0076
Prediction value of DWI-ASPECTS and HR-VWI to evaluate the response of patients with acute ischemic stroke1First Affiliated Hospital of Harbin Medical University, Harbin, China, 2Philips Healthcare, Beijing, China
Synopsis
Keywords: Stroke, Atherosclerosis, ASPECTS, HR-VWI, RESPONSE, STROKE
Motivation: The predicted ability of High-resolution vessel wall imaging (HR-VWI) combined with diffusion-weighted imaging (DWI) in acute ischemic stroke (AIS) patients based on the simplified modified Rankin Scale questionnaire(smRSq)remains unknown.
Goal(s): The purpose is to analyze AIS patients by obtaining HR-VWI and DWI information for further providing the information for endovascular therapy.
Approach: Patients are grouped by smRSq including the good response group and the poor. The characteristics of plaque and DWI are analysed for comparing between the two groups.
Results: Severe stenosis, high normalized wall index, plaque enhancement, T1WI high signal and low ASPECTS were risk factors of poor response (all P<0.05).
Impact: The combination of HR-VWI and ASPECTS can assist clinical in adopting different rehabilitation management methods for patients.
Introduction
Stroke is a worldwide disease with high morbidity. Atherosclerosis (AS) remains the primary cause of ischemic stroke1, but the effective method for predicting patients with AIS is limited. Narrowing or occlusion of the lumen due to AS decrease cerebral blood flow which could result in AIS. ASPECTS serves as a tool to make treatment decision-making with the advantages of simple, fast and reliable. HR-VWI as one of the best non-invasive methods for displaying the vascular features of intracranial atherosclerosis plays an irreplaceable role in evaluating the plaque burden and stability. The hyperintensity of T1WI and plaque enhancement play a positive predictive effect which have been confirmed in forecasting the outcome of patients2. Other characteristics of atherosclerotic plaque also have the predictive value for the response of patients2. Therefore, the purpose of this study is to analyze AIS patients with different condition by obtaining the characterizes of vessel wall and diffusion information for further providing the information for endovascular therapy.Methods
Forty-three patients with AIS in the anterior circulation who underwent endovascular treatment were enrolled from September 2021 to May 2023. AIS was determined based on high-signal lesions on diffusion-weighted imaging and the corresponding central nervous dysfunction in 1 week. The hyperintense lesions on DWI were located in the blood supply area of the middle cerebral artery. AIS patients after 3 months was obtained by telephone follow-up for classifying patients into good and poor response according to the smRSq at 90 days after discharged. All patients were divided into the good response group (smRSq≤2, 29 cases) and the poor response group (smRSq≥3, 14 cases)9.All participants were scanned on a 3.0T MRI scanner (Ingenia Elition; Philips Healthcare, Best, the Netherlands) with a 32-channel cranial phased array coil. HR-VWI scanning sequences were including T1WI-VISTA,T2WI-VISTA,SNAP and gadolinium-based contrast enhancement T1WI (Figure 1) with the following parameters: 0.6 mm isotropic resolution, 160×160 mm FOV, 228×228 matrix, 120slices. All images were postprocessed on Philips IntelliSpace Portal software. The culprit plaque was defined as the one responsible for the most severe stenosis. Quantitative parameters were analyzed, such as vascular lumen area of stenosis (Vmin), degree of stenosis (DOS), the hyperintensity of T1WI (T1high), plaque enhancement (PE) and normal wall index (NWI). ASPECTS scored on DWI and divided into high score (≤7)and low score (<7). Normally distributed continuous variables were compared by Student’s t-test. Non-normally distributed continuous variables were verified by Mann-Whitney U test. Categorical variables were assessed by chi-square test. Area under the curves (AUCs), specificity, sensitivity and optimal cut-off values were analyzed by receiver-operating characteristic (ROC) curve.Result
