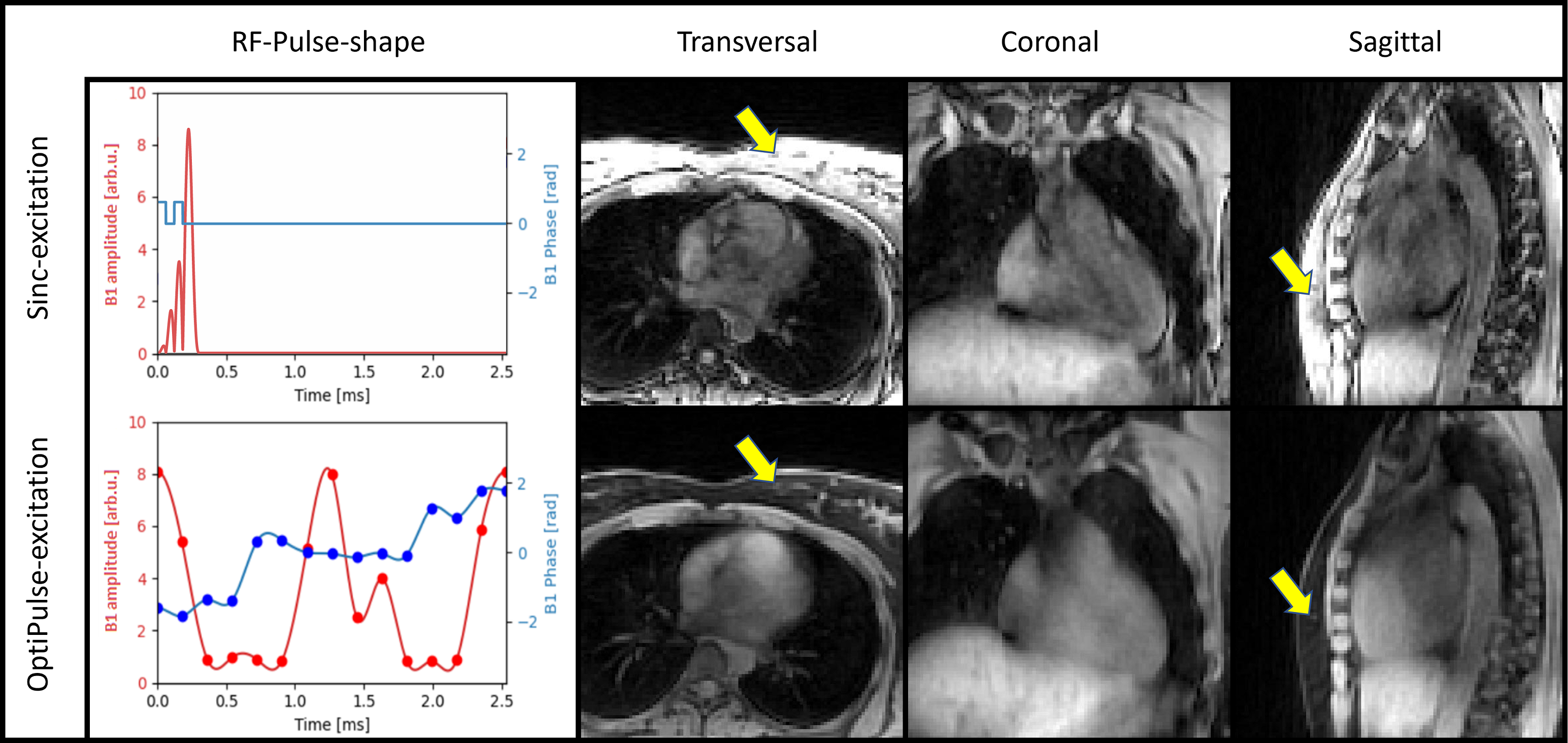
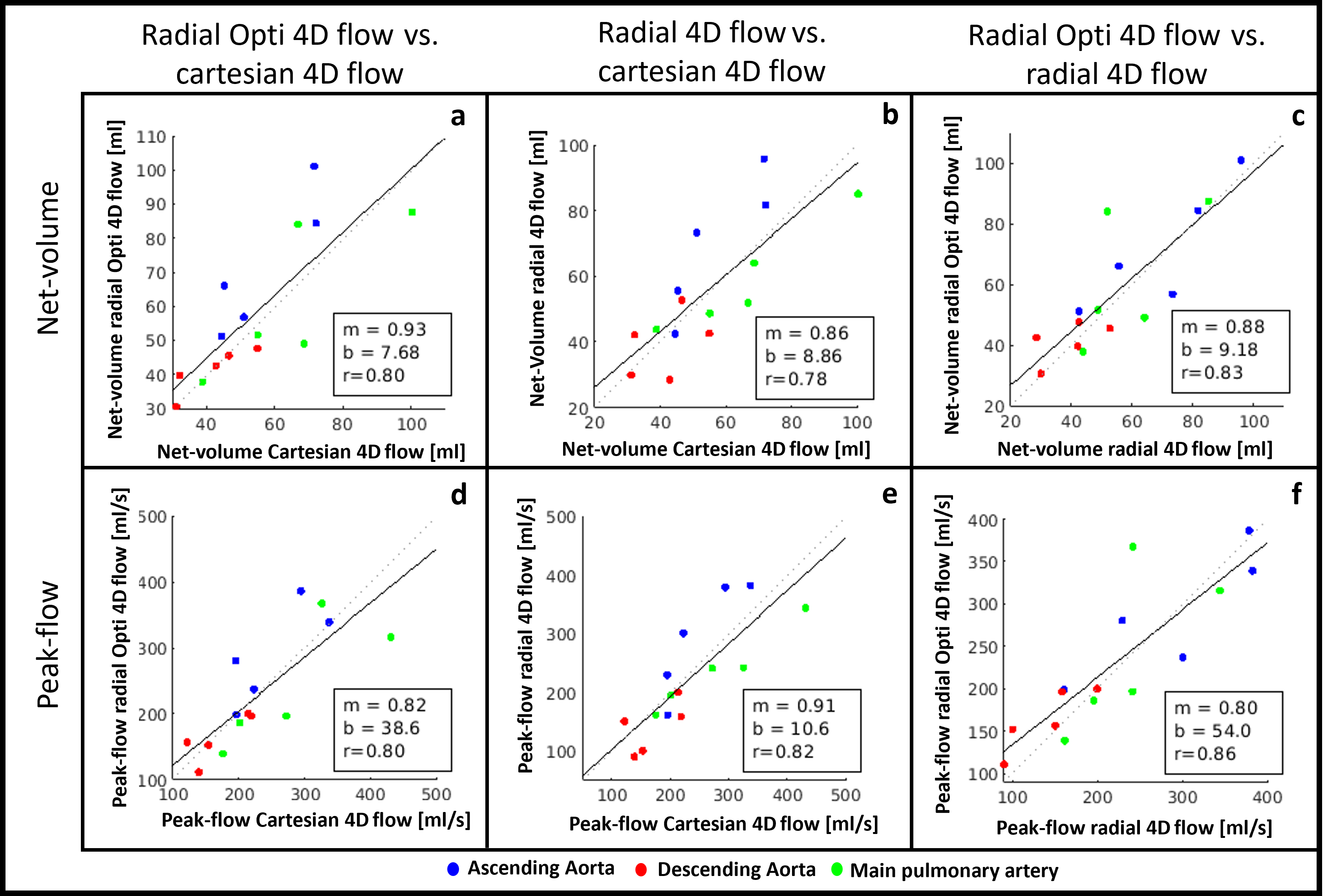
Figure 2: Correlation analysis of net-volume (a,b,c) and peak-flow (d,e,f). With respective flow-sequence comparisons of radial Opti 4D flow vs. Cartesian 4D flow (a,d), radial 4D flow vs. Cartesian 4D flow (b,e) and of radial Opti 4D flow vs. radial 4D flow (c,f), each with its respective linear curve fit (f(y)=m*x+b) and the corresponding Pearson-correlation coefficient r. N=5 measurements (of 5 subjects) have been performed by manually segmenting a perpendicular slice of the ascending aorta (AAo: blue), the descending aorta (DAo: red) and the main pulmonary artery (MPA: green).
