0089
Spiral Real-time Phase Contrast MR on a 0.55T MRI System1Siemens Medical Solutions USA, Inc, Solon, OH, United States, 2Department of Biomedical Engineering, The Ohio State University, Columbus, OH, United States, 3Dorothy M. Davis Heart and Lung Research Institute, The Ohio State University, Columbus, OH, United States, 4Department of Radiology, The Ohio State University, Columbus, OH, United States, 5Division of Cardiovascular Medicine, The Ohio State University, Columbus, OH, United States, 6Department of Internal Medicine, Columbus, OH, United States
Synopsis
Keywords: Flow, Low-Field MRI
Motivation: Free-breathing (FB) real-time phase contrast (RT-PC) MR is very useful to resolve the beat-by-beat variations and for patients for whom breath-holding poses a challenge; however its feasibility remains to be tested at low-field.
Goal(s): To develop a FB RT-PC MR technique on a clinical wide-bore 0.55T MR scanner with reduced gradient performance.
Approach: FB RT-PC was developed using a dual-density spiral readout with a modified golden-angle rotation strategy and compressed sensing reconstruction. Flow quantifications were compared with the conventional BH segmented PC approach.
Results: Our proposed method yielded flow measurements of comparable accuracy and effectively captured the peak flow dynamics at low-field.
Impact: The proposed RT PC MR technique for low-field systems could enable flow imaging for patients with arrhythmias, critical illnesses, or claustrophobia, potentially making cardiac MRI more accessible and patient-friendly in a variety of clinical settings.
Introduction
Low-field, ultra-wide bore MRI systems offer several advantages that could potentially expand the accessibility of cardiac MRI [1]. Conventional phase-contrast (PC) MR [2] relies on ECG synchronization with respiratory control to measure blood flow averaged over multiple heartbeats. The technique fails to resolve the beat-by-beat variations that occur with arrhythmia [3]. Furthermore, for young or critically ill patients, or those with shortness of breath