0090
Venous Return in Chronic Obstructive Pulmonary Disease Assessed with 4D Flow MRI1University of Wisconsin-Madison, Madison, WI, United States, 2Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 3Columbia University, New York, NY, United States, 4Johns Hopkins University School of Medicine, Baltimore, MD, United States, 5University of Michigan School of Medicine, Ann Arbor, MI, United States, 6University of California Los Angeles, Los Angeles, CA, United States, 7University of California San Francisco, San Francisco, CA, United States, 8University of Utah School of Medicine, Salt Lake City, UT, United States, 9Wake Forest University, Winston-Salem, NC, United States
Synopsis
Keywords: Heart Failure, Blood vessels, COPD, Hemodynamics, Heart Failure, 4D Flow
Motivation: Chronic obstructive pulmonary disease (COPD) and emphysema are associated with hemodynamic changes in the pulmonary vasculature, possibly related to increased intra-thoracic pressure during expiration, altering venous return into the thorax.
Goal(s): Assess the association of respiratory dysfunction with hemodynamic parameters of venous return.
Approach: Velocity, kinetic energy, and stasis in the superior vena cava and inferior vena cava were quantified with 4D Flow MRI in 72 subjects across the COPD spectrum in an ongoing study (SPIROMICS HF).
Results: Our results show an association of impaired (reduced) venous return to the thorax with airway obstruction as assessed by spirometry.
Impact: This study demonstrates impaired venous return in subjects with COPD, which warrant further investigations into the cardiopulmonary interactions of right heart flow in COPD and its potential value as a noninvasive marker of disease progression.
Introduction
Mortality from chronic obstructive pulmonary disease (COPD) has doubled since the 1960’s1 such that it was the third leading cause of death globally in 2019.2, 3 COPD is an independent risk factor for incident heart failure with preserved ejection fraction (HFpEF)4 and more than a third of patients hospitalized for COPD have HFpEF, and vice versa5; however COPD guidelines barely mention HF and HFpEF guidelines do not mention the lungs.6,7 COPD and HFpEF do not adequately address the complex cardiopulmonary interactions that result in changes to the pulmonary vasculature possibly related to increased intra-thoracic pressure during expiration, which alters venous return into the thorax.4D Flow MRI has emerged as a useful and reliable technique to comprehensively capture dynamic blood velocity vectors in the heart and vessels over a large imaging volume, thus enabling comprehensive, advanced hemodynamic evaluation. Here we use 4D Flow MRI to quantify parameters characterizing venous return to the right heart in participants with COPD and controls.
Methods
The SubPopulations and InteRmediate Outcome Measures In COPD and Heart Failure Study (SPIROMICS HF) is a prospective cohort study that has acquired cardiac MRIs in over 600 subjects across multiple centers. 4D Flow MRI datasets were acquired and analyzed at central reading centers within a subset of the SPIROMICS HF study with analysis in more subjects ongoing. 