0087
Inline automatic quality control of 2D phase-contrast flow MR imaging for subject-specific scan time adaptation1Laboratory of Imaging Technology, National Heart, Lung & Blood Institute, NIH, Bethesda, MD, United States, 2Cardiovascular Branch, National Heart, Lung & Blood Institute, NIH, Bethesda, MD, United States, 3Siemens Healthcare Ltd., Calgary, AB, Canada
Synopsis
Keywords: Data Acquisition, Low-Field MRI, MR value
Motivation: Conventional fixed duration acquisitions can result in patient-dependent image quality, leading to either unnecessarily long scan times or insufficient quality across patients.
Goal(s): We propose an inline automatic quality control based on signal-to-noise ratio (SNR) to achieve consistent diagnostic image quality and apply it to 2D phase-contrast flow MRI.
Approach: We designed a closed-loop feedback framework between image reconstruction and data acquisition to automatically stop the acquisition when a target SNR is achieved. Ten healthy volunteers and one patient were imaged at 0.55T.
Results: Deployed inline, the SNR stop threshold saved 53% of the scan duration, with a variation of ±1min across subjects.
Impact: The inline automatic quality control enables a subject-specific optimized scan time while ensuring consistent diagnostic image quality. The distribution of automated stopping times across the population revealed the value of a subject-specific scan time.
Introduction
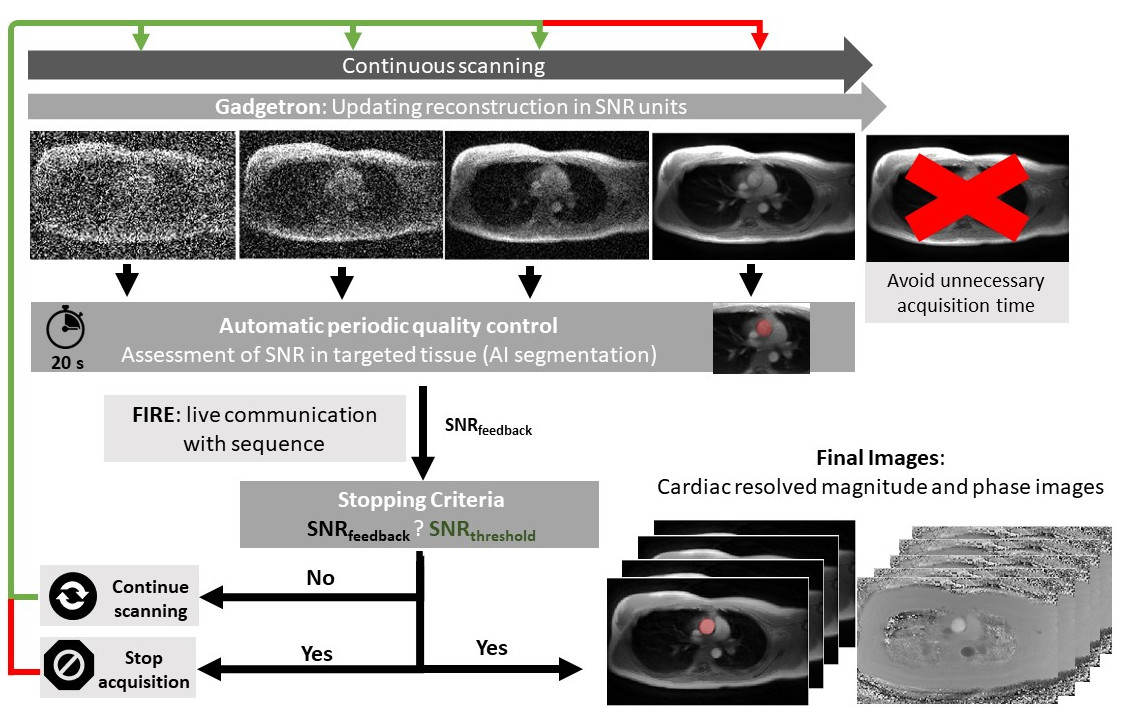
Conventional MRI acquisitions are optimized with a fixed duration to provide acceptable image quality for most patients. However, image quality is patient-dependent which may lead to unnecessary scan time for some patients or insufficient quality for others due to body habitus or heart rate. Therefore, we proposed an inline automatic quality control based on closed-loop feedback framework between image reconstruction and data acquisition to efficiently achieve consistent diagnostic image quality. Since the signal-to-noise ratio (SNR) is directly related to confidence of flow measurements1, we applied this framework for quantitative flow measurements with cardiac 2D phase-contrast flow MRI using a SNR threshold as a stop criterion for a subject-specific imaging duration.Methods
