0072
Assessment of collateral flow in patients with carotid stenosis using random vessel-encoded arterial spin labeling1Radiology, The first affiliated hospital of Nanjing medical university, Nanjing, China, 2Radiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 3Interventional Radiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 4Radiology, Feinberg School of Medicine, Northwestern University, Evanston, IL, United States
Synopsis
Keywords: Stroke, Perfusion
Motivation: The ability to characterize collateral flows is crucial for evaluating patients with steno-occlusive internal carotid artery disease (ICAD). A random vessel-encoded ASL (rVE-ASL) has been introduced as a non-invasive approach for mapping vascular territories.
Goal(s): In this study, we evaluated the feasibility of using a planning-free rVE-ASL to assess collateral flows in patients with ICAD by taking DSA as the golden standard.
Approach: Prospective, case-control study.
Results: rVE-ASL provides comparable information with DSA in determining the presence and the extent of collateral flows. The presence of flow alterations in the territory of middle cerebral artery may be attributed to symptomatic ICAD.
Impact: Our study emphasized the clinical utility of a planning-free random vessel-encoded ASL (rVE-ASL) as a non-invasive tool for characterizing individual collateral pathways and its potential role in predicting and managing symptomatic patients with ICAD.
Introduction
Collateral circulation plays an important role in steno-occlusive internal carotid artery disease (ICAD) to reduce the risk of stroke1. Digital subtraction angiography (DSA) remains the gold standard to assess collateral circulation. However, this procedure is invasive and bears the risk of neurological complications and ionizing radiation2. A random vessel-encoded ASL (rVE-ASL) has been introduced as a non-invasive approach for mapping vascular territories3. We aimed to investigate the utility of a planning-free rVE-ASL in assessing collateral flows in patients with ICAD.Methods