4D Flow data was processed following established guidelines8 including background phase corrections, noise corrections, and velocity anti-aliasing (Figure 1). A 3D PC angiogram was generated from the 4D Flow data (magnitude and phase) and used to manually segment the brachiocephalic veins and the superior vena cava (SVC) as well as the hepatic veins and the inferior vena cava (IVC) using Mimics Innovation Suite 20.0 (Materialize, Leuven, Belgium). The manual segmentations were then applied to an algorithm to quantify SVC and IVC hemodynamic parameters: mean and maximum velocity, mean stasis (percent of the cardiac cycle with blood velocity <0.1m/s), and kinetic energy (velocity squared times the density of a voxel and ultimately summed up over the volume of interest with density of blood as ρ=1060 kg/m3) (Figure 2). Respiratory function was assessed via spirometry: forced expiratory volume in one second (FEV1) and forced vital capacity of the lung (FVC). Multivariable regression was used to examine associations between the independent exposures adjusted for age, sex, race/ethnicity, and height.Results
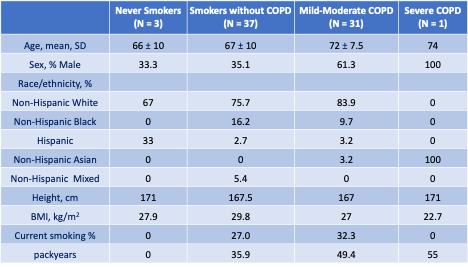
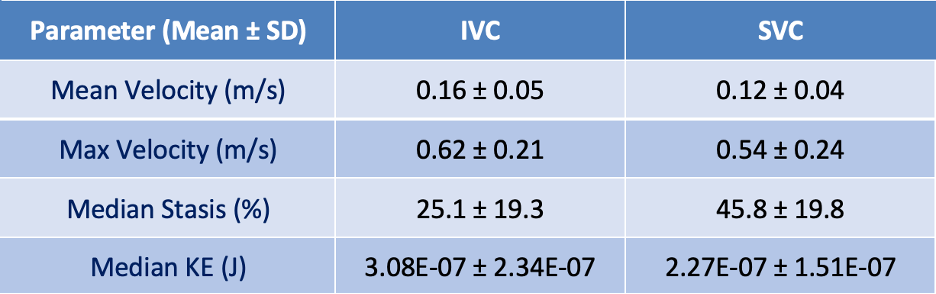
72 participants were included (age: 70±9yrs, 38 female) with available measures to date (Table 1) and grouped according to Global Initiative for Obstructive Lung Disease (GOLD) criteria: COPD (FEV1/FVC<0.7, n=32), mild-moderate (FEV1 50-80%, n=31) severe (FEV1<50%, n=1), 37 controls (FEV1/FVC≥0.70) with a smoking history, and 3 controls without a smoking history.Figure 3 shows a representative example (participant A) of 4D flow IVC data with normal, efficient flow characterized by low stasis values, high mean velocity, and high kinetic energy compared to the average values of our cohort (Table 2). Participant B presents with poor, impaired flow where opposite trends are observed.
FEV1/FVC ratio was correlated with maximum and mean velocity of IVC blood flow (r=0.39, p=0.04 and r=0.48, p=0.01 respectively) and kinetic energy of IVC blood flow (r=0.46, p=0.01). FEV1/FVC ratio was also negatively correlated with stasis of blood in the IVC (r= -0.38, p=0.05). Similar trends were found for the SVC and FEV1/FVC but were not statistically significant.
Discussion
Previous work has found impaired left ventricular filling in COPD and emphysema9. Additionally, pulmonary vascular changes have been linked to this impaired filling suggesting an upstream mechanism affecting cardiac function.10,11 Our results show that a lower FEV1/FVC ratio is associated with an impairment in venous return into the thorax where we observed lower peak velocities, lower kinetic energy, and higher stasis in the IVC. We found that respiratory dysfunction is associated with slower velocities and increased stasis in the IVC, trending similarly in the SVC, which is consistent with reports suggesting that COPD affects upstream blood flow and alters venous return into the thorax. Currently, the sample size is relatively small for each subgroup, particularly for patients with severe COPD, which underpowers the statistical significances of some of our observed trends. Sample size will be improved with further data inclusion. Our findings warrant further investigations into the cardiopulmonary interactions of right heart flow in COPD and comparisons with invasive catheter-based methods for central venous pressure.Acknowledgements
Funding: NIH/NHLBI R01-HL093081 and R01-HL121270. SPIROMICS was supported by contracts from the NIH/NHLBI (HHSN268200900013C, HHSN268200900014C, HHSN268200900015C, HHSN268200900016C, HHSN268200900017C, HHSN268200900018C, HHSN268200900019C, HHSN268200900020C), which were supplemented by contributions made through the Foundation for the NIH from AstraZeneca; Bellerophon Therapeutics; Boehringer-Ingelheim Pharmaceuticals, Inc; Chiesi Farmaceutici SpA; Forest Research Institute, Inc; GSK; Grifols Therapeutics, Inc; Ikaria Inc; Nycomed GmbH; Takeda Pharmaceutical Company; Novartis Pharmaceuticals Corporation; Regeneron Pharmaceuticals, Inc; and Sanofi."References
- Health Statistics US. 2016. Extracted from CDC data, August, 2018.
