0070
Improved stratification for thrombectomy after acute ischemic stroke using personalized brain thermal modeling1Department of Biomedical Engineering, Georgia Institute of Technology and Emory University, Atlanta, GA, United States, 2Woodruff School of Mechanical Engineering, Georgia Institute of Technology, Atlanta, GA, United States, 3Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, IN, United States, 4Department of Radiology and Imaging Sciences, Emory University School of Medicine, Atlanta, GA, United States, 5Department of Neurology, Emory University School of Medicine, Atlanta, GA, United States, 6Petit Institute for Bioengineering and Bioscience, Georgia Institute of Technology, Atlanta, GA, United States
Synopsis
Keywords: Stroke, Stroke, Computational Model
Motivation: Prior research has demonstrated the benefits of thrombectomy after acute ischemic stroke (AIS). Despite improvements in surgical techniques, failed reperfusion after thrombectomy is problematic.
Goal(s): Our goal was to evaluate brain temperature-based identification of infarcted and salvageable tissue for improved stratification after AIS.
Approach: A patient-specific computational model using imaging data was used to predict local brain temperatures after AIS to identify infarcted and salvageable tissue and compared to existing clinical methods (RAPID).
Results: Temperature-based stratification identified infarct regions not observed with RAPID and predicted lower mismatch ratios more consistent with final clinical outcomes.
Impact: We demonstrate the potential for model-predicted brain temperatures to quantify infarcted and salvageable tissue after acute ischemic stroke for patient selection for thrombectomy. Local brain temperature may complement existing metrics, particularly for patients without sufficient salvageable tissue.
Introduction
Following an acute ischemic stroke (AIS), local brain temperature can increase due to regional hypoperfusion and inflammation.1-3 Current standard of care is intravenous injection of tissue plasminogen activator, followed by mechanical thrombectomy for large artery occlusion. Thrombectomy, which mechanically eliminates a blockage, is beneficial up to 24 hours after AIS onset.4,5 The recent SELECT2 trial reported thrombectomy is beneficial even for patients with large infarct volume (≥50mL) and small mismatch ratio (<1.8) with low incidence of intracranial hemorrhage;6 however, failed reperfusion after thrombectomy is reported and leads to complications.7,8 The goal of this study is to evaluate the use of brain temperature after AIS, calculated using a personalized computational model previously validated with chemical shift thermometry.9 We hypothesize local temperatures can effectively discriminate salvageable tissue from infarct after AIS.Methods
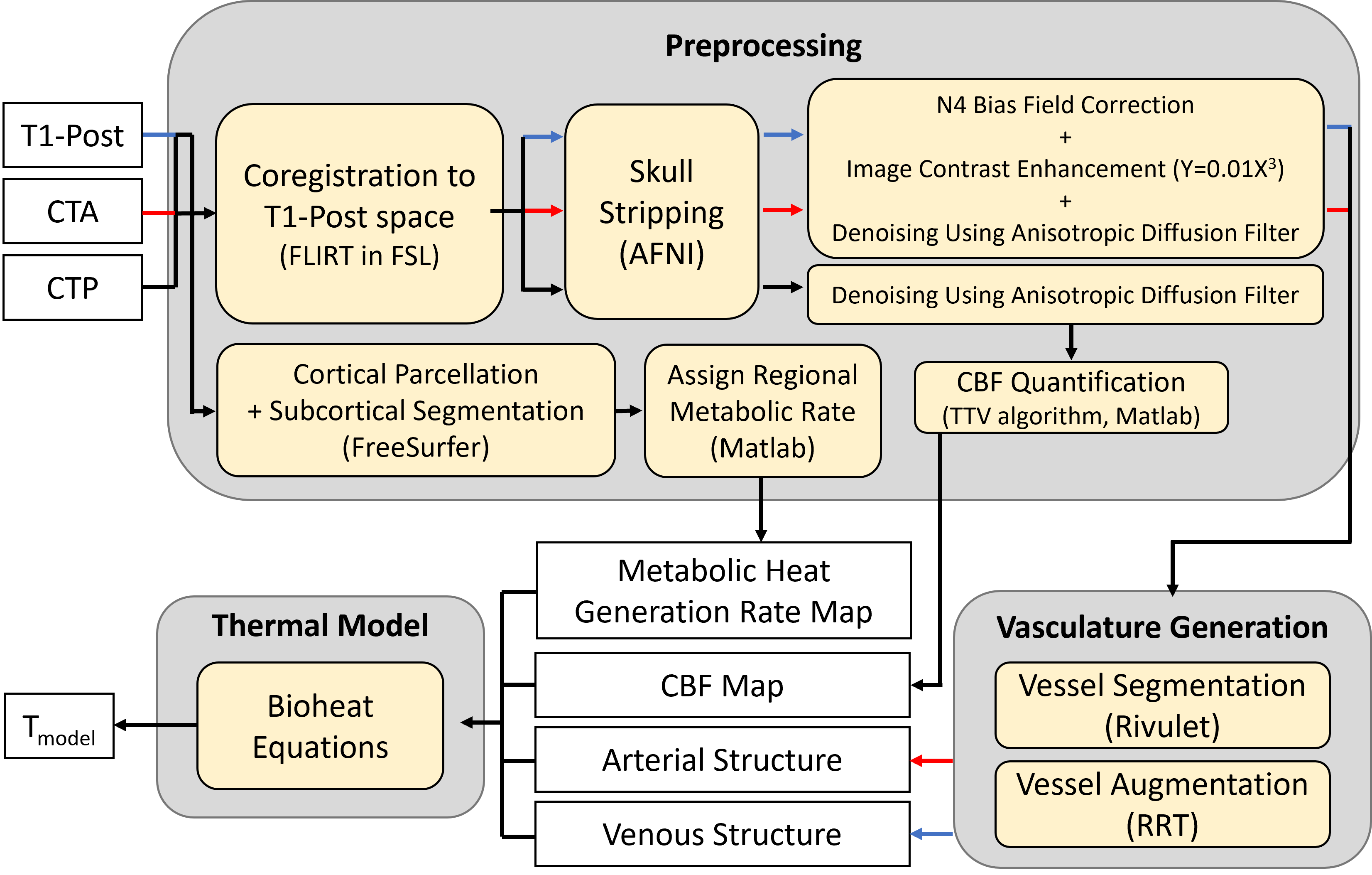