We prospectively recruited 40 patients with ICAD and presenting with internal carotid artery (ICA) stenosis (≥ 50%) or occlusion on noninvasive imaging (computed tomography angiography, magnetic resonance angiography or ultrasonography) who underwent DSA for further evaluation. Those patients either suffered from recent neurologic events (acute ischemic stroke or transit ischemic attack) or non-specific neurological symptoms like dizziness and headache. The presence and extent of collateral flow were assessed and compared between rVE-ASL and digital subtraction angiography (DSA) using Contingency (C) and Cramer’s V (V) coefficients. The differences in flow territory alterations stratified by stenosis ratio and symptoms, respectively, were compared between symptomatic (n = 19) and asymptomatic (n = 21) patients using Fisher’s exact test.Results
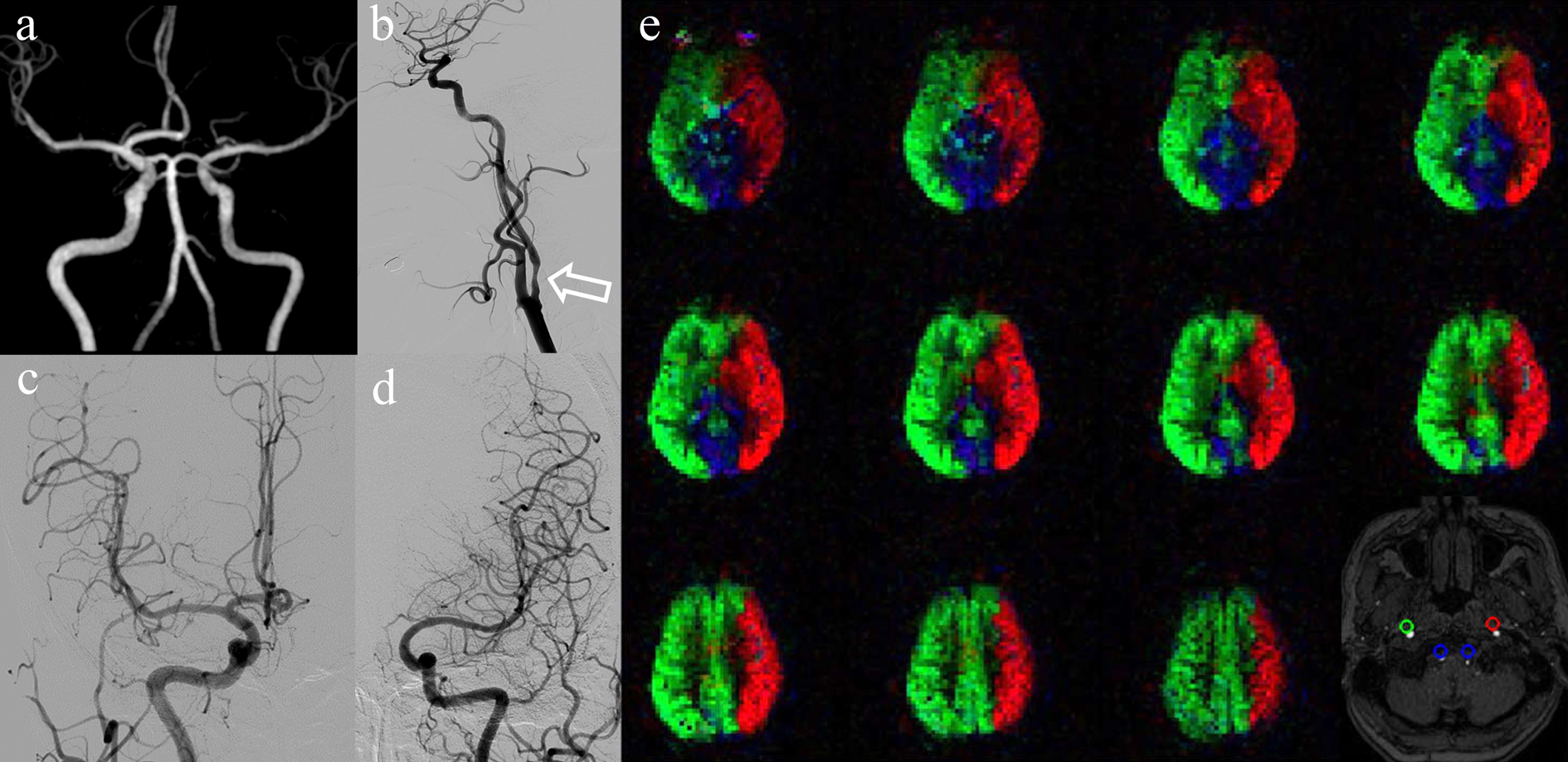
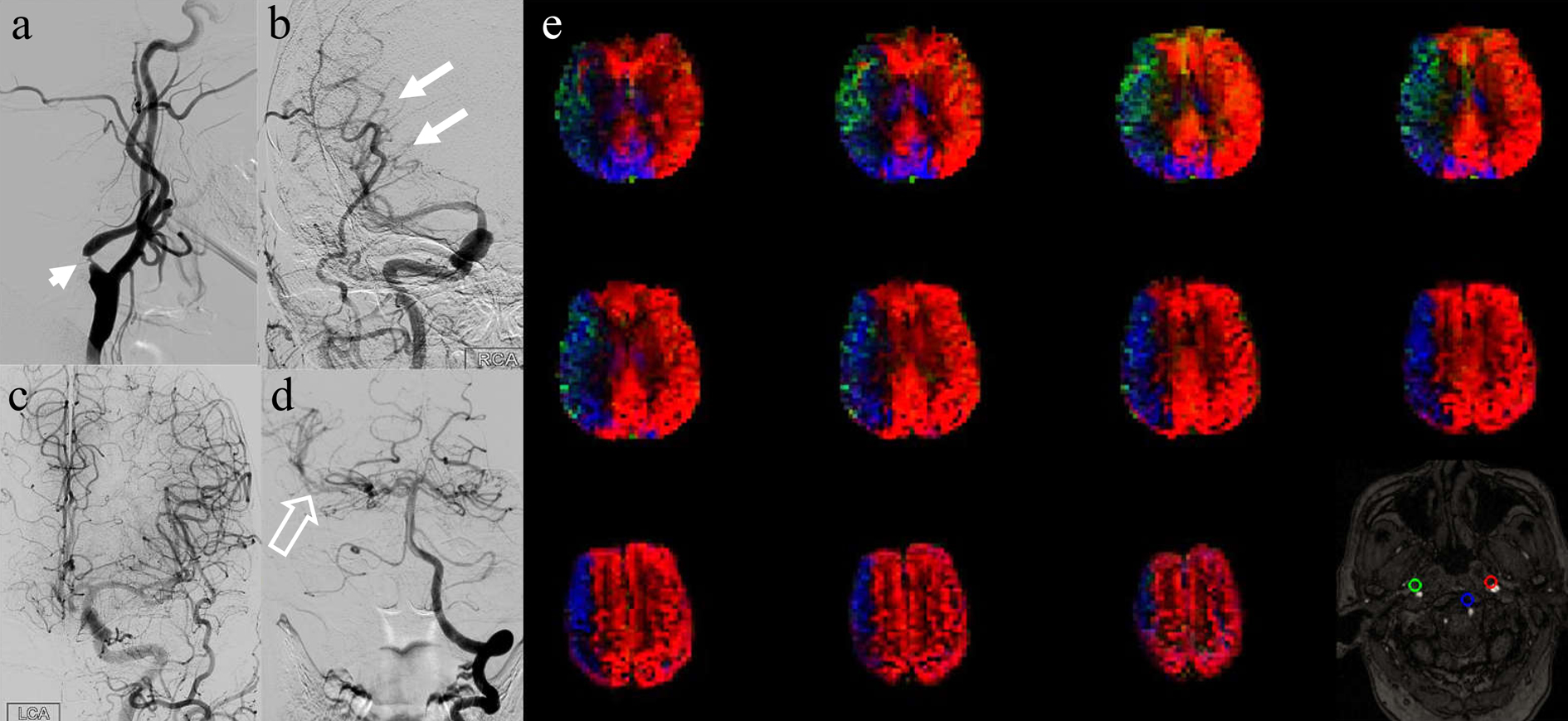
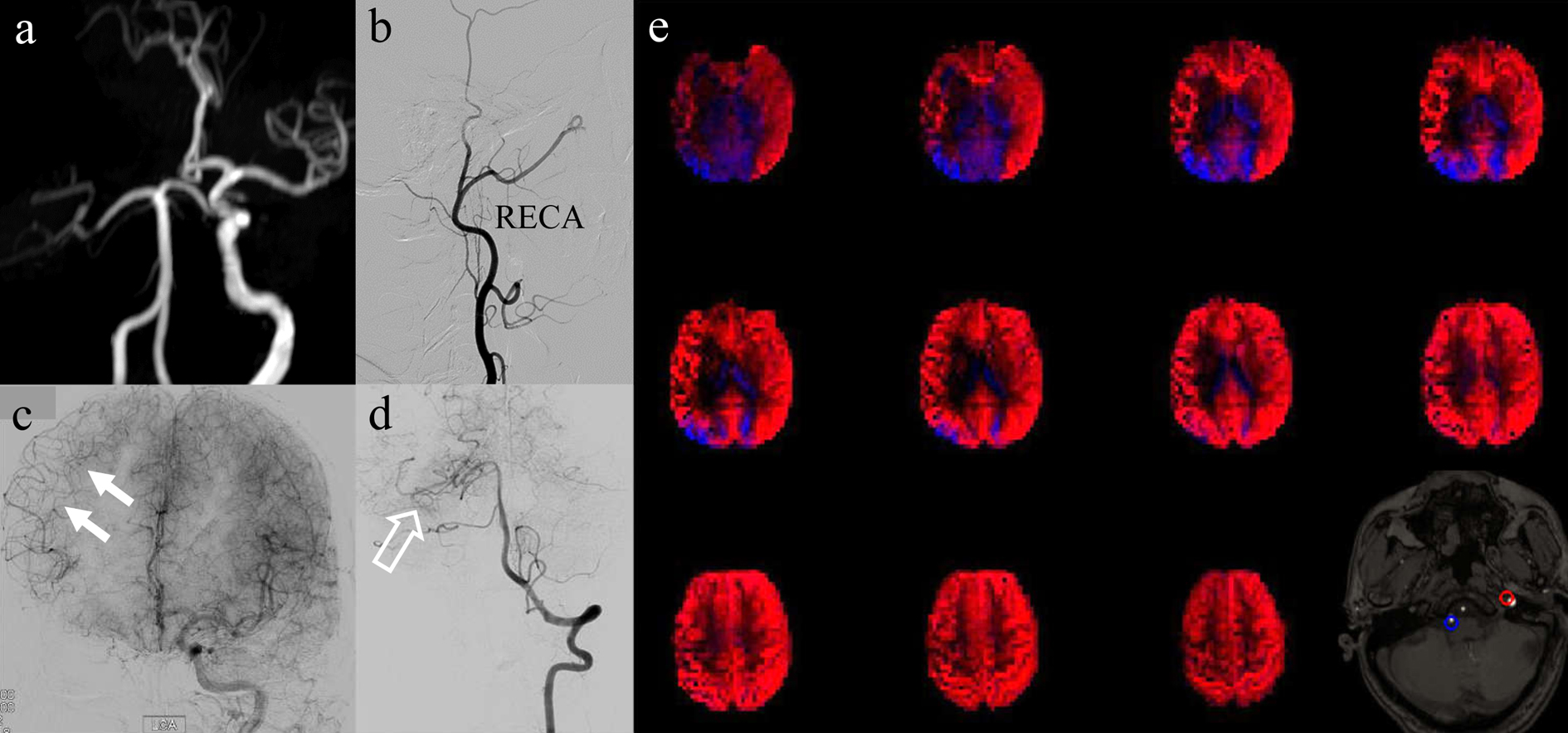
Good agreement was observed between rVE-ASL and DSA in assessing collateral flow (C = 0.762, V = 0.833, both p < 0.001). Patients with ICA stenosis of ≥ 90% were more likely to have flow alterations (p < 0.001). Symptomatic patients showed a higher prevalence of flow alterations in the territory of middle cerebral artery (MCA) on the same side of ICAD (63.2%), compared to asymptomatic patients (23.8%, p = 0.012), while the flow alterations in the territory of anterior cerebral artery (ACA) did not differ (p = 0.442). The collateral flow to MCA territory was developed primarily from the contralateral internal carotid artery (70.6%) and vertebral-basal artery (VBA) to a lesser extent (47.1%).Discussion