There were 29 patients in the good response group (53.45±11.08 years,69.0% male) and 14 patients in the poor response group (59.36±8.46 years,64.3% male). Compared with the good response group, the poor response group had higher prevalence of diabetes, lower ASPECTS, lower Vmin, higher DOS, more T1high, higher PE and higher NWI (all P<0.05, Table1). In ROC analysis, NWI, DOS, Vmin, PE, T1high and ASPECTS showed significant predicting value between good and poor response groups with AUC of 0.828, 0.776, 0.740, 0.746, 0.702, 0.697 separately (all P<0.05) (Figure 2, Table 2). When combined HR-VWI and ASPECTS, the AUC increased to 0.956 (95%CI 0.845 to 0.995) with sensitivity and specificity represented 0.929 and 0.862, respectively (Table 2). In Delong test, there was difference in the above characteristics of HR-VWI, ASPECTS and the combination of HR-VWI and ASPECTS (all P<0.05).Discussion
In this study, ASPECTS, NWI, DOS, Vmin, PE and the T1high were predictive parameters for the response with ACI patients, which was consistent with previous study3,4. ASPECTS score<7 was associated with poor response which represents early cytotoxic oedema and possibly the development of irreversible injury6,7. Stenosis caused by atherosclerotic plaque is negatively correlated with the perfusion state and blood flow acceleration of distal brain tissue, which leads to an increased risk of plaque rupture due to lumen shrinkage, further affects the response of patients5. PE is related to vascular endothelial permeability and inflammatory response caused by neovascularization, which may increase the risk of plaque rupture and progression. T1high is associated with intraplaque hemorrhage (IPH) and large intraplaque lipid cores. Plaque progression, characterized by increased lipid core volume, fibrous cap, and IPH, is often associated with stroke recurrence[3]. Studies have illustrated that an independent relationship between hyperintensity on T1WI in middle cerebral artery plaques and recurrence in stroke patients for 6 months8. Furthermore, recurrence of infarction often leads to more severe infarcts with the improve of mortality rate.Conclusions
The combination HR-VWI and clinical evaluation score of ASPECTS showed significantly predicted value in the outcome of ACI patients. To improve the risk stratification and therapeutic management for patients, comprehensive vascular examinations should be systematically performed.Acknowledgements
No acknowledgement found.References
1. Hou Z, Zhang Z, Yan L, et al. Association of residual stenosis after balloon angioplasty with vessel wall geometries in intracranial atherosclerosis. J Neurointerv Surg. 2022;14(8):762-766. doi:10.1136/neurintsurg-2021-017997
2. Li F, Wang Y, Hu T, Wu Y. Application and interpretation of vessel wall magnetic resonance imaging for intracranial atherosclerosis: a narrative review. Ann Transl Med. 2022;10(12):714. doi:10.21037/atm-22-2364
3. Jiang H, Ren K, Li T, et al. Correlation of the characteristics of symptomatic intracranial atherosclerotic plaques with stroke types and risk of stroke recurrence: a cohort study. Ann Transl Med. 2022;10(12):658. doi:10.21037/atm-22-2586
4. Li S, Tang M, Zhang D, et al. The prevalence and prognosis of asymptomatic intracranial atherosclerosis in a community-based population: Results based on high-resolution magnetic resonance imaging [published online ahead of print, 2023 Sep 22]. Eur J Neurol. 2023;10.1111/ene.16057. doi:10.1111/ene.16057
5. Ren K, Jiang H, Li T, et al. Predictive value of the combination between the intracranial arterial culprit plaque characteristics and the Essen Stroke Risk Score for short-term stroke recurrence [published correction appears in J Stroke Cerebrovasc Dis. 2022 Dec;31(12):106793]. J Stroke Cerebrovasc Dis. 2022;31(9):106624. doi:10.1016/j.jstrokecerebrovasdis.2022.106624
6. Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score [published correction appears in Lancet 2000 Jun 17;355(9221):2170]. Lancet. 2000;355(9216):1670-1674. doi:10.1016/s0140-6736(00)02237-6
7. Xu XQ, Chu Y, Shen GC, et al. Prognostic value of ASPECTS on post-treatment diffusion-weighted imaging for acute ischemic stroke patients after endovascular thrombectomy: comparison with infarction volume. Eur Radiol. 2022;32(12):8079-8088. doi:10.1007/s00330-022-08888-z
8. Li X, Liu C, Zhu L, et al. The Role of High-Resolution Magnetic Resonance Imaging in Cerebrovascular Disease: A Narrative Review. Brain Sci. 2023;13(4):677. Published 2023 Apr 18. doi:10.3390/brainsci13040677
9. Bruno A, Close B, Switzer JA, et al. Simplified modified Rankin Scale questionnaire correlates with stroke severity. Clin Rehabil. 2013;27(8):724-727. doi:10.1177/0269215512470674
Figures
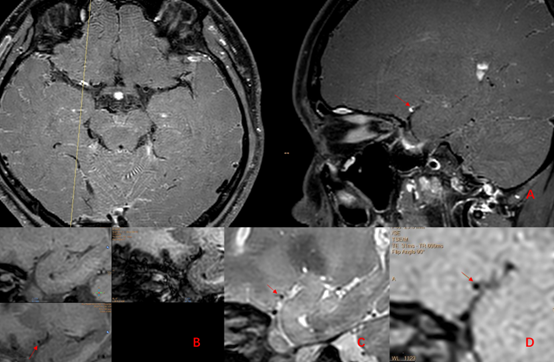
Figure 1:(A)contrast-enhanced T1-weighted imaging;(B)SNAP imaging; (C)T2-weighted imaging;(D) T1-weighted imaging
[The red arrow indicates the location of plaque.]
