0074
Prediction of Long-term Motor Function Based on Functional Connectivity in Ischemic Stroke after Intra-arterial Thrombectomy1Department of Biomedical Imaging and Radiological Sciences, National Yang Ming Chiao Tung University, Taipei, Taiwan, 2Department of Radiology, Far Eastern Memorial Hospital, New Taipei City, Taiwan, 3Department of Neurology, Far Eastern Memorial Hospital, New Taipei City, Taiwan
Synopsis
Keywords: Stroke, Brain Connectivity
Motivation: Intra-arterial thrombectomy (IAT) can remove the thrombus to restore cerebral blood flow. However, even if the thrombus is removed, the experienced hypoxia may still damage the brain, resulting in motor deficits.
Goal(s): This study demonstrated that early brain network changes after IAT treatment can predict long-term recovery in ischemic stroke patients.
Approach: Functional connectivity was correlated with motor recovery after IAT treatment, identifying key functional connectivity features that influence stroke prognosis to unravel the involved mechanisms.
Results: Long-term motor functions can be predicted based on the two-week functional connectivity and Fugl-Meyer Assessment scores.
Impact: The current clinical challenge is that nearly half of stroke patients who undergo IAT still cannot fully recover after treatment and rehabilitation. Early prediction of post-IAT motor recovery in stroke patients can provide appropriate rehabilitation plans in clinics.