The closed-loop feedback framework is designed as follows (Figure 1): during the acquisition, SNR maps are reconstructed in Gadgetron2 every 20s using 100 pseudo replicas3, then the SNR of the target tissue is extracted automatically using a trained nnUNet4, and sent from Gadgetron to the sequence controller via the “FIRE” research framework5 (Siemens Healthineers AG, Germany). The acquisition automatically stops when a target SNR is achieved.Ten healthy volunteers (HV) (BMI=25.4±2.5, age=30±8 years old, male/female=4/6) and one patient (BMI=29.3, age=73 years old, female) with a valvular implant were imaged on a 0.55T MRI scanner (MAGNETOM Free.Max, Siemens Healthineers AG, Germany) using a free-breathing GRE pseudo-golden-angle spiral flow research sequence (TE/TR=2.0/10.5ms, FA=25°, 1.7mm2 resolution, venc=200cm/s, FOV=384mm2) modified to listen for a ‘stop’ message. The acquisition was run with (6 HVs) or without (10 HVs) closed-loop feedback with a maximum scan time of 4min35s (ascending aorta, AAo) or 6min (main pulmonary artery, MPA). At the end of the scan, data were retrospectively self-gated to 25 cardiac frames and reconstructed using T-CG-SENSE with a spatial and temporal constraints (λs=0.1, λt=1).
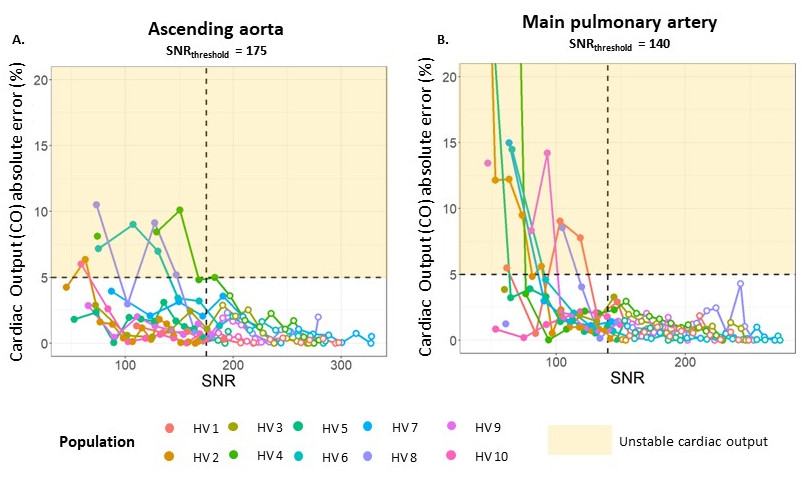
The stopping criterion (SNR threshold) was chosen to produce an accurate measurement of cardiac output, defined as <5% absolute relative error (CO%error) compared measurements from the full acquisition. This optimal targeted tissue specific SNR was then applied inline.
For the automatic segmentation, 2D nnUNet were trained on 128 patients and evaluated on a test dataset including 10 patients (Dice Similarity Coefficient=0.95±0.02 for AAo and MPA), all of whom were imaged at 1.5/0.55T. Quality control and image reconstructions were performed on a computer equipped with 4 GPUs (NVIDIA A100-SXM, 80Gb). Subject imaging was performed with IRB approval.