Following approval by the local institutional review board, MR and CT data were obtained retrospectively from four patients with unilateral large vessel occlusion and AIS (mean±standard deviation age=63±14 years old; three males, one female). Two patients received thrombectomy but had failed reperfusion [final thrombolysis in cerebral infarction (TICI) score=0]. The other two patients did not undergo thrombectomy as no infarct was observed from RAPID. CT data was acquired with a Discovery CT750 HD (GE Healthcare), and MR data using a 3T MR scanner (TIM Trio, Siemens Healthcare). Arterial structure was determined using helical CT angiography (CTA;120kVp;500mA;resolution=0.5×0.5×0.6mm3). Cerebral blood flow (CBF) was calculated from CT perfusion (CTP) data collected from 2 contiguous slabs (80kVp;145mA;pixel spacing=0.47×0.47mm2). Post-contrast T1-weighted magnetization-prepared rapid-gradient-echo images (TR/TI/TE=1900/900/2.52ms;flip angle (FA)=9°;resolution=1.0×1.0×1.0mm3) were used to define tissue and venous structures. Diffusion weighted imaging (DWI;TR/TE=4400/91ms;FA=90°;resolution=1.2×1.2×6.0mm3) acquired within 48 hours from CTP acquisition was used to calculate apparent diffusion coefficients (ADCs) to confirm infarct. Tissue with ADC≤620μm2/s was classified as infarct.10 RAPID, an automatic software to identify ischemic and infarcted tissue, was used to compare with temperature-based stratification.11Imaging data were resampled and transformed to T1-weighted image space using FMRIB’s Linear Image Registration Tool (FLIRT, FSL v6.0.3).12,13 A tensor total-variation regularization algorithm (MATLAB) was used to quantify CBF from CTP data.14 Arterial and venous vessel segments were extracted from skull-stripped15 CTA and T1 images, respectively, after preprocessing. Geometric information of arterial and venous nodes were acquired using NeuTube.16 Imaging data were used to predict patient-specific brain temperatures using a biophysical brain model, adapted from previous reports,9,17 to include full momentum conservation across all domains (arteries+tissue+veins) (Figure 1). Tissue voxels with CBF<10mL were set to 26% of cerebral metabolic rate of oxygen in contralateral voxels as previously reported.18-20
From RAPID, infarcted and salvageable regions include voxels with ipsilateral CBF <30% of contralateral CBF and time-to-maximum >6s but not infarcted, respectively, as used in clinical practice. For temperature-based identification, average ipsilateral (37.16°C) and contralateral (37.25°C) temperatures were used to discriminate ischemic and infarcted regions.2 Specifically, infarct was defined as ipsilateral voxels (voxi) with temperature 37.16<Tinfarct(voxi)<37.25°C, and salvageable regions as Tsalvageable(voxi)>37.25°C, respectively. For both RAPID- and temperature-based analyses, the mismatch ratio was defined as the ratio of combined infarct + salvageable volumes over infarct volume.