Background and Purpose
The current standard clinical treatment of acute ischemic stroke involves the administration of an intravenous-injected recombinant tissue plasminogen activator (rt-PA) within three hours after stroke onset[1]. However, rt-PA is less effective in thrombolysis of large arteries, with a recanalization rate of only 10% to 20%[2]. Therefore, it is recommended to perform intra-arterial thrombectomy (IAT) on stroke patients with a large artery occlusion in anterior circulation infarction to enhance the chances of vascular recanalization[3]. The level of post-stroke motor recovery is highly associated with the integrity of brain functions. We anticipated that functional connectivity (FC) may predict long-term motor recovery after IAT.Materials and Methods
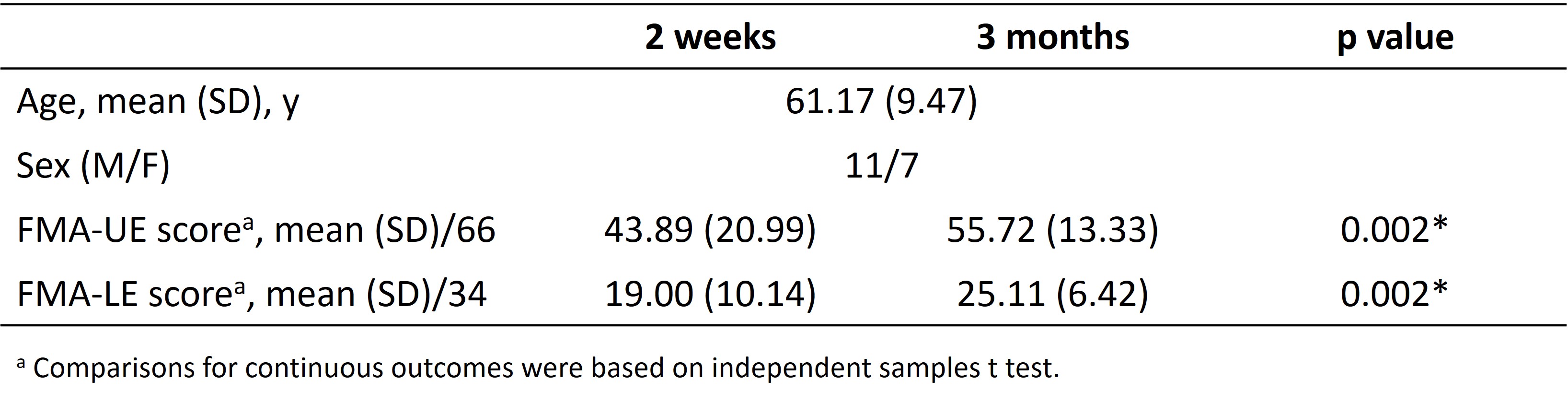
This study was approved by the local Institutional Review Board, and the written informed consent was provided by each participant. Eighteen acute ischemic stroke patients with large vascular occlusion, who underwent IAT within twenty-four hours of stroke onset, were recruited. All patients underwent the assessment of motor function using the Fugl-Meyer Assessment (FMA) at two weeks and three months after stroke onset. FMA is an assessment scale for motor functions and provides a reliable measurement of motor recovery in stroke patients. This scale assesses different aspects of recovery for upper and lower limbs, including the