- WHO. Cuase-specific mortality, 2000-2019. Global health estimates: Leading causes of death. 2020.
- Heron M. Deaths: Leading Causes for 2019. Natl Vital Stat Rep. 2021;70:1-114.
- Eckhardt, C. M., Balte, P. P., Barr, R. G., Bertoni, A. G., Bhatt, S. P., Cuttica, M., Cassane, P. A., Chaves, P., Couper, D., Jacobs, D. R., Kalhan, R., Kronmal, R., Lange, L., Loehr, L., London, S. J., O’connor, G. T., Rosamond, W., Sander, J., Schwartz, J. E., … Oelsner, E. C. (2022). Lung function impairment and risk of incident heart failure: the NHLBI Pooled Cohorts Study. European heart journal, 43(23), 2196-2208.
- Iversen KK, Kjaergaard J, Akkan D, Kober L, Torp-Pedersen C, Hassager C, Vestbo J, Kjoller E and Group ELFS. The prognostic importance of lung function in patients admitted with heart failure. European Journal of Heart Failure. 2010;12:685-691.
- Venkatesan P. GOLD report: 2023 update. https://goldcopd.org/2023-gold-report-2/
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr., Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, Hollenberg SM, Lindenfeld J, Masoudi FA, McBride PE, Peterson PN, Stevenson LW and Westlake C. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70:776-803.
- Dyverfeldt P, Bissell M, Barker AJ, Bolger AF, Carlhäll CJ, Ebbers T, Francios CJ, Frydrychowicz A, Geiger J, Giese D, Hope MD, Kilner PJ, Kozerke S, Myerson S, Neubauer S, Wieben O, Markl M. 4D flow cardiovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson. 2015 Aug 10;17(1):72.
- Smith, B. M., Prince, M. R., Hoffman, E. A., Bluemke, D. A., Liu, C. Y., Rabinowitz, D., ... & Barr, R. G. (2013). Impaired left ventricular filling in COPD and emphysema: is it the heart or the lungs?: the multi-ethnic study of atherosclerosis COPD study. Chest, 144(4), 1143-1151.
- Aaron, C. P., Hoffman, E. A., Lima, J. A., Kawut, S. M., Bertoni, A. G., Vogel-Claussen, J., ... & Barr, R. G. (2017). Pulmonary vascular volume, impaired left ventricular filling and dyspnea: The MESA Lung Study. PloS one, 12(4), e0176180.
- Barr, R. G., Bluemke, D. A., Ahmed, F. S., Carr, J. J., Enright, P. L., Hoffman, E. A., ... & Watson, K. E. (2010). Percent emphysema, airflow obstruction, and impaired left ventricular filling. New England Journal of Medicine, 362(3), 217-227.
