0075
Nomogram to predict hemorrhagic transformation using arterial spin labeling MRI in acute ischemic stroke with mechanical endovascular therapy1Guangdong Provincial Hospital of Traditional Chinese Medicine, guangzhou, China, 2nanfang hospital, guangzhou, China, 3Philips Healthcare, guangzhou, China
Synopsis
Keywords: Stroke, Arterial spin labelling
Motivation: Hemorrhagic transformation (HT) is the most severe complication of acute ischemic stroke.
Goal(s): The present study was to construct and internally validate a nomogram model based on pre-treatment arterial spin labeling (ASL) MRI to predict HT in AIS patients
Approach: This retrospective study enrolled 117 AIS patients with anterior circulation large vessel occlusion. Multivariate logistic regression analysis identified that baseline NIHSS, ADC value and pre-treatment ASL hyperperfusion were independent factors affecting HT. Those independent predictors were then incorporated to develop a predictive nomogram model.
Results: The nomogram model, could reliably calculated the probability of HT in AIS patients with mechanical endovascular therapy.
Impact: The prediction model has significant clinical implications, which could guide clinical screening of high-risk patients and develop more targeted prevention strategies.
Introduction
Hemorrhagic transformation (HT) is the most severe complication of acute ischemic stroke after mechanical thrombectomy [1]. Previous computed tomography perfusion (CTP) and magnetic resonance imaging (MRI) with postcontrast T1 parenchymal enhancement have been proposed for the identification of BBB disruption to predict HT. However, the use of exogenous contrast agents restricted clinical applicability during urgent examinations. Arterial spin labeling (ASL) has been suggested as a regular MRI technique to assess cerebral blood flow (CBF) in AIS patients, without radiation and contrast agent administration [2]. Post-ischemic hyperperfusion, produced by collateral vessels on pre-treatment ASL maps, was associated with occurrence of HT in AIS patients. The aim of this study was to identify independent risk variables for HT, construct and internally validate a model based on pre-treatment ASL MRI to predict HT in AIS patients with mechanical endovascular therapy, and draw a nomogram of the model.Methods
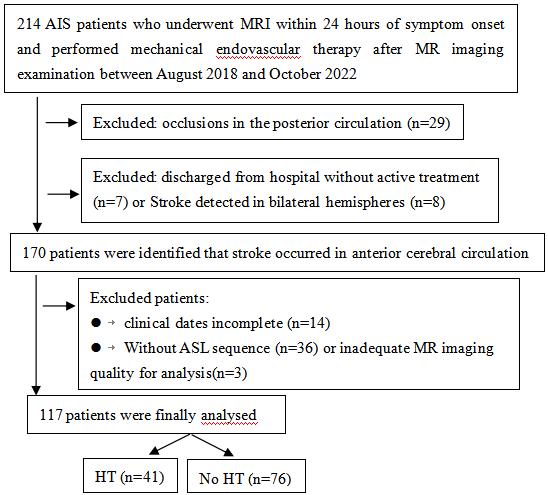