motor function, sensation, passive joint motion, and joint pain. MRI data, including 3D-MPRAGE T1-weighted images (TR/TE: 2060/2.3 ms; voxel size: 0.9x0.9x0.9 mm3) and BOLD resting-state fMRI (TR/TE: 2000/24 ms; voxel size: 3x3x4 mm3, 190 volumes) were acquired on a 3T MR scanner (Siemens Magnetom Skyra). Each patient received twice MRI scans at two weeks and three months after IAT treatment to evaluate the changes of brain functional networks. The fMRI data were preprocessed using SPM12 with the standard procedures: corrected for slice timing, realigned, co-registered with structural images, spatially normalized into the standard space, and spatially smoothed with a 6-mm FWHM Gaussian kernel. Independent Component Analysis (ICA) was conducted to decompose the functional networks into 25 components. Among these components, the cerebellar network and sensorimotor network were selected to evaluate the changes between two weeks and three months after IAT treatment. Furthermore, the FC between motor-related regions in both hemispheres, including primary motor cortex, primary somatosensory cortex, supplementary motor area, dorsal premotor cortex, ventral premotor cortex, and intraparietal sulcus, was calculated from the functional data. The correlation analysis (|r|>0.5, p<0.05) between the changed score of FMA (3 months – 2 weeks) and FC was performed. A stepwise linear regression model was established based on two-week FMA and FC