Figures
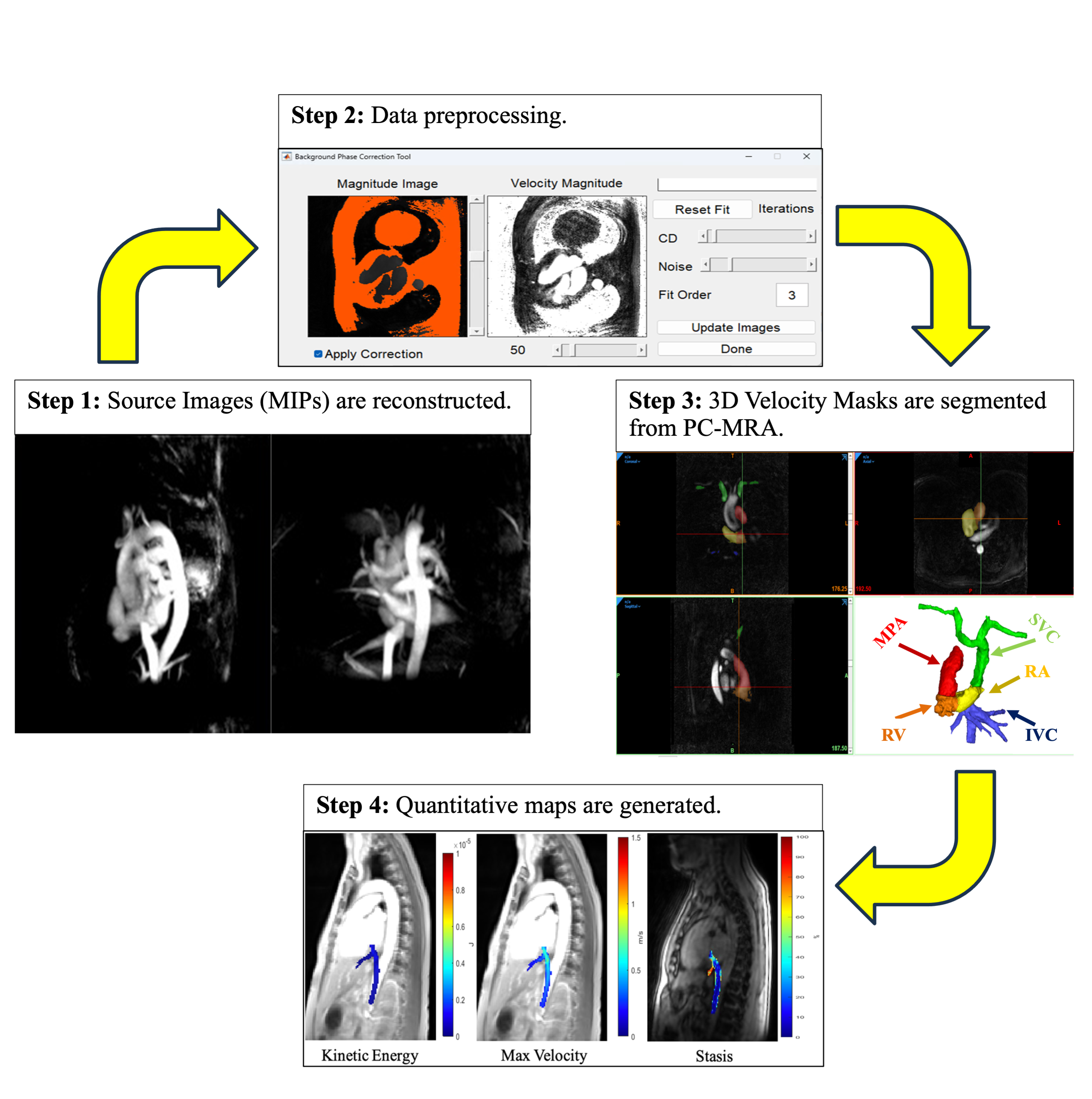
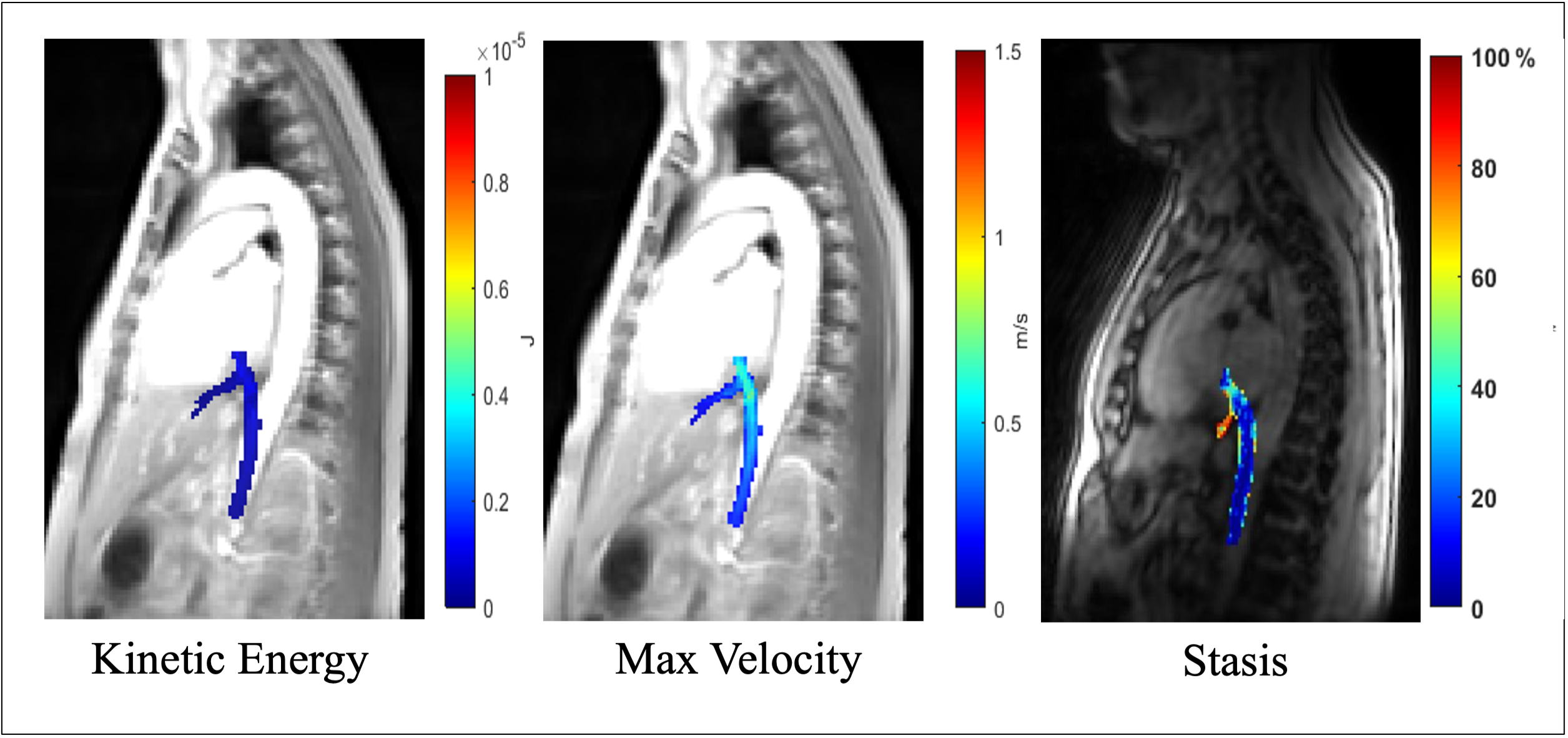
Figure 2: Representative results of kinetic energy, maximum velocity, and stasis in the inferior vena cava illustrated by quantitative colormaps of the 3D segmented regions superimposed onto the corresponding reformatted anatomical images. Kinetic energy is given in terms of Joules (J), or equivalently kg⋅m2⋅s−2. Velocity is given in meters/second (m/s). Blood stasis values are given in terms of % of the cardiac cycle in which velocity < 0.1 m/s.