This retrospective study enrolled 117 AIS patients with anterior circulation large vessel occlusion within 24 hours of symptom onset before mechanical endovascular therapy (Fig. 1). All patients underwent conventional MRI scanning and ASL images were obtained with a pseudo-continuous ASL pulse sequence with the following parameters: TR of 4521ms, TE of 9.8 ms, label time of 1500 ms, post label delay of 1525 ms, field-of-view of 240×240 mm2,slice thickness 4mm, scan time 3 min 10 s. Hyperperfusion was characterized as patchy patches with visually discernible increased CBF on ASL maps inside and/or surrounding the hypoperfused area when compared with the homologous contralateral hemisphere and it was distinguished from arterial transit artifacts observed on proximal normal vascular structures of occlusion. A region with relative cerebral blood flow (CBF) ≥1.4 was defined as hyperperfusion [3]. A noncontrast CT scan performed during the subacute phase after mechanical endovascular therapy for the evaluation of HT.Included patients were randomly assigned into two cohorts (6.5 : 3.5): the training cohort and the validation cohort. Variables with p < 0.05 in the univariate logistic analysis were included in the multivariablelogistic regression analysis using a backward stepwise method to eliminate nonsignificant variables. Receiver operating characteristics (ROC) curves were drawn to assess the area under the curve (AUC). The cutoff point was selected by using the maximized values of Youden indexes, and sensitivity and specificity at the threshold value were determined. We used the AUC-ROC to assess the discrimination of the prediction model.Results
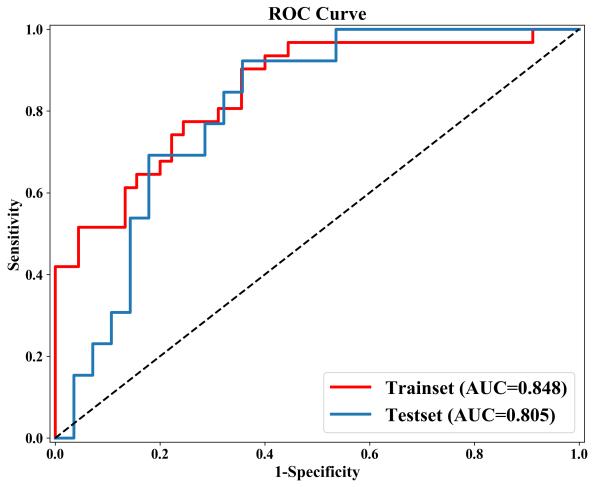
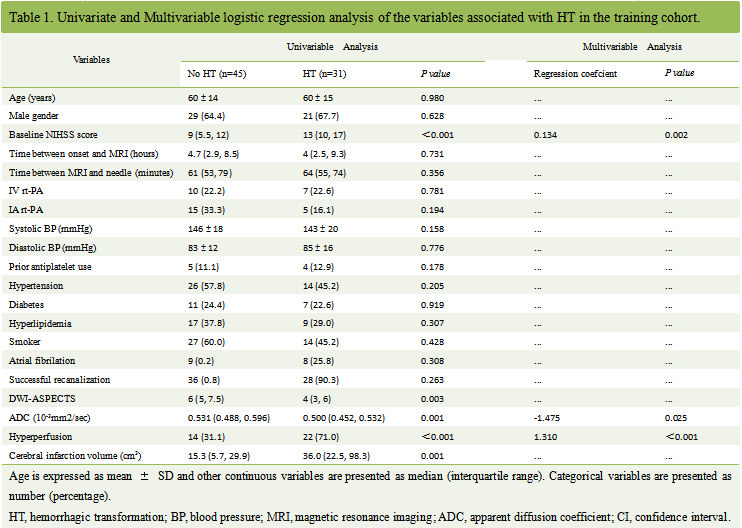
117 patients with AIS in total met the criteria for inclusion. 101 (86%) patients experienced successful recanalization. HT occurred in 44 (39%) patients. ASL hyperperfusion was detected in 57 (48%) patients. A multivariate logistic regression analysis identified that baseline NIHSS, ADC value and ASL hyperperfusion were independent predictive factors affecting HT (Table 1). The regression coefcient of baseline NIHSS, ADC value and ASL hyperperfusion were 0.134, -1.475 and 1.310, respectively . The AUC-ROC of the model in training cohort was 0.848 (95% CI, 0.747-0.920); the accuracy, sensitivity and specificity were 0.750, 0.645 and 0.822, respectively (Fig. 2). The calibration of the model was good ( p = 0.820 for the Hosmer-Lemeshow test). In the validation cohort, the AUC-ROC value was 0.805 (95% CI, 0.651-0.912) (Fig. 2); the accuracy, sensitivity and specificity were 0.707, 0.769 and 0.678, respectively.Discussion
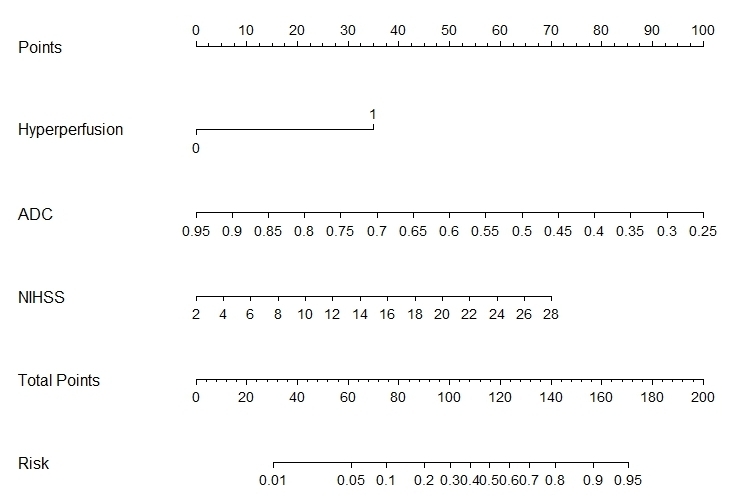
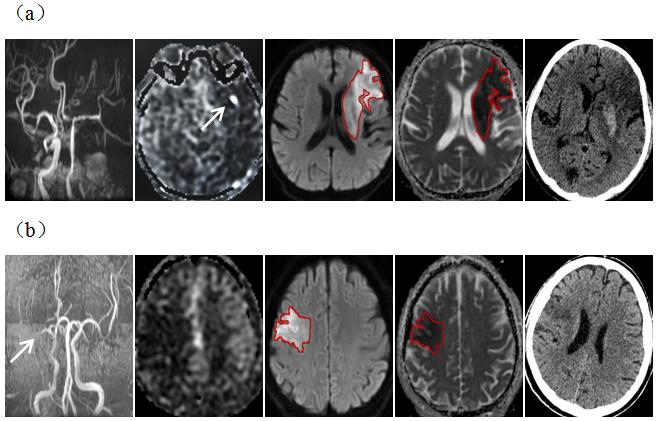