to predict long-term (three-month) FMA. The performance of linear regression models was evaluated by the goodness-of-fit (R-square, R2) and F statistic versus a constant model (with p < 0.05 as a significance).Results and Discussion
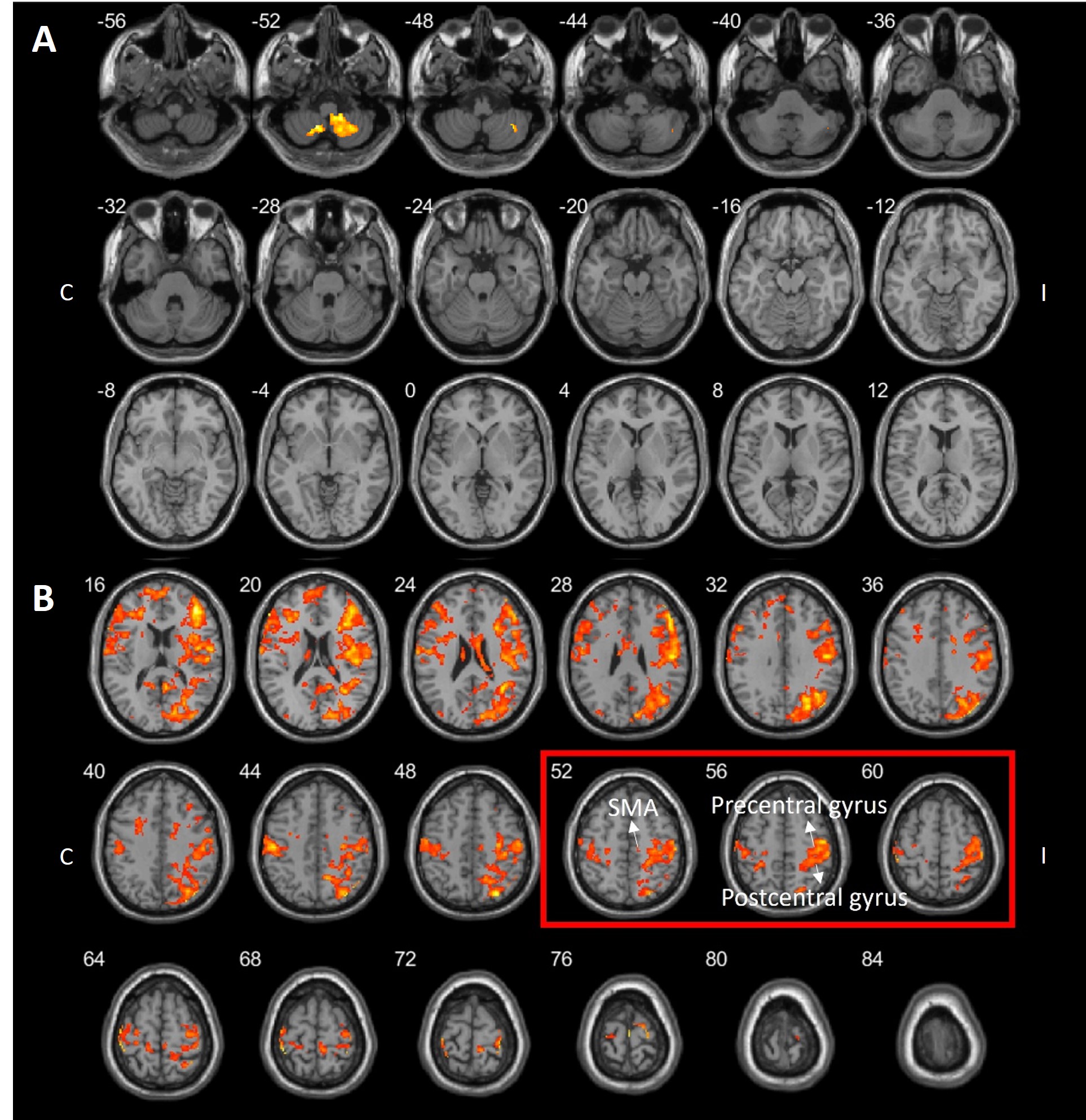
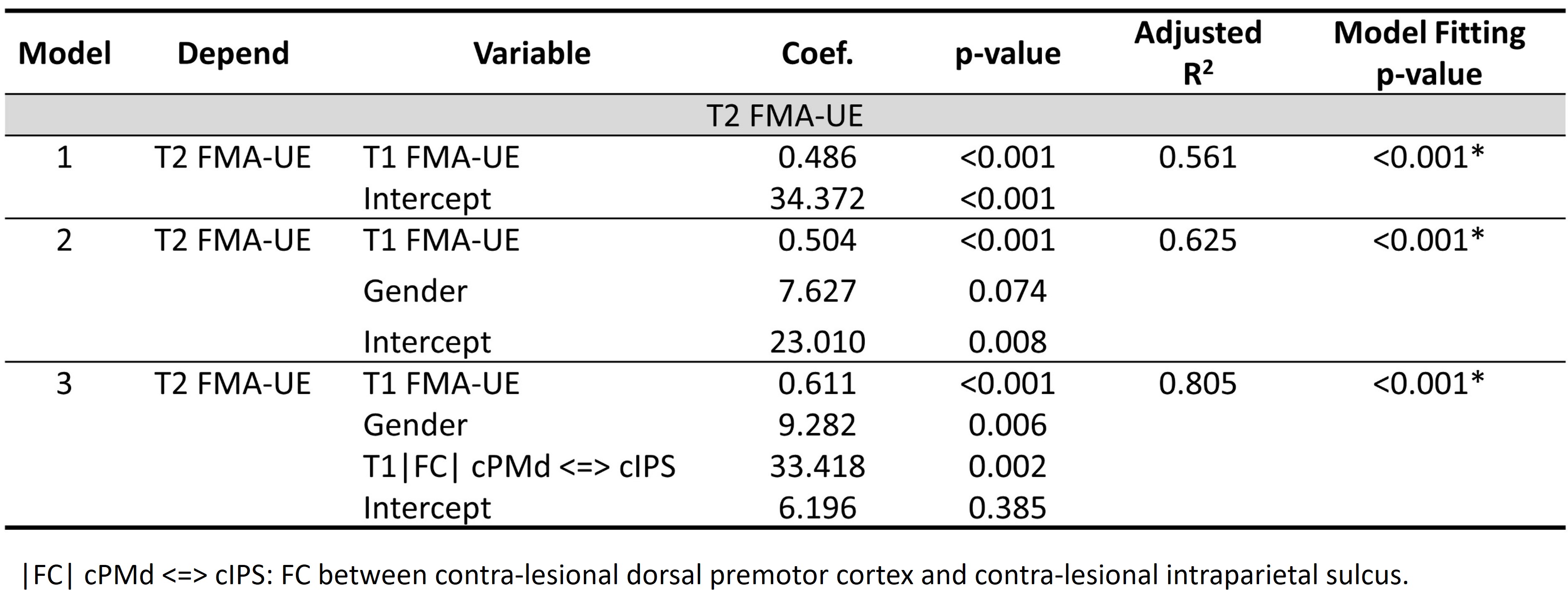
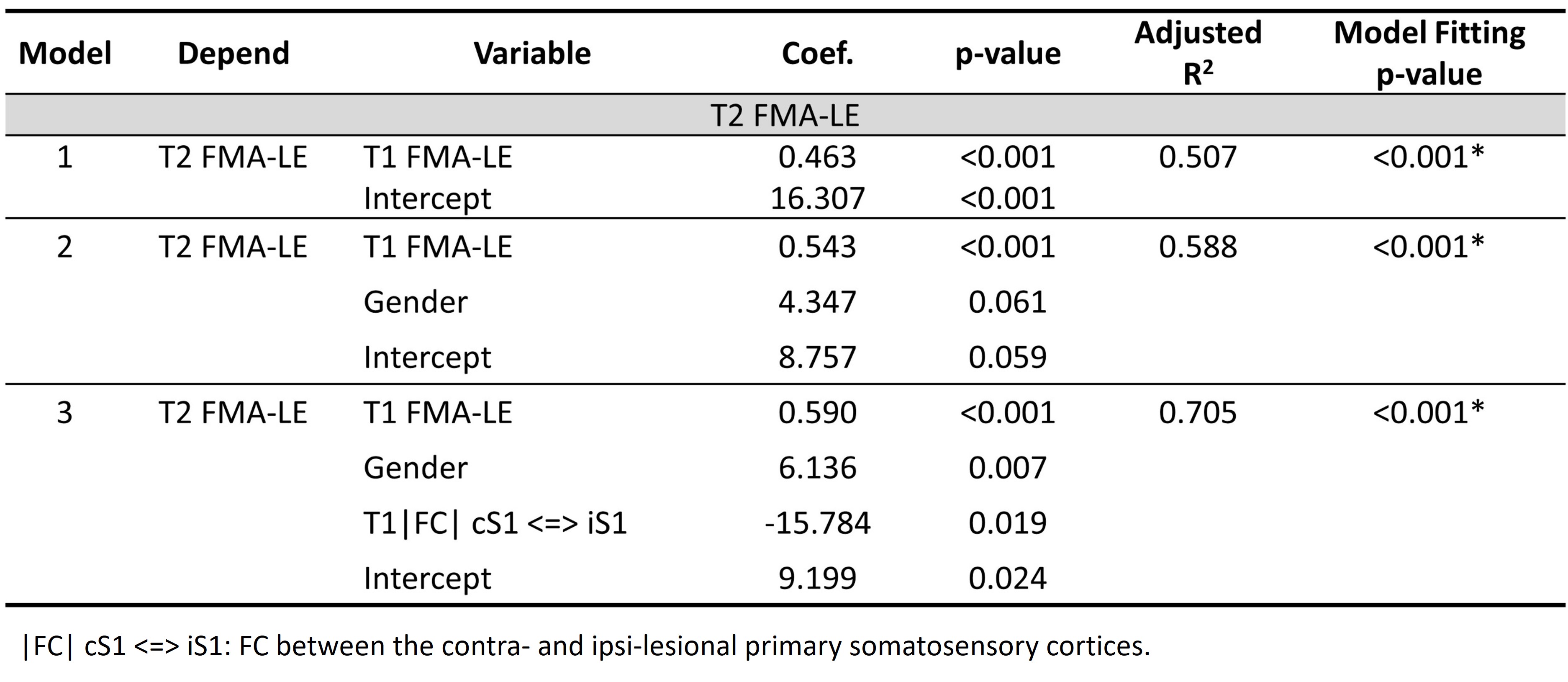
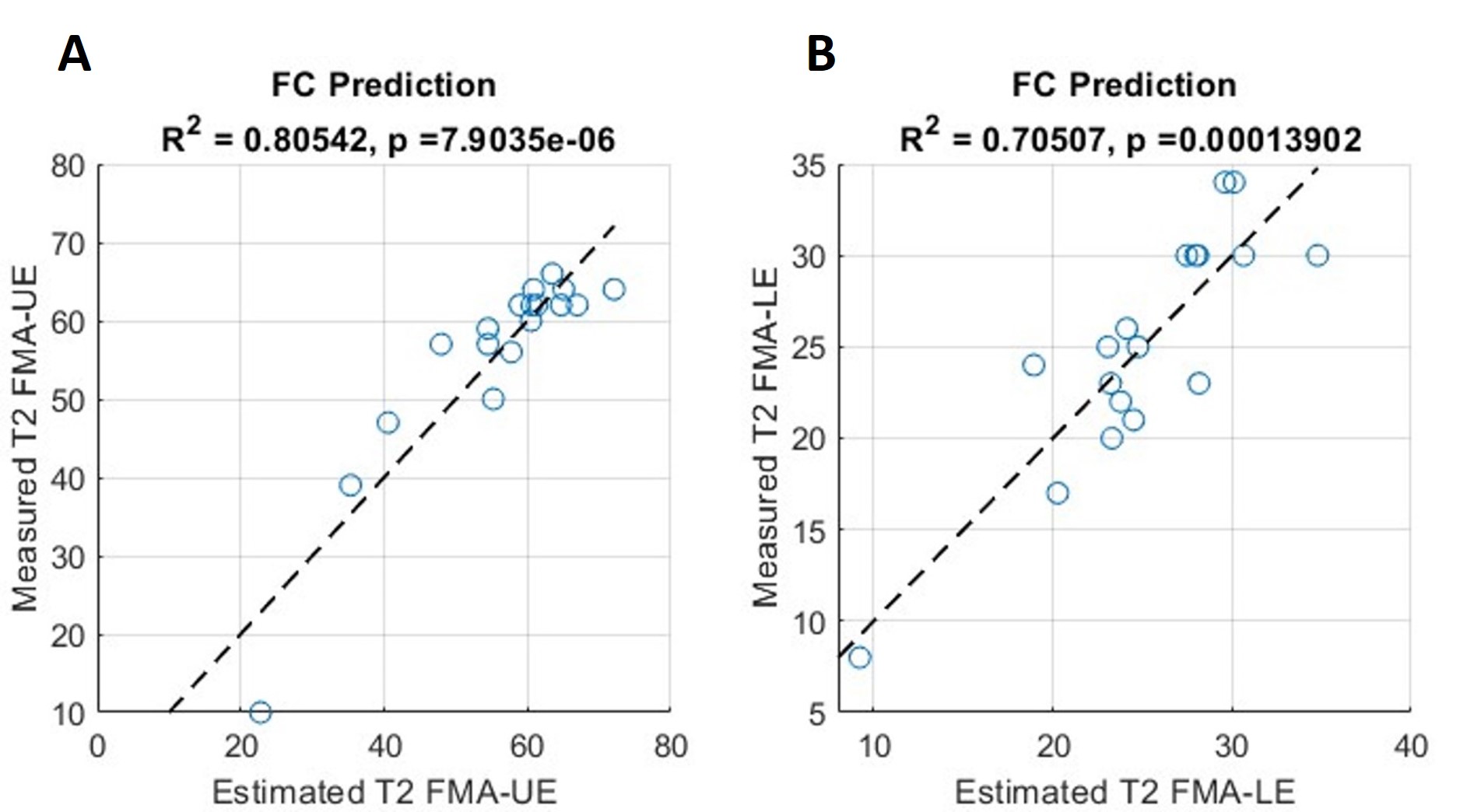
Table 1 lists the demographic data and FMA of the recruited patients at two time points. A significant improvement was observed in motor function at three months compared to two weeks after IAT (p=0.002). The results were consistent with previous studies that IAT can assist ischemic stroke patients in achieving a better functional outcome[3]. Figure 1A and Figure 1B show the paired t-test results (p<0.05 and cluster size ≥30 with false discovery rate (FDR) correction) for the cerebellar network and sensorimotor network, respectively, between two weeks and three months. Strength of network in the medial cerebellum (Figure 1A) and hand area of motor cortex (Figure 1B) significantly increased at three months compared to two weeks after IAT treatment. Besides, the ipsilesional motor cortex showed a significant increase in strength of network compared to contralesional motor cortex (Figure 1B). Table 2 demonstrates that FC between contra-lesional dorsal premotor cortex and contra-lesional intraparietal sulcus can increase the predictive