Results
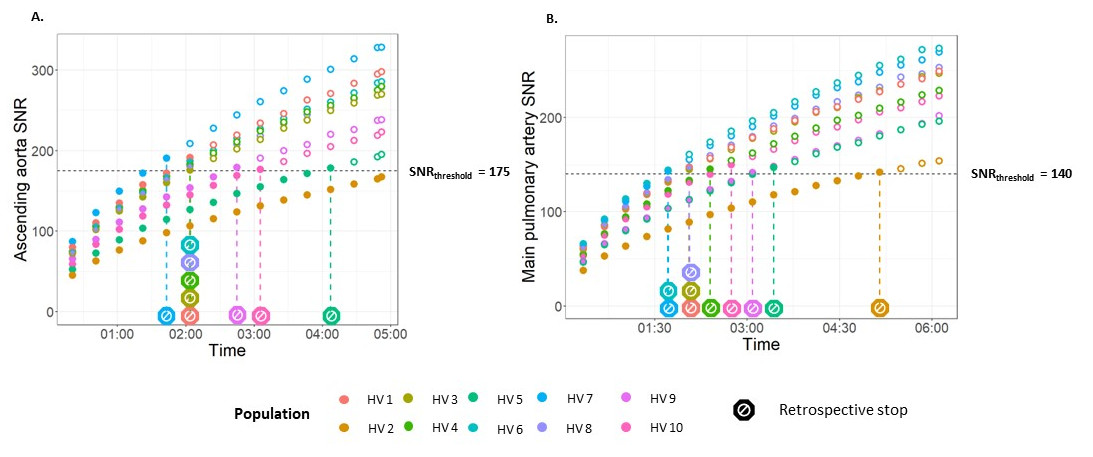
Retrospective analysis demonstrated that by choosing an SNR threshold of 175 (total across all cardiac frames) for AAo and 140 for MPA (Figure 2), we ensured sufficient image quality to keep quantitative flow measurements with an error ≤ 5% relative to the full duration measurement. By applying these optimal SNR thresholds retrospectively (Figure 3), acquisition would have automatically stopped at 2min 41s±62s/2min 39s±63s, saving 41%/57 % of scan time for AAo and MPA.Deploying the closed-loop feedback inline, target SNR was reached at 2min27s±53s/2min50s±69s with SNR=181±5/145±3 and the acquisition stopped at 2min39s±67s/3min±80s saving 43%/51% of the scan duration for AAo and MPA (Figure 4). Compared to the full acquisition, the CO%error was 2.13±2.04%/6.34+3.73% with a maximum of 5.43%/11.5% for AAo/MPA. For one subject with BMI=28.8, the full acquisition for AAo was too short to reach the target SNR (max SNR=164). The SNR-driven acquisition was also successful and generated diagnostic flow measurements in the one patient, despite a metallic valvular implant (Figure 4).
Two example subjects are shown in Figure 5 for illustration. Using a 2 min fixed acquisition time (top row), CO%error was 5.4% compared to the full acquisition due to insufficient SNR. Whereas, in a different subject (bottom row), the SNR-driven acquisition stopped the scan at 1min40 but with a CO%error≤1%, avoiding unnecessary acquisition time.
When deployed inline, SNR map computation required 12.98±5.49s and automatic segmentation required 1.08±0.09s, meaning that SNR calculation was always feasible within the 20s assessment interval.
Discussion
We demonstrated an inline SNR-driven automatic quality control for adaptive subject-specific MRI acquisition time applied to 2D phase contrast MR flow measurements of the great arteries. The distribution of automated stopping times across the population (standard deviation of 62/63s for AAo/MPA) revealed the value of subject-specific acquisition time for consistent image quality instead of fixed duration (Figure 5). It resulted in a 41%/57% acquisition time savings while ensuring a diagnostic measurement with an average error in quantitative flow parameters lower than 2.2% and 6.4% for AAo and MPA respectively.Conclusion
Our inline SNR-driven automatic quality control enables time-efficient subject-specific acquisitions while ensuring diagnostic image quality and consistent quantitative flow measurement compared to full time acquisitions. This framework could be adapted for other applications using different quality metric.Acknowledgements
This work was supported by the National Heart, Lung, and Blood Institute (NHLBI) Division of Intramural Research (Z01-HL006257, Z01-HL006213). The authors are investigators on a US Government Cooperative Research and Development Agreement (CRADA) with Siemens Healthcare to develop 0.55T MRI.References
1. Hansen MS, Olivieri LJ, O’Brien K, Cross RR, Inati SJ, Kellman P. Method for calculating confidence intervals for phase contrast flow measurements. J Cardiovasc Magn Reson. 2014;16(1):46. doi:10.1186/1532-429X-16-46
2. Hansen MS, Sørensen TS. Gadgetron: An open source framework for medical image reconstruction: Gadgetron. Magn Reson Med. 2013;69(6):1768-1776. doi:10.1002/mrm.24389
3. Robson PM, Grant AK, Madhuranthakam AJ, Lattanzi R, Sodickson DK, McKenzie CA. Comprehensive quantification of signal-to-noise ratio and g -factor for image-based and k -space-based parallel imaging reconstructions. Magn Reson Med. 2008;60(4):895-907. doi:10.1002/mrm.21728
4. Isensee F, Jaeger PF, Kohl SAA, Petersen J, Maier-Hein KH. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nat Methods. December 2020. doi:10.1038/s41592-020-01008-z
5. Chow K, Kellman P, Xue H. Prototyping Image Reconstruction and Analysis with FIRE. In: SCMR. Virtual Scientific Sessions. ; 2021:838972.
Figures