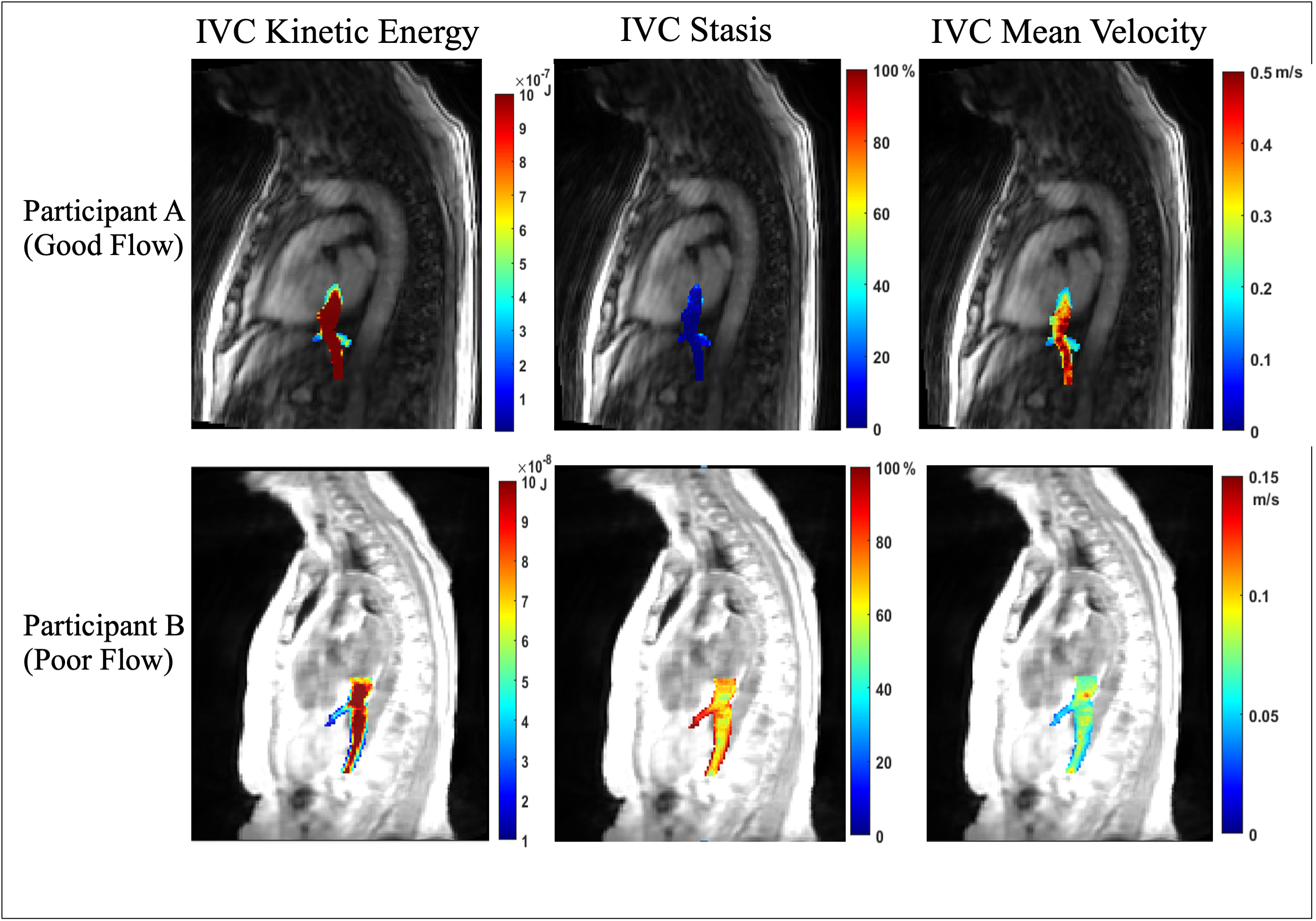
Figure 3: Quantitative colormaps of the 3D segmented inferior vena cava superimposed onto the corresponding reformatted anatomical images. Participant A represents normal flow with lower IVC stasis, higher kinetic energy, and higher mean velocity compared to the sample’s average calculations. Participant B represents poor flow with higher IVC stasis, lower kinetic energy, and lower mean velocities. (note different color scales were used to better illustrate the dynamic range of maps between participants)