In this study, We found three easy-to-assess variables based on baseline NHISS, ADC value and pre-treatment ASL hyperperfusion for clinical professionals to predict the occurrence of HT after acute ischemic stroke (Fig. 3). The model performs well in predicting the risk of HT in acute ischemic stroke patients (Fig. 4 show representative cases) and the calibration curve exhibited good fit, and internal validation in the model revealed good discrimination. Unlike those studies that focused on clinical factors and intravenous thrombolysis [4-5], this study focused on radiologic features based on ASL MRI examination and patients with mechanical endovascular therapy. We evaluated the pre-treatment ASL flow perfusion images of all included AIS patients. The results showed that the presence of pre-treatment ASL hyperperfusion was significantly correlated with the incidence of HT, which corresponded with previous studies [3]. To our knowledge, this is the first prediction model that enrolled pre-treatment ASL hyperperfusion to predict HT in AIS patients with mechanical endovascular therapy. The prediction model has significant clinical implications, which could perhaps enable timely intervention to prevent PH, a lesion that is associated with poor outcome.Conclusions
We proposed and validated a nomogram model, included NHISS, ADC value and pre-treatment ASL hyperperfusion, could reliably calculated the probability of HT, and had good predictive ability in AIS patients with mechanical endovascular therapy.Acknowledgements
The authors thank the Department of Medical Imaging Center, Nanfang Hospital for providing MR images of acute ischemic stroke patients for this studyReferences
1. Nguyen T, Lefevre J, Kanagaratnam L et al (2022) ADC measurement relevance to predict hemorrhage transformation after mechanical thrombectomy. Journal of the Neurological Sciences 441:1203702.
2. Lu SS, Cao YZ, Su CQ et al (2021) Hyperperfusion on Arterial Spin Labeling MRI Predicts the 90-Day Functional Outcome After Mechanical Thrombectomy in Ischemic Stroke. Journal of Magnetic Resonance Imaging 53:1815-18223.
3. Niibo T, Ohta H, Miyata S, Ikushima I, Yonenaga K, Takeshima H (2017) Prediction of Blood-Brain Barrier Disruption and Intracerebral Hemorrhagic Infarction Using Arterial Spin-Labeling Magnetic Resonance Imaging. Stroke 48:117-1224.
4. Cappellari M, Mangiafico S, Saia V, et al. IER-SICH Nomogram to Predict Symptomatic Intracerebral Hemorrhage After Thrombectomy for Stroke[J]. Stroke, 2019,50(4):909-916.5.
5. Wu Y, Chen H, Liu X et al (2020) A new nomogram for individualized prediction of the probability of hemorrhagic transformation after intravenous thrombolysis for ischemic stroke patients. BMC Neurology 20:426.
Figures