or severe claustrophobia, breath-holding (BH) can be challenging. Real-time (RT) PC MR, without ECG gating or BH, has been shown to address these limitations on 1.5T and 3T clinical scanners [4-6]; however, its feasibility remains to be tested at low-field. The aim of the study was to develop a RT-PC MR technique using a modified golden-angle spiral acquisition and compressed sensing (CS) reconstruction on a clinical 0.55T MR scanner (MAGNETOM Free.Max, Siemens Healthineers AG, Erlangen, Germany) with 80 cm bore and reduced gradient performance of 26 mT/m amplitude, 45/T/m/s slew rate.Methods
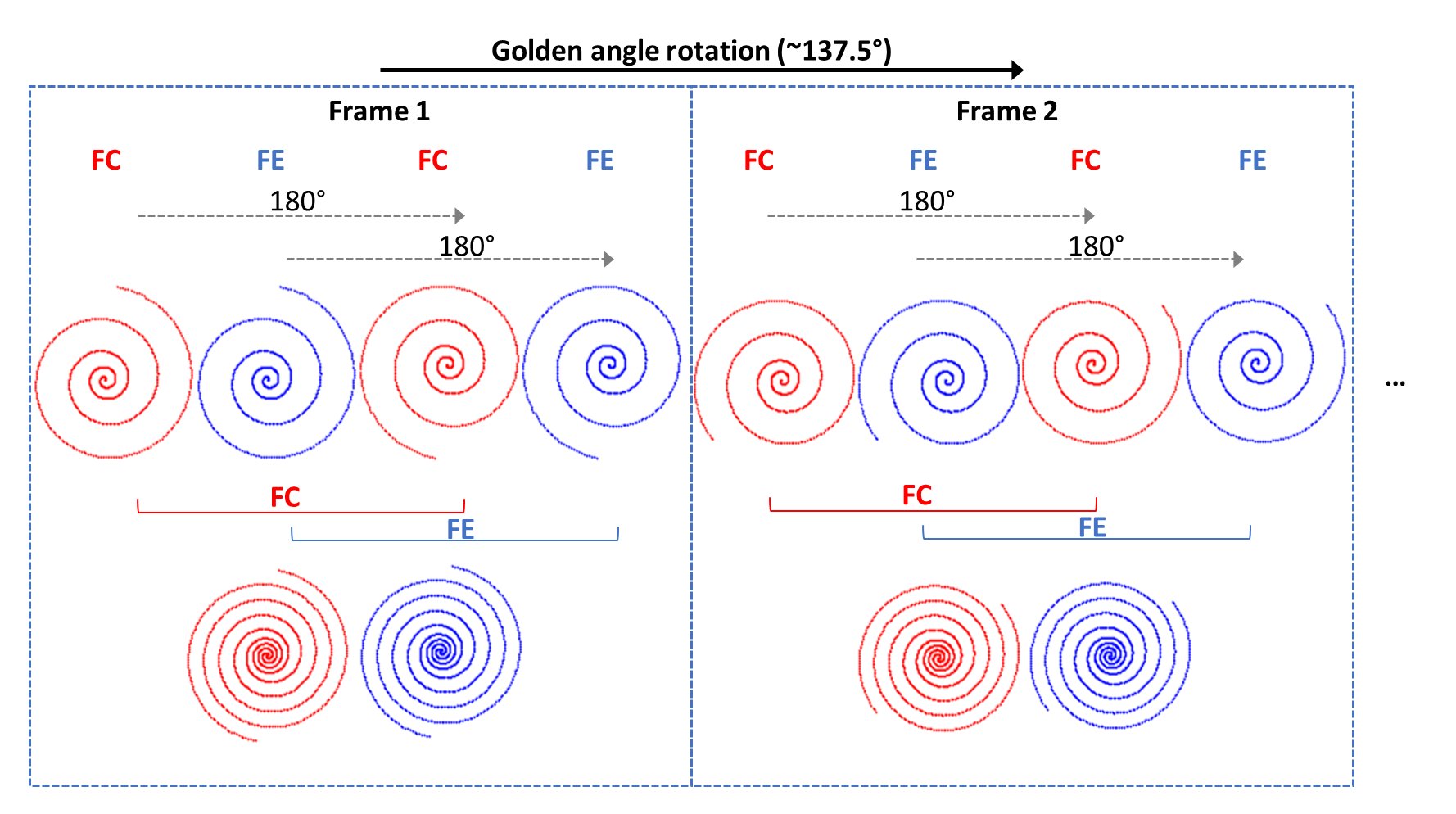
The free-breathing (FB) spiral RT-PC research sequence was implemented using a dual-density spiral trajectory with the first 30% of the spiral readout sampled at twice the Nyquist rate, and the remaining 70% sampled at 60% of Nyquist rate [7]. The imaging parameters were: FOV = 300x300 mm2, voxel size = 2.3x2.3x8 mm3, TR/TE = 11.0/3.0 ms, flip angle = 20°, VENC = 150/200 cm/s, acquisition time = 4 s. Two spiral interleaves were acquired for each frame resulting in 6-fold undersampling (12 interleaves if fully sampled) and a temporal resolution of 44 ms. Flow compensated (FC) and flow encoded (FE) readouts were interleaved in each frame. From one frame to the next, the spiral readouts were continuously rotated by the golden angle (~137.5°). Within each frame, the 2nd interleave was rotated by 180° relative to the first one to maximize the k-space coverage in each frame (Figure. 1).RT-PC images were reconstructed offline using SENSE based CS, with non-decimated wavelet (NWT) along both temporal and spatial dimensions as the sparsity transformation. The regularization parameters were tuned individually for each NWT band using a single dataset, and then fixed for all other subjects. The density compensation function was calculated following the method presented in [8] and the 2D NUFFT implementation provided in [9] was utilized. The coil sensitivity maps were estimated from the time-averaged FC image using ESPIRiT [10].
