0082
MR microscopy to assess clot composition following mechanical thrombectomy predicts recanalization and clinical outcome1Neuroradiology, University Hospital Heidelberg, Heidelberg, Germany, 2Neurology, University Hospital Heidelberg, Heidelberg, Germany, 3Neurology, University Hospital Mannheim, Mannheim, Germany, 4Neuropathology, University Hospital Heidelberg, Heidelberg, Germany
Synopsis
Keywords: Stroke, Stroke
Motivation: Mechanical thrombectomy (MT) is the standard for ischemic stroke with large vessel occlusion (LVO). Clot composition is underexplored in clinical practice, leading to standardized MT regardless of clot type.
Goal(s): This single-center study examined clot composition in 60 LVO stroke patients using high-field MRI at 9.4T ("MR-microscopy").
Approach: MR microscopy correlated with histopathology, and quantifying the hyperdense artery sign (HAS) on pre-interventional CT further stratified clot composition.
Results: MR microscopy successfully identified clot types—red (23%), white (28%), or mixed (48%)—with 95.4% accuracy. White clots required more passes during MT, had worse clinical outcomes, while red clots showed better first-pass recanalization rates.
Impact: This study suggests clot imaging can personalize MT for improved outcomes in LVO stroke patients.
Background
Mechanical thrombectomy (MT) is the standard of care for ischemic stroke patients with large vessel occlusion (LVO) eligible for endovascular treatment.1,2 Clot composition is not routinely assessed in clinical practice as no specific diagnostic value is attributed to it and currently, MT is performed in a standardized “non-personalized” approach, irrespective of the stroke etiology or clot composition. Whether different clot compositions are associated with intrinsic likelihoods of recanalization success or treatment outcome is unknown.Methods
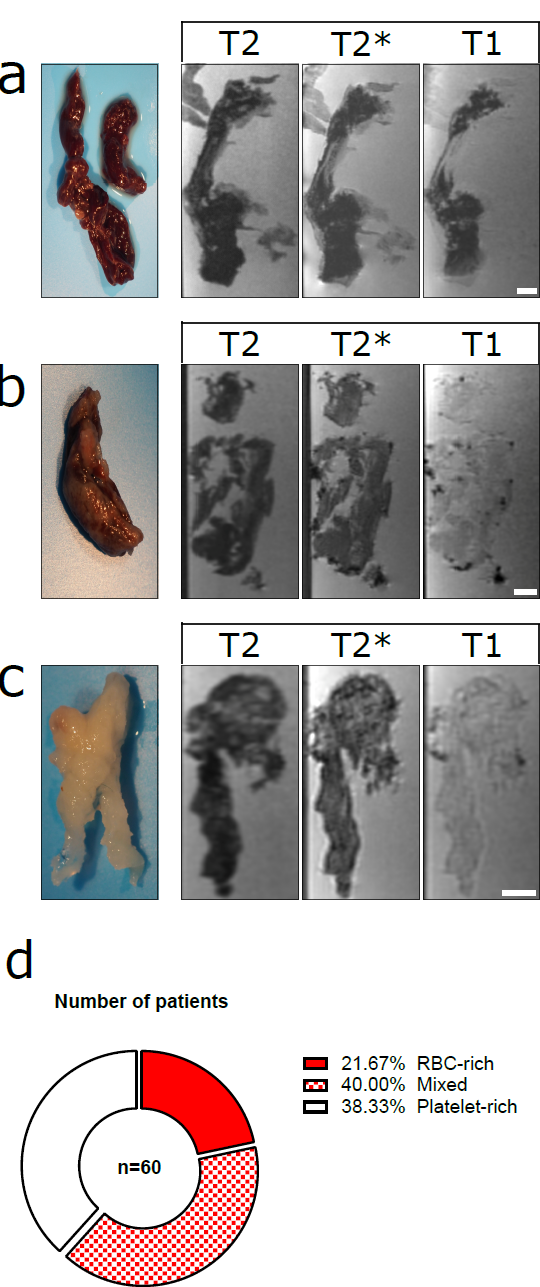
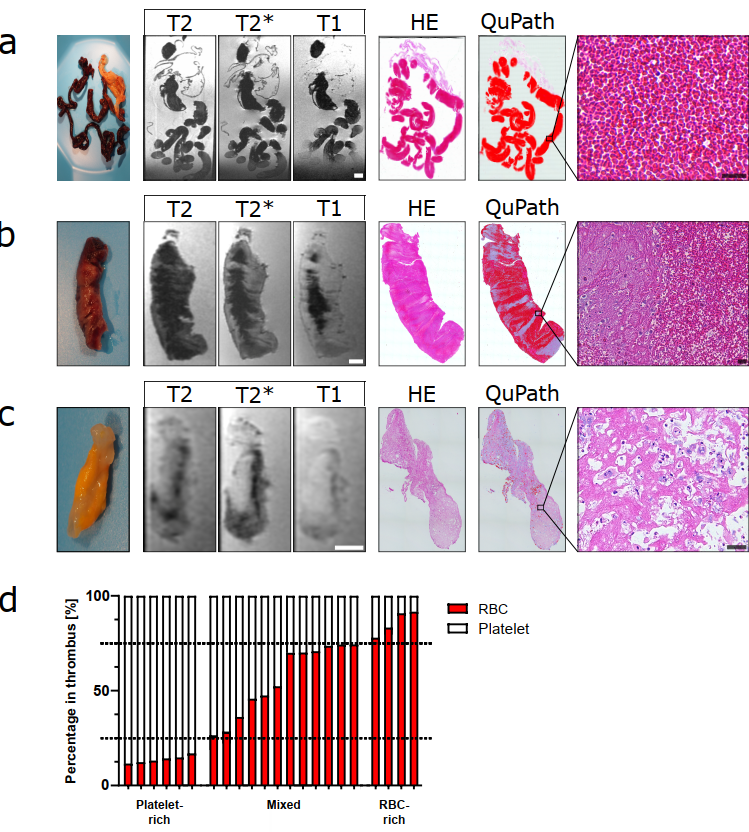
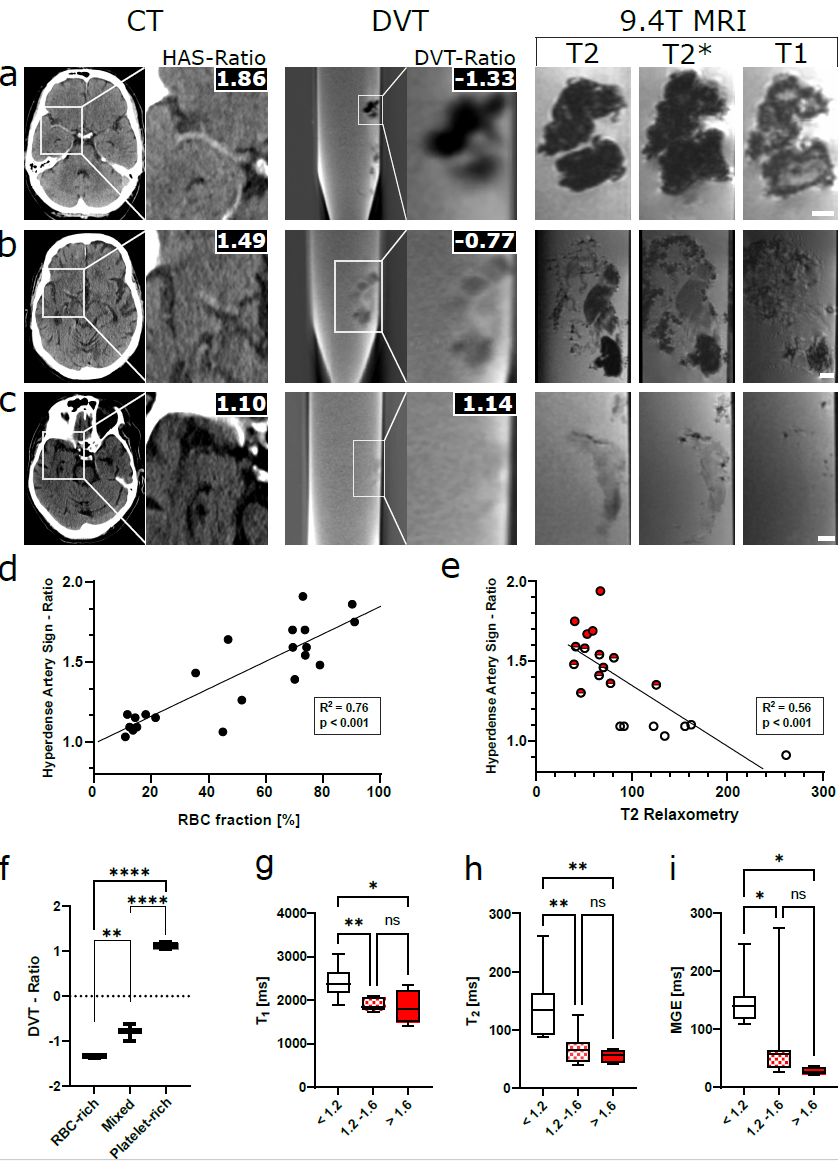
We performed a prospective, non-randomized, single center study and systematically analyzed the clot composition in 60 consecutive ischemic stroke patients undergoing MT at our institution. Clot specimens were assessed by ex vivo high field MRI at 9.4T (“MR-microscopy”, MR-M) by anatomical and relaxometric MR sequences and high-resolution DVT. Histopathology was performed to validate MR-M results in a subset of 22 specimens. Clot imaging was correlated with preinterventional CT for hyperdense artery sign (HAS) quantification and clinical data.Results