performance of FMA-Upper Extremity (Model 3, adjusted R2=0.805). On the other hand, Table 3 shows that FC between the bilateral primary somatosensory cortices can increase the predictive performance (Model 3, adjusted R2=0.705) of the FMA-Lower Extremity. Figure 2A and Figure 2B demonstrate the stepwise linear regression models in predicting three-month FMA after treatment based on the two-week FC and FMA. These figures show that FC can enhance the long-term prediction of FMA-UE and FMA-LE after IAT.Conclusions
This study reported a significant increase in the strength of motor-related networks in three months after IAT treatment. Furthermore, long-term motor functions can be predicted based on the two-week FC and FMA.Acknowledgements
This work was supported by Far Eastern Memorial Hospital National Yang Ming Chiao Tung University Joint Research Program (111DN34), and National Science and Technology Council (NSTC 112-2314-B-A49-060).References
1. Hacke, W., et al., Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet, 2004. 363(9411): p. 768-74.
2. Wolpert, S.M., et al., Neuroradiologic evaluation of patients with acute stroke treated with recombinant tissue plasminogen activator. The rt-PA Acute Stroke Study Group. AJNR Am J Neuroradiol, 1993. 14(1): p. 3-13.
3. Roaldsen, M.B., et al., Endovascular thrombectomy and intra-arterial interventions for acute ischaemic stroke. Cochrane Database Syst Rev, 2021. 6(6): p. CD007574.
Figures