For comparison, a BH retrospective ECG-gated Cartesian PCMR sequence was acquired with the following parameters: voxel size = 1.7x2x8 mm3, TR/TE = 6.7/3.71 ms, flip angle = 12°, GRAPPA = 2, temporal resolution = 53 ms, acquisition time = 10 heart beats.
Nine healthy volunteers (4 males, 32±17 years) were scanned on a 0.55T using FB spiral RT-PC and BH Cartesian PC, with 2D flow measured perpendicular to the ascending aorta (AO) in all volunteers and the main pulmonary artery (MPA) in 7 volunteers. The flow waveforms from RT-PC were averaged over consecutive cardiac cycles into one waveform to compare it with the reference standard.
Results
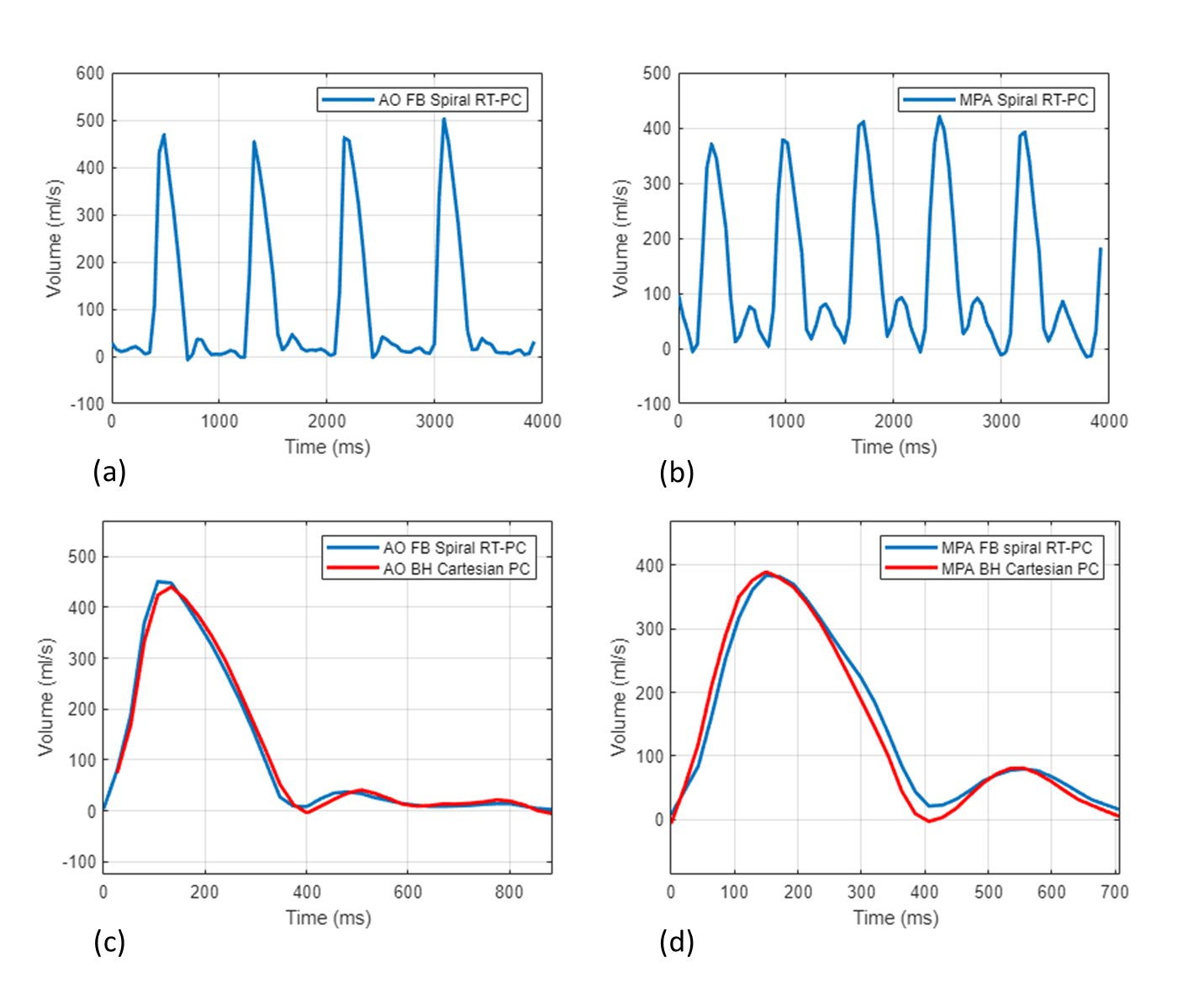
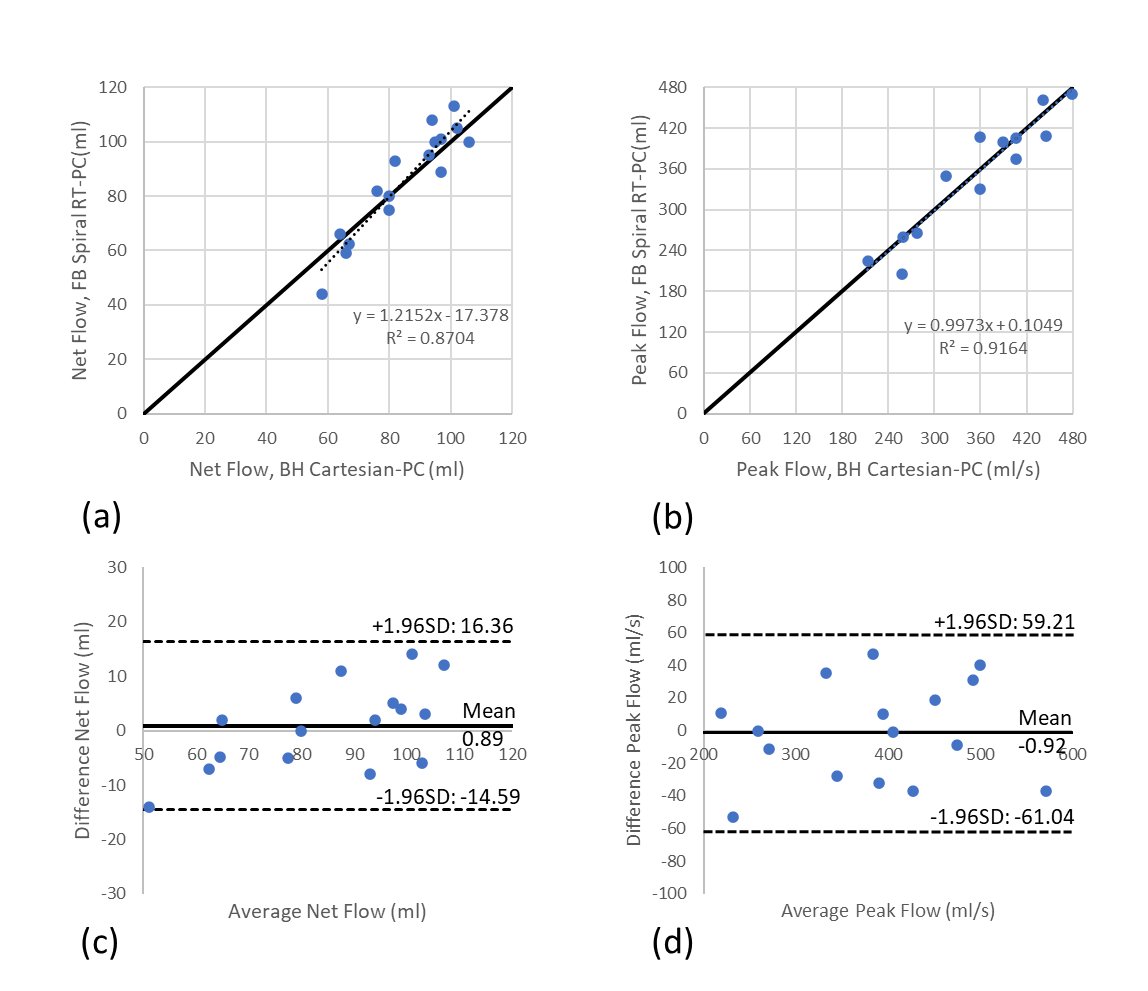
Figures 2 and 3 show the representative PC images in the AO and MPA from one healthy volunteer acquired by BH Cartesian PC and FB spiral RT-PC. Although both methods can resolve the vessel structure, Cartesian PC is visually noisier while the CS reconstruction improves SNR for RT flow. The flow curves from one subject show that spiral RT-PC (Figure 4a,b) was able to resolve beat-to-beat variations, and that the averaged flow curves for AO and MPA correlate well with Cartesian PC, with both methods yielding similar peak flow (Figure 4c,d). Correlations (Figure 5a,b) and Bland-Altman plots (Figure 5c,d) of net flow and peak flow reveal good agreement between the two methods.Conclusion