Results and Discussion
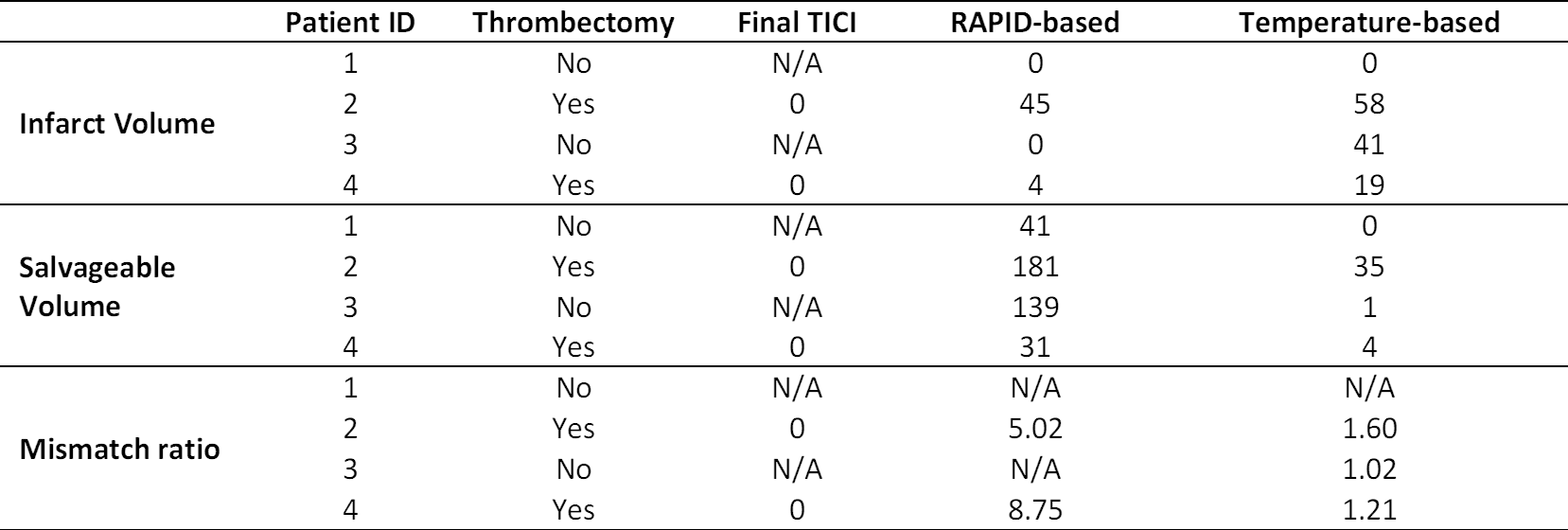
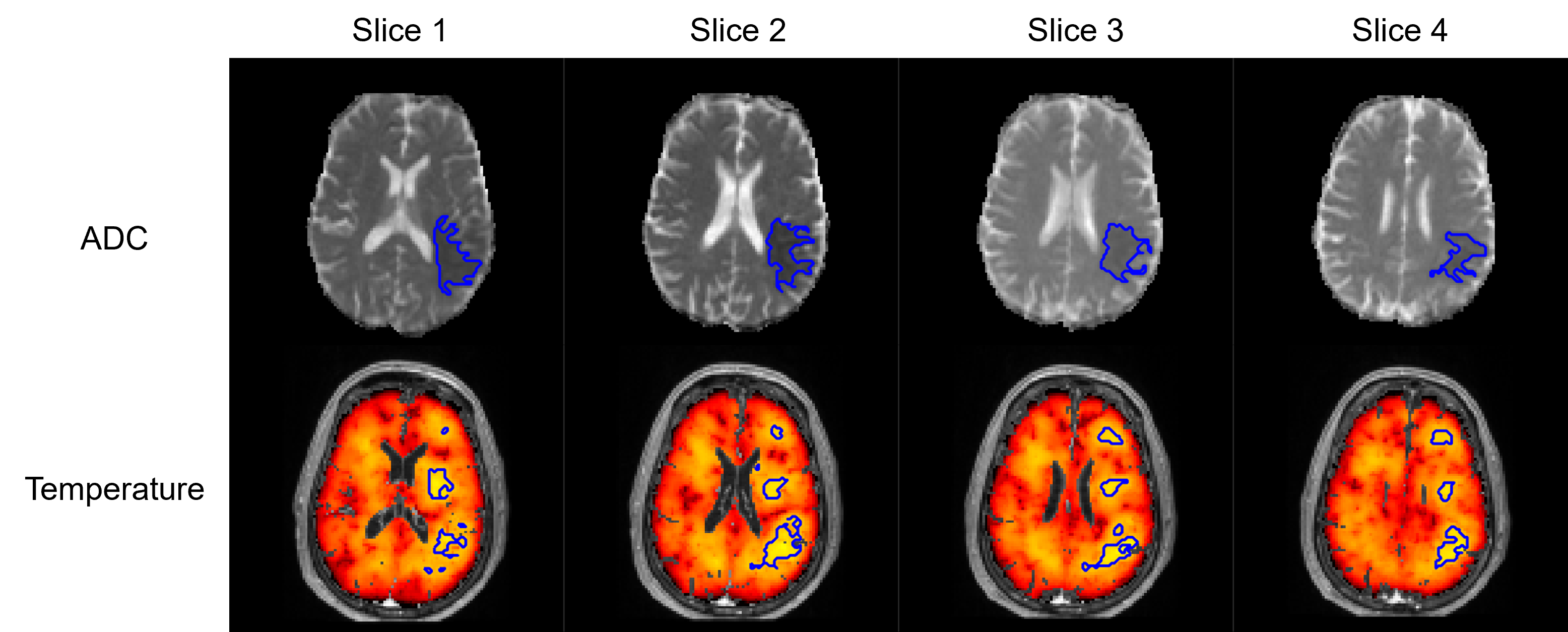
Infarct volumes, salvageable volumes, and mismatch ratios acquired from both RAPID and temperature analysis are summarized in Table 1. Patients 1 and 3 did not undergo thrombectomy as no infarct was identified with RAPID. Temperature analysis also confirmed the absence of an infarct in patient 1, consistent with RAPID. Patient 3 had a non-zero infarct volume from temperature analysis which was inconsistent with RAPID, suggesting potential evolution of infarct. Infarct identified in DWI-ADC images were consistent with infarct regions identified from brain temperature maps (Figure 2). In contrast, both patients 2 and 4 underwent thrombectomy based on RAPID stratification but failed in reperfusion (TICI=0). While temperature-based infarct volumes for both patients were <70mL (satisfying DEFUSE3 inclusion criteria5), the mismatch ratio was <1.8, and these patients would have been excluded based on DEFUSE3 criteria.5 The SELECT2 trial confirmed patients with large infarct volume (>50mL) also benefit from thrombectomy;6 however, the potential risk of complications in patients with small infarct (<50mL from RAPID) as well as small mismatch ratios is unclear. Our results suggest temperature may be an additional marker for patient selection for thrombectomy via improved identification of salvageable tissue and mismatch ratios.Conclusion
We demonstrate the use of brain temperature for patient stratification after AIS. Our brain thermal model includes both perfusion metrics and vascular structure, which may better discriminate infarct from salvageable tissue due to factors such as lack of collateral flow. Model-predicted brain temperatures may be a complementary metric for thrombectomy selection after initial stratification using RAPID.Acknowledgements
This research was supported, in part, by an American Heart Association predoctoral fellowship to D.S. (Award ID: 909342).References
1. Karaszewski B, Wardlaw JM, Marshall I, et al. Measurement of brain temperature with magnetic resonance spectroscopy in acute ischemic stroke. Ann Neurol. 2006;60(4):438-446.
