0081
Detection of Acute Infarction Using 0.23T Mobile Magnetic Resonance Imaging in Patients with Minor Ischemic Stroke or Transient Ischemic Attack1Tiantan Neuroimaging Center of Excellence, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 3China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Synopsis
Keywords: Stroke, Stroke
Motivation: Low-field mobile MRI (0.064T) enables early identification of acute infarction(s) for patients with minor ischemic stroke (MIS) or transient ischemic attack (TIA). Improving the spatial resolution and shortening the scanning time are needed.
Goal(s): This study sought to compare the performance of low-field mobile MRI (0.23T) and 3T MRI in detecting acute infarction(s) in MIS or TIA patients within 14 days since onset.
Approach: The accuracy was calculated. The ground truth was defined as the closest 3T fixed MRI examination.
Results: The accuracy of mobile low-field MRI in detecting acute infarction(s) was 96.1%. Overall scan time was shortend compared to the 0.064T system.
Impact: The performance of 0.23T low-field mobile MRI in detecting acute ischemic infarctions was comparable with 3T MRI in our study.
Introduction/Purpose
Early identification of patients with acute ischemic lesion is of great importance for development of acute treatment and secondary prevention plan for patients with minor ischemic stroke (MIS) or transient ischemic attack (TIA). The application of the Hyperfine 0.064T MRI in the intensive care unit for diagnosis and differential diagnosis of neurological diseases is well-received and with high efficiency. 1-3 However, the nature of low-field intensity has impeded the Hyperfine system from discovering small ischemic lesion. The scanning time of one examination is long (35 minutes for 4 sequences). 1 Improving the spatial resolution and shortening the scanning time are important topics for future solutions of mobile low-field MRI. Recently, the national medical products administration of China has approved a low-field (0.23T) mobile MRI, ACUTA Elfin.4 Compared to fixed MRI, mobile MRI could optimize the intrahospital transportation workflow and reduce cardiovascular and respiratory risks during transportation.2 We sought to compare the performance of ACUTA Elfin and 3T MRI in discovering acute ischemic lesion (acute infarction) in patients with MIS or TIA within 14 days since the last-known well time (the time at which the patient’s condition was last reported to be normal).Method