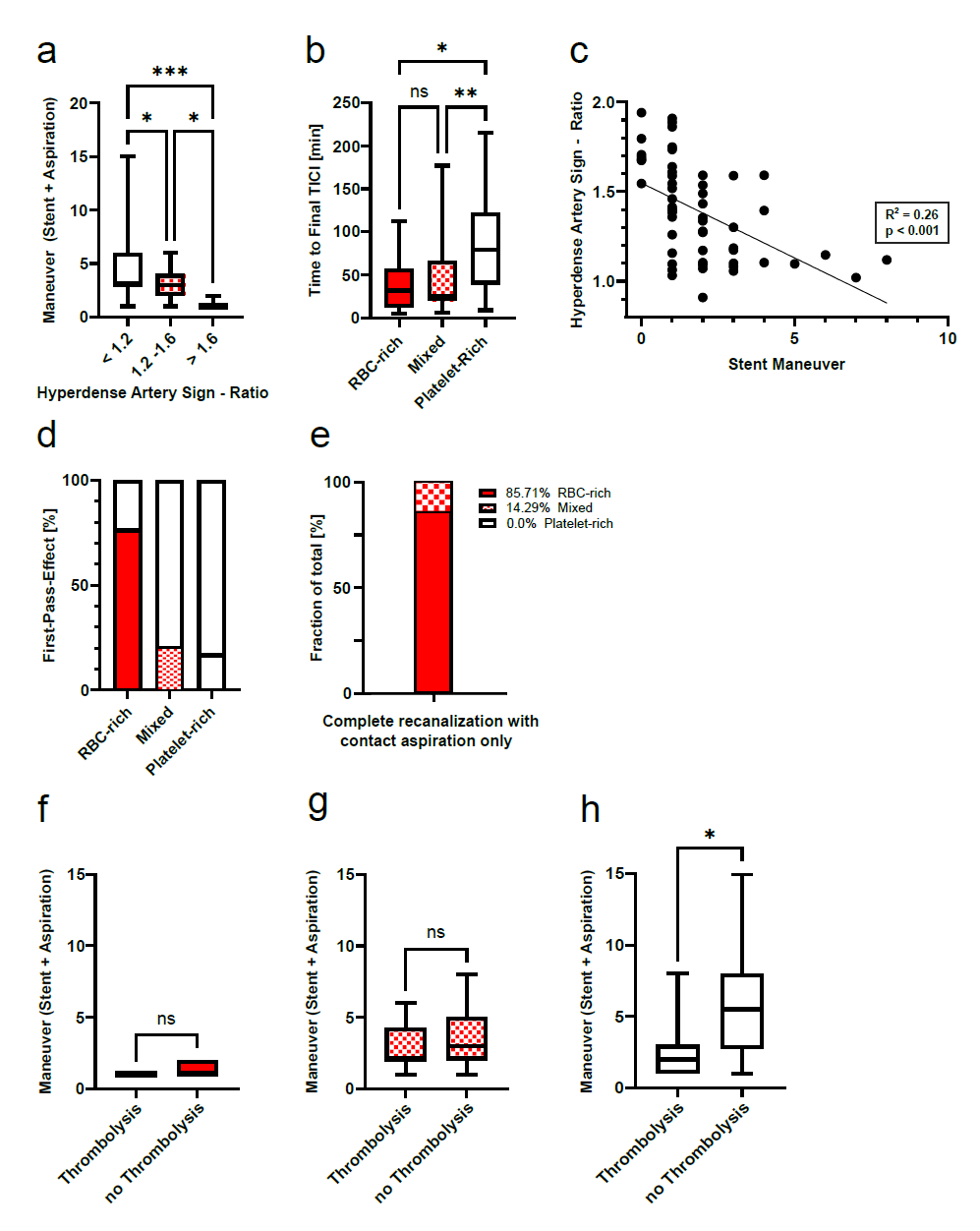
Ex vivo high field MR microscopy had high accuracy of 95.4% to differentiate the different clot types and 21/22 clots were categorized correctly using histopathology as ground truth. MR microscopy showed red blood cell-rich (red, 23% of clots), platelet-rich (white, 28%) or mixed clots (48%) as distinct morphological patterns. T2* times differed between the clots types as assessed by MR relaxometry. Clot composition could be further stratified by quantifying the HAS on pre-interventional non-enhanced CT. During MT, white clots required significantly more passes to achieve final recanalization and were not amenable to contact aspiration compared to mixed and RBC-rich clots, whereas red clots showed highest probability of first pass recanalization (76.92%) compared to white clots (17.39 %). Clinically, white clots were associated with poorer clinical outcome and performance status at 90 mRS.Discussion
Our study characterizes the composition of retrieved clots following MT by multimodality quantitative imaging and introduces MR microscopy to assess clot composition. Our study demonstrates that preinterventional clot imaging by quantification of the HAS or MR relaxometry could guide the interventional strategy and predict clinical outcome. Thus, our study could enable a personalized treatment approach to improve radiological MT results and ultimately clinical outcome of stroke patients with LVO undergoing MT. In subsequent studies, we aim to investigate the composition of clots in patients suffering from stroke secondary to pertinent pre-existing conditions, such as cancer. We hypothesize that these clots exhibit a complex structure that may impede mechanical recanalization efforts. Notably, the application of relaxometry for quantification holds substantial potential for pre-interventional clot detection; currently, relaxometry is being measured in artificially generated thrombi within the context of another study, which may standardize this assessment technique.Acknowledgements
The authors thank Dr S Bonekamp (Neuroradiology Department, University Hospital Heidelberg) for organizational and Manfred Jugold (DKFZ) for technical support of this study.References
1. Berkhemer OA, Fransen PSS, Beumer D, et al. A randomized trial of Intraarterial
treatment for acute ischemic stroke. N Engl J Med 2015;372:11–20.
2.
Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after
large-vessel ischaemic stroke: a meta-analysis of individual patient data from five
randomised trials. Lancet 2016;387:1723–31.
Figures