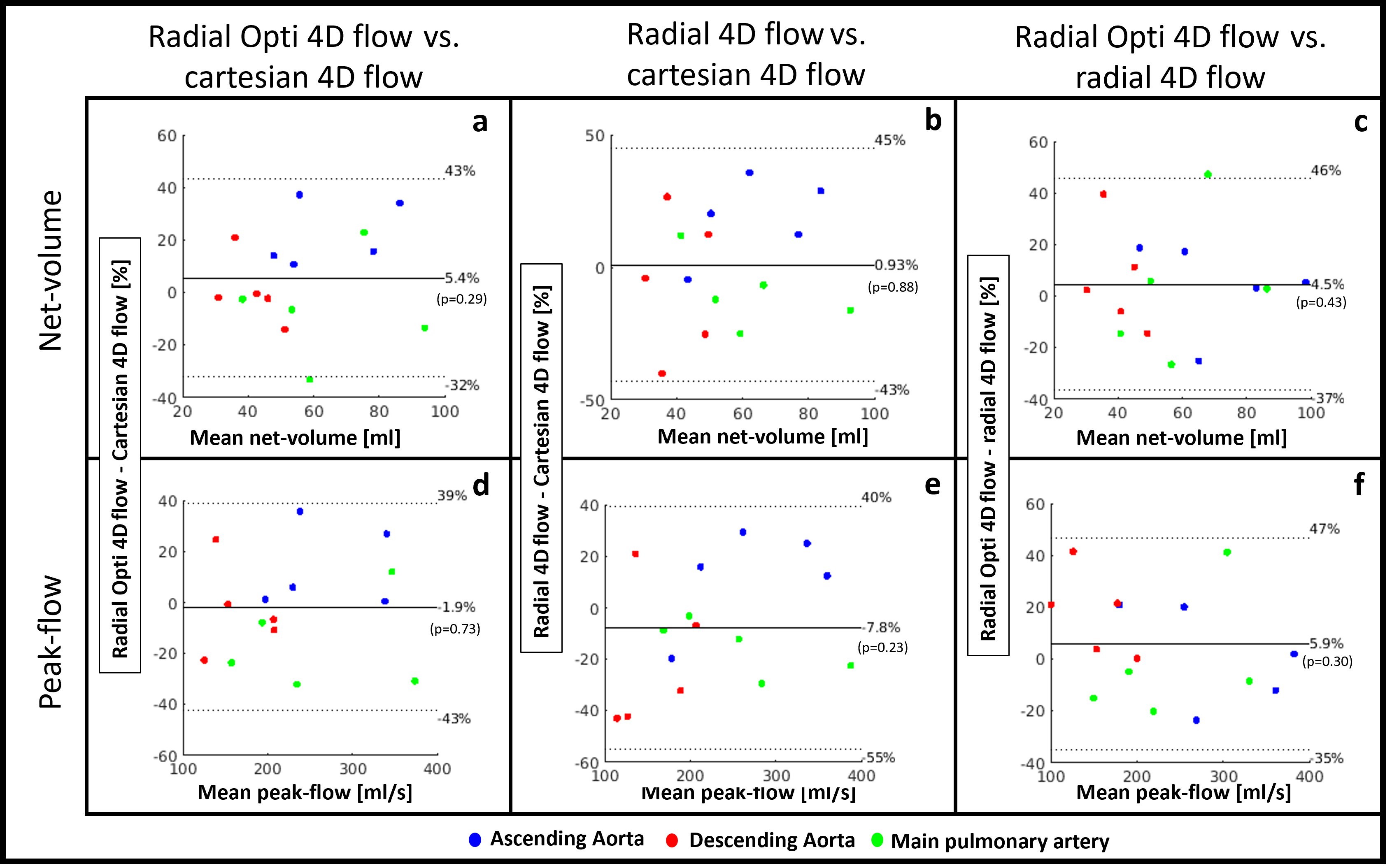
Figure 4: Dynamic visualization of flow streamlines in one subject with Cartesian 4D flow, radial 4D flow and radial Opti 4D flow.