We prospectively included 102 patients from April 2022 to May 2023 in Beijing Tiantan Hospital who underwent both mobile MRI and 3T fixed brain MRI (uMR NX, United Imaging Healthcare). Imaging protocol of mobile MRI and 3T MRI included axial T1-weighted fluid-attenuated inversion recovery (or FLAIR), T2-weighted FLAIR, T2-weighted fast spin-echo, and DWI with apparent diffusion coefficient sequences. Sequence details were shown in Table 1 and Table 2. Images were centrally reviewed by 2 raters. Any disagreements were resolved by a third rater. Using the weighted Cohen k statistics, we compared the performance of low-field mobile MRI and 3T MRI in discovering acute ischemic lesion (lesion number, distribution). The comparison of performance of low-filed mobile MRI on acute ischemic lesion discovery were evaluated using weighted Cohen k statistics. A greater than 0.75 Cohen k coefficient will be considered as excellent. The ground truth was defined as the closest 3T fixed MRI examination. Accuracy, sensitivity, and specificity of ischemic infarction(s) detection were calculated based on the consensus of the raters. A 2-sided p-value < 0.05, was considered statistically significant.Results
The median age of included patients were 60 years and 15.7% of the patients were female. The scan protocols of low-field mobile MRI and 3T MRI both consist of axial T1-weighted fluid-attenuated inversion recovery (or FLAIR), T2-weighted FLAIR, T2-weighted fast spin-echo, and DWI with apparent diffusion coefficient sequences. The low-field mobile MRI scan takes 15 minutes 11 seconds and 3T MRI scan takes 2 minutes 43 seconds. The median time interval between low-field mobile MRI and 3T MRI was 18.5 minutes. Eighty-five patients’ infarction(s) were detected by both 3T MRI and low-field (0.23T) mobile MRI. In four patients, the ischemic infarction(s) were identified by the 3T MRI but not by the 0.23T MRI (Figure 1), while in 13 patients, no lesions were detected by either the 3T or 0.23T MRI (96.1% overall accuracy, 97.9% sensitivity (95%CI: 88.2%-98.6%), 100% specificity (95%CI: 71.7%-100%)). There were no patients identified with lesions by the 0.23T MRI that were missed by the 3T MRI. The agreement between the two imaging modalities in diagnosing acute infarction(s) and infarction number were 0.84(0.70-0.99), 0.92(0.85-0.99), respectively. Patients were well tolerated, and no adverse events occurred.Discussion