We demonstrated the feasibility of FB spiral RT-PC using a dual-density spiral readout with a modified golden-angle rotation strategy and CS reconstruction on a wide-bore 0.55T clinical system. Our proposed technique yielded flow measurements of comparable accuracy and effectively captured the peak flow dynamics, relative to the traditional BH segmented PC method. FB spiral RT-PC can be a valuable tool in the assessment of flow hemodynamics, particularly for patients for whom breath-holding poses a challenge.Acknowledgements
No acknowledgement found.References
- Simonetti OP, Ahmad R. Low-Field Cardiac Magnetic Resonance Imaging: A Compelling Case for Cardiac Magnetic Resonance's Future. Circ Cardiovasc Imaging. 2017 Jun;10(6)
- Firmin DN, Nayler GL, Klipstein RH, Underwood SR, Rees RS, Longmore DB. In vivo validation of MR velocity imaging. J Comput Assist Tomogr. 1987;11:751–756.
- Lin HY, Bender JA, Ding Y et al (2012) Shared velocity encoding: a method to improve the temporal resolution of phase-contrast velocity measurements. Magn Reson Med 68:703–710
- Xiong F, Emrich T, Schoepf UJ, Jin N, Hall S, Ruddy JM, Giese D, Lautenschlager C, Emrich AL, Varga-Szemes A. Highly accelerated free-breathing real-time 2D flow imaging using compressed sensing and shared velocity encoding. Eur Radiol. 2023
- Kowalik GT, Knight D, Steeden JA, Muthurangu V. Perturbed spiral real-time phase-contrast MR with compressive sensing reconstruction for assessment of flow in children. Magn Reson Med. 2020 Jun;83(6):2077-2091.
- Chen C, Gregg MA, Liu Y, Jin N, Raman SV, Simonetti OP, Ahmad R. Inline real-time phase-contrast cardiac MRI with Cartesian sampling. Abstract# 751158, The 23rd Annual SCMR Scientific Sessions, 2020
- CH Meyer, L Zhao, M Lustig, M Jilwan-Nicolas, M Wintermark, JP Mugler, FH Epstein. Dual-density and parallel spiral ASL for motion artifact reduction. Proceedings ISMRM 2011, p. 398
- Meyer CH, Hu BS, Nishimura DG, Macovski A. Fast spiral coronary artery imaging. Magn Reson Med. 1992;28(2):202-213. doi:10.1002/mrm.1910280204
- Lim Y, Toutios A, Bliesener Y, Tian Y, Lingala SG, Vaz C, Sorensen T, Oh M, Harper S, Chen W, Lee Y, Töger J, Monteserin ML, Smith C, Godinez B, Goldstein L, Byrd D, Nayak KS, Narayanan SS. A multispeaker dataset of raw and reconstructed speech production real-time MRI video and 3D volumetric images. Sci Data. 2021 Jul 20;8(1):187.
- Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med. 2014 Mar;71(3):990-1001.
Figures