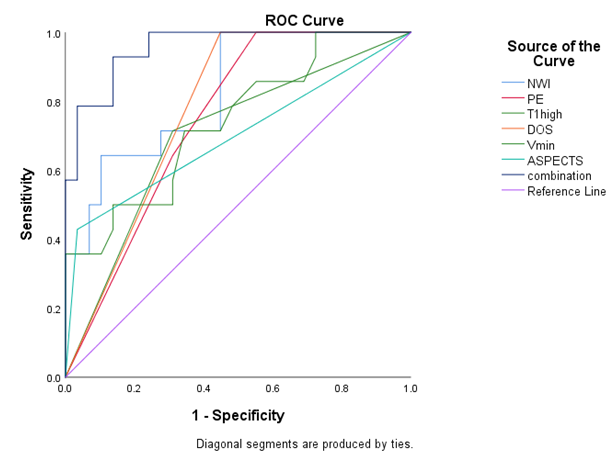
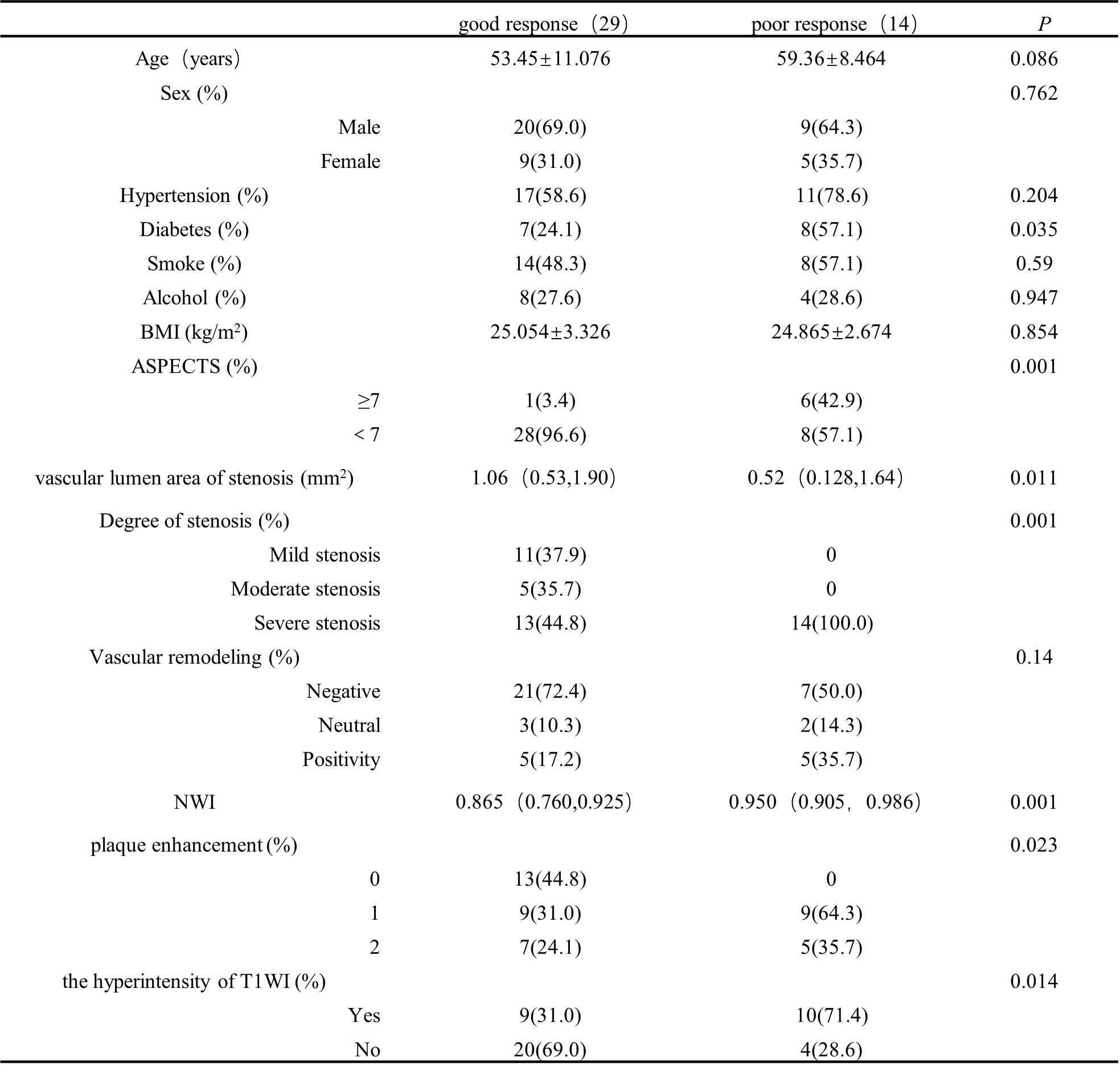
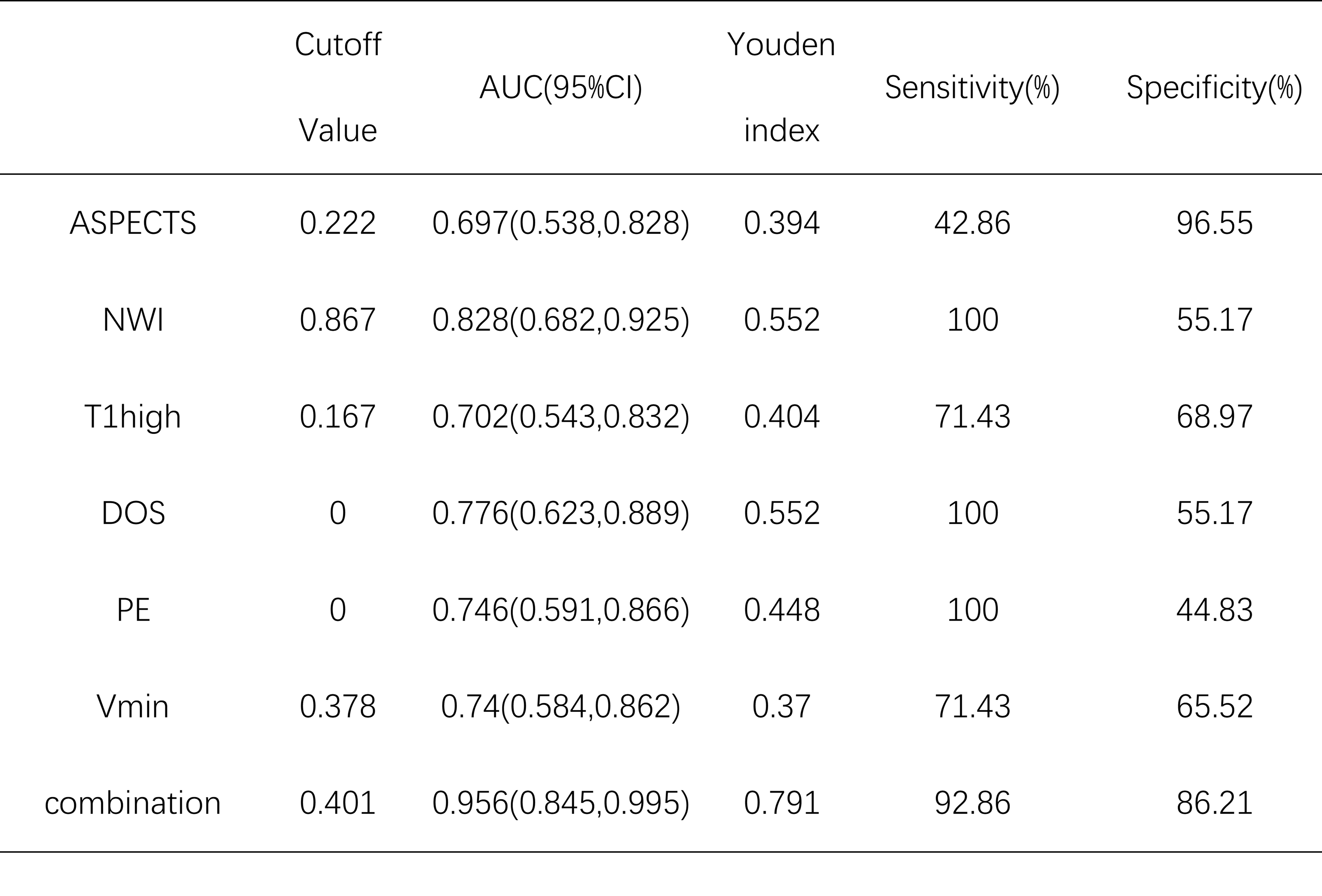
Table 2: Predictive power of prediction model on prognosis.
NWI: normalized wall index, T1high: hyperintensity of T1WI, DOS: degree of stenosis, PE: plaque enhancement, Vmin: vascular lumen area of stenosis