We found that the 0.23T mobile MRI (Elfin) is comparable in discover acute ischemic lesion with 3T MRI in patients with MIS or TIA within 14 days since the last-known well time. Subcortical infarction or infarction of the brain stem with less than 5mm in the maximal axial dimension has a chance to be missed in mobile MRI examination. Safety and feasibility of using mobile MRI to evaluate patients with MIS or TIA was proved in this study. The multi-center prospective cohort is needed to further prove the feasibility and accuracy in imaging evaluation by mobile MRI of these patients.Conclusion
The performance of 0.23T low-field mobile MRI in detecting acute ischemic infarctions was comparable with 3T MRI in our study. Experienced clinicians could identify ischemic infarctions on 0.23T mobile MRI in 95.5% of patients with discernible infarctions at 3T MRI. With lower infrastructure requirements and reduced overall scan time, low-field mobile MRI holds significant importance for the diagnosis and treatment for MIS or TIA.Acknowledgements
We appreciated all the study participants and their relatives. We also appreciated the hard work and dedication of all relevant clinicians and imaging technicians who participated in the study.References
1. Sheth KN, Mazurek MH, Yuen MM, et al. Assessment of brain injury using portable, low-field magnetic resonance imaging at the bedside of critically ill patients. JAMA neurology. 2020;Sep 8;78(1):41-47.
2. Yuen MM, Prabhat AM, Mazurek MH, et al. Portable, low-field magnetic resonance imaging enables highly accessible and dynamic bedside evaluation of ischemic stroke. Science advances. 2022 Apr 22;8(16):eabm3952.
3. Kuoy E, Glavis-Bloom J, Hovis G, et al. Point-of-care brain mri: Preliminary results from a single-center retrospective study. Radiology. 2022;Dec;305(3):666-671.
4. https://www.Nmpa.Gov.Cn/yaowen/ypjgyw/20220831172100180.Html (attachment document). 2022;2023
Figures
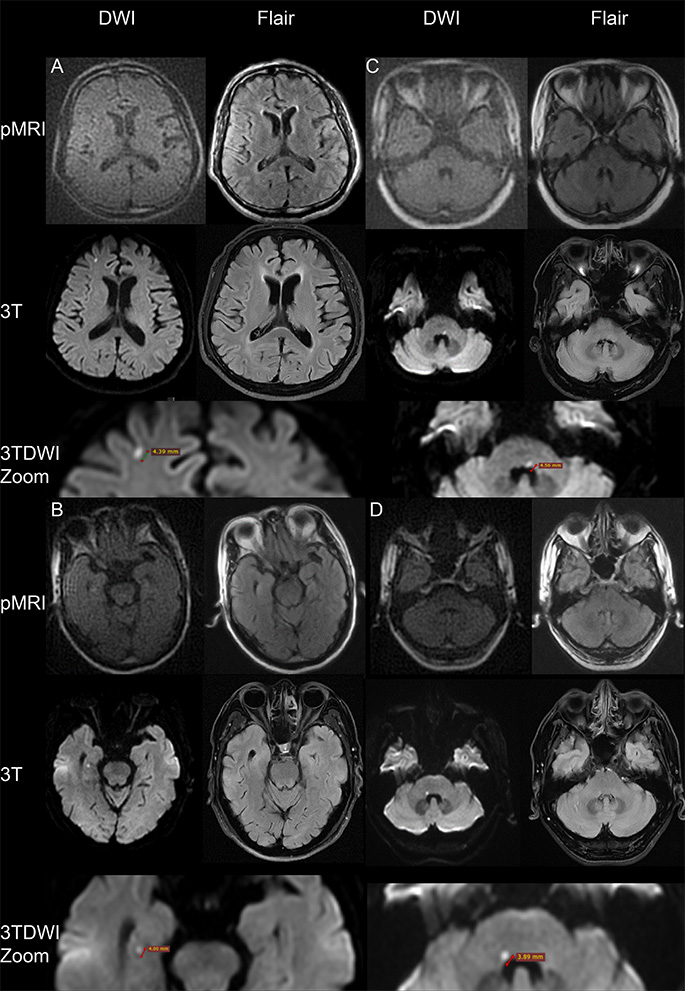
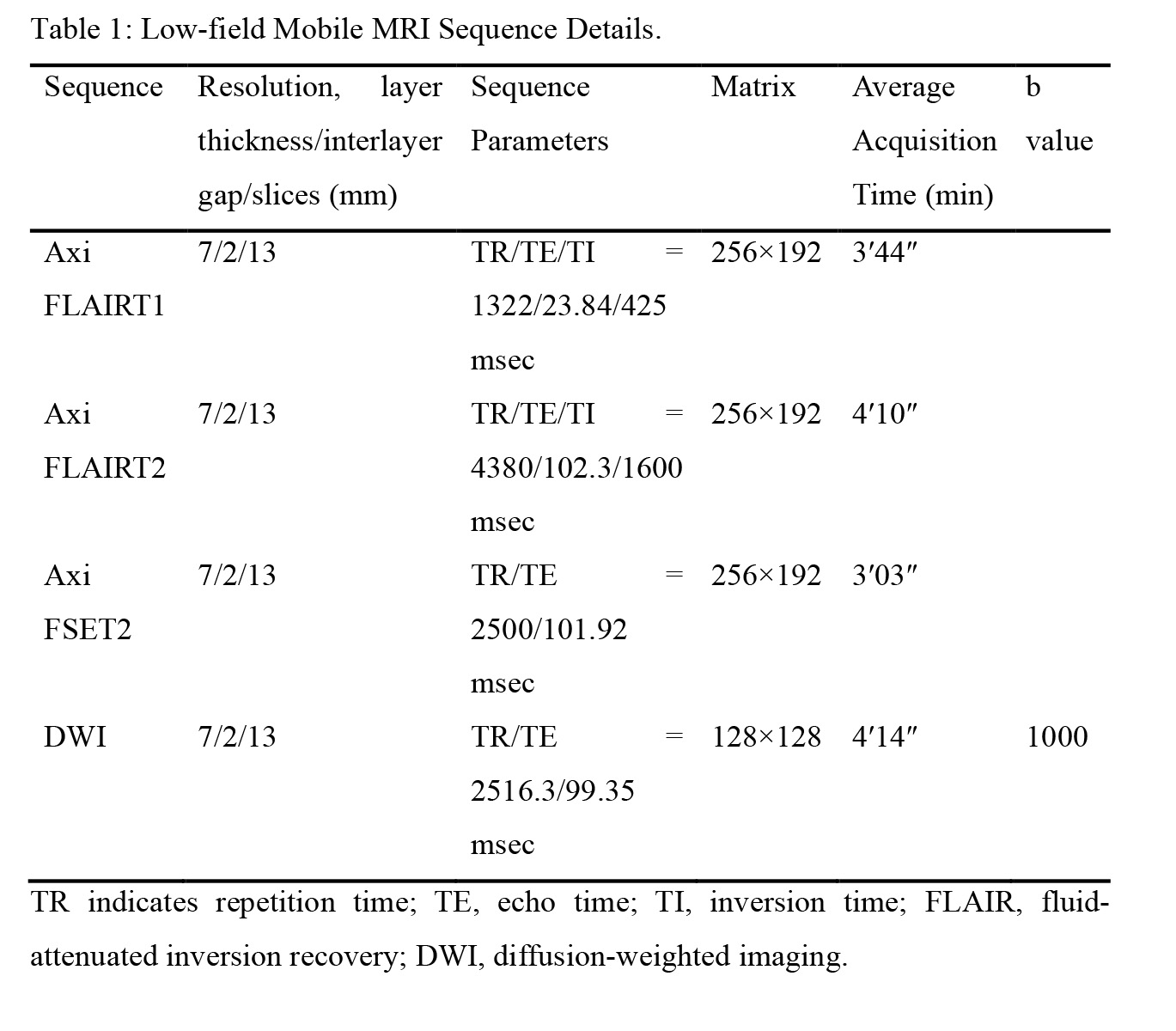
Table 1: Low-field Mobile MRI Sequence Details.