Conventional vessel-selective ASL techniques require prior knowledge of the locations of vessels to be tagged. This in turn necessitates a collection of an angiogram and expertise in planning4,5. The rVE-ASL used in our study can not only map vascular territories without the need for explicit planning but also identify the locations of corresponding source arteries in the tagging plane. This simplifies the scan procedure similar to conventional pseudo-continuous ASL (pCASL). In the conventional vessel-selective ASL based on pCASL, potential off-resonance at the locations of the arteries in the tagging plane can significantly impact the tagging efficiency. In contrast, rVE-ASL is insensitivity to off-resonance effects similar to multiphase pCAS3. Our study demonstrated a high consistency between vascular territory mapping using rVE-ASL and DSA, indicating that rVE-ASL could serve as an alternative and non-invasive method to evaluate individual collateral pathways in patients with ICAD.We observed that symptomatic patients with ICAD had a higher prevalence of flow alterations in the MCA territory on the affected side, compared to asymptomatic patients. The collateral flow to the MCA territory on the side of ICAD was primarily developed from the contralateral ICA (70.6% via Acom) and, to a lesser extent, from the VBA (47.1% via Pcom). Such results emphasized the importance of collateral flow from the contralateral ICA in maintaining blood flow in the MCA territory on the side of ICAD. In symptomatic patients without flow alteration, inadequate collateral compensation may lead to an occurrence of ischemic stroke event6,7.