2. Karaszewski B, Wardlaw JM, Marshall I, et al. Early brain temperature elevation and anaerobic metabolism in human acute ischaemic stroke. Brain. 2009;132(4):955-964.
3. Dehkharghani S, Fleischer CC, Qiu D, Yepes M, Tong F. Cerebral temperature dysregulation: MR thermographic monitoring in a nonhuman primate study of acute ischemic stroke. Am J Neuroradiol. 2017;38(4):712-720.
4. Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378(1):11-21.
5. Albers GW, Marks MP, Kemp S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018;378(8):708-718.
6. Sarraj A, Hassan AE, Abraham MG, et al. Trial of endovascular thrombectomy for large ischemic strokes. N Engl J Med. 2023;388(14):1259-1271.
7. Nawabi J, Kniep H, Schön G, et al. Hemorrhage after endovascular recanalization in acute stroke: lesion extent, collaterals and degree of ischemic water uptake mediate tissue vulnerability. Front Neurol. 2019;10:569.
8. Meyer L, Bechstein M, Bester M, et al. Thrombectomy in extensive stroke may not be beneficial and is associated with increased risk for hemorrhage. Stroke. 2021;52(10):3109-3117.
9. Sung D, Risk BB, Kottke PA, et al. Comparisons of healthy human brain temperature predicted from biophysical modeling and measured with whole brain MR thermometry. Sci Rep. 2022;12(1):1-11.
10. Purushotham A, Campbell BC, Straka M, et al. Apparent diffusion coefficient threshold for delineation of ischemic core. Int J Stroke. 2015;10(3):348-353.
11. Laughlin B, Chan A, Tai WA, Moftakhar P. RAPID automated CT perfusion in clinical practice. Pract Neurol. 2019;2019:41-55.
12. Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17(2):825-841.
13. Jenkinson M, Smith S. A global optimisation method for robust affine registration of brain images. Med Image Anal. 2001;5(2):143-156.
14. Fang R, Zhang S, Chen T, Sanelli PC. Robust low-dose CT perfusion deconvolution via tensor total-variation regularization. IEEE Trans Med Imaging. 2015;34(7):1533-1548.
15. Cox RW. AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res. 1996;29(3):162-173.
16. Feng L, Zhao T, Kim J. neuTube 1.0: a new design for efficient neuron reconstruction software based on the SWC format. Eneuro. 2015;2(1):1-10.
17. Sung D, Kottke PA, Risk BB, et al. Personalized predictions and non-invasive imaging of human brain temperature. Commun Phys. 2021;4(1):1-10.
18. Wu L, Wu W, Tali ET, Yuh WT. Oligemia, Penumbra, Infarction: Understanding Hypoperfusion with Neuroimaging. Neuroimaging Clin N Am. 2018;28(4):599-609.
19. Gersing AS, Ankenbrank M, Schwaiger BJ, et al. Mapping of cerebral metabolic rate of oxygen using dynamic susceptibility contrast and blood oxygen level dependent MR imaging in acute ischemic stroke. Neuroradiology. 2015;57(12):1253-1261.
20. An H, Ford AL, Chen Y, et al. Defining the ischemic penumbra using magnetic resonance oxygen metabolic index. Stroke. 2015;46(4):982-988.
Figures