TR indicates repetition time; TE, echo time; TI, inversion time; FLAIR, fluid-attenuated inversion recovery; DWI, diffusion-weighted imaging.
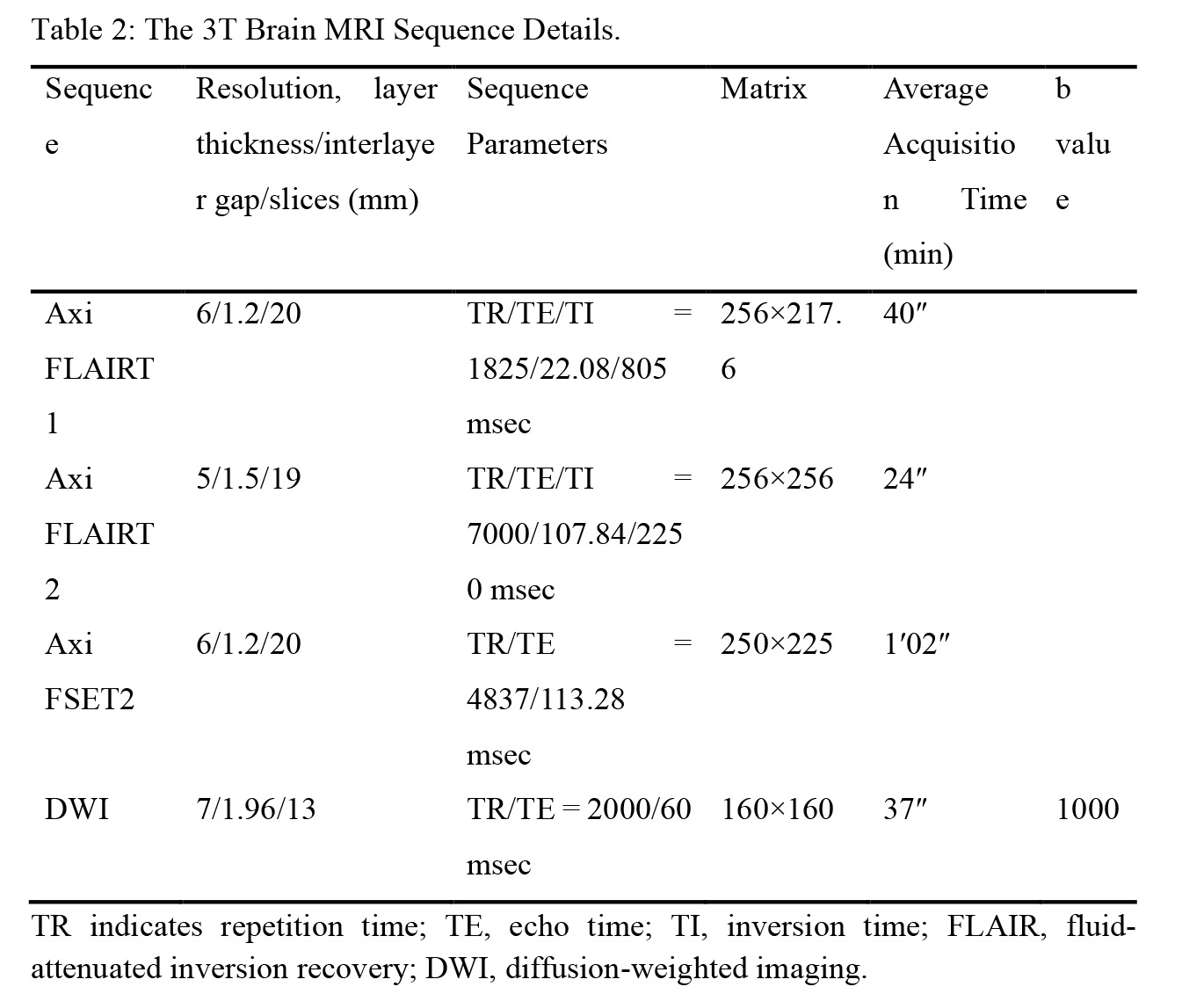
Table 2: The 3T Brain MRI Sequence Details.
TR indicates repetition time; TE, echo time; TI, inversion time; FLAIR, fluid-attenuated inversion recovery; DWI, diffusion-weighted imaging.