We also revealed a significant association between flow alterations and the degree of stenosis. A high-grade ICA stenosis (≥ 90%) was most likely to result in flow alterations. Traditionally, the stenotic rate of ICA ≥ 70% is considered an indicator of hemodynamic impairment. However, our study indicates that patients with high-grade ICA stenosis could remain asymptomatic despite exhibiting flow alterations. These findings suggest that changes in flow territory may occur before CBF deficits manifest, and adequate compensating collateral flow may protect patients from the deterioration of clinical symptoms. Flow assessment by rVE-ASL can demonstrate the redistribution of CBF from the contralateral ICA and VBA, reflecting compensating patterns and the presence of collateral pathways in patients with ICAD, and may help predict the border zone prone to infarction.
Acknowledgements
No acknowledgement found.References
1. Liebeskind DS. Collateral circulation. Stroke 2003;34(9):2279-2284.
2. Kaufmann TJ, Huston J, 3rd, Mandrekar JN, Schleck CD, Thielen KR, Kallmes DF. Complications of diagnostic cerebral angiography: evaluation of 19,826 consecutive patients. Radiology 2007;243(3):812-819.
3. Wong EC, Guo J. Blind detection of vascular sources and territories using random vessel encoded arterial spin labeling. MAGMA 2012;25(2):95-101.
4. Wong EC. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magn Reson Med 2007;58(6):1086-1091.
5. Okell TW, Garcia M, Chappell MA, Byrne JV, Jezzard P. Visualizing artery-specific blood flow patterns above the circle of Willis with vessel-encoded arterial spin labeling. Magn Reson Med 2019;81(3):1595-1604.
6. Fang H, Song B, Cheng B, et al. Compensatory patterns of collateral flow in stroke patients with unilateral and bilateral carotid stenosis. BMC Neurol 2016;16:39.
7. Hendrikse J, Hartkamp MJ, Hillen B, Mali WP, van der Grond J. Collateral ability of the circle of Willis in patients with unilateral internal carotid artery occlusion: border zone infarcts and clinical symptoms. Stroke 2001;32(12):2768-2773.
Figures