0065
Combining Hyperpolarized 129Xe MR Imaging and Spectroscopy to Estimate Pulmonary Vascular Resistance1Medical Physics, Duke University, Durham, NC, United States, 2Radiology, Duke University, Durham, NC, United States, 3Biomedical Engineering, Duke University, Durham, NC, United States, 4Cardiology, Duke University, Durham, NC, United States
Synopsis
Keywords: Lung, Lung, Pulmonary Hypertension
Motivation: Pulmonary hypertension (PH) and reduced capillary blood volume, VC’, have competing effects on oscillations of the hyperpolarized 129Xe red blood cell (RBC) resonance, rendering it difficult to distinguish PH.
Goal(s): Our goal was to correct RBC oscillations for reduced VC', then use corrected oscillations to estimate pulmonary vascular resistance (PVR).
Approach: We developed a model of RBC oscillations as a function of VC’ in a cohort without known PH and used this model to derive a correction factor. Corrected oscillations were regressed against known PVR in a cohort with suspected PH.
Results: Corrected oscillations improved PH sensitivity and were significantly correlated to PVR.
Impact: Correcting oscillations in the hyperpolarized 129Xe red blood cell resonance for reduced pulmonary capillary blood volume improves sensitivity to pulmonary hypertension and permits estimation of pulmonary vascular resistance, thereby offering a non-invasive diagnostic alternative to right heart catheterization.
Introduction
Inhaled hyperpolarized 129Xe exhibits distinct resonances in the lung airspaces, membrane tissues, and red blood cells (RBCs), enabling MR imaging and spectroscopy of each gas exchange compartment. 129Xe MR spectra, acquired every 15ms, also reveal cardiogenic oscillations in the RBC resonance[1], which tend to decrease in amplitude in the presence of pre-capillary pulmonary hypertension (PH)[2]. Thus, oscillations may provide a non-invasive alternative to right heart catheterization (RHC), the current gold standard method of measuring pulmonary vascular resistance (PVR) and diagnosing PH. However, many patients also exhibit RBC transfer defects on 129Xe imaging (interpreted as reduced pulmonary capillary blood volume), which tend to increase oscillation amplitudes, thereby rendering it difficult to distinguish PH from healthy oscillations[3]. Here, we hypothesize that 129Xe RBC signal oscillations are driven by changes in pulmonary capillary blood volume between systole and diastole, and we implement a windkessel model of pulmonary hemodynamics[4] to estimate the effects of pulmonary capillary and venous impedances on compliance-induced blood storage (Figure 1). We show that as capillary blood volume decreases, capillary impedance increases, thereby increasing the pressure on the microvasculature and the relative oscillation amplitudes. Using this framework, we develop a physiological model to simultaneously account for the competing effects of RBC transfer defects and PH on oscillations, thus enabling combined 129Xe MRI/MRS to non-invasively estimate PVR.Methods
A cohort of subjects without known PH (n=129) underwent the Xenon consortium-standard 129Xe MRI/MRS protocol[5], as did subjects with suspected PH (n=39), who also had RHC within 3 months of imaging. In both cohorts, 129Xe RBC transfer images were used to estimate the capillary blood volume[6]. This was then divided by the expected value, calculated using established regression equations based on age, sex, and height[7], to obtain relative capillary blood volume, VC'. From our physiological hypotheses and the windkessel circuit analogy (Figure 1), and assuming that instantaneous blood-flow differs between systole and diastole (ΔQ is non-zero), we obtain a model of oscillations as a function of VC' given by: $$Osc.=\frac{C}{2V_C}ΔQ(\frac{Z_{C0}}{V_C'}+2Z_V)$$ where C is pulmonary capillary compliance, VC is mean healthy capillary blood volume, ZV is venous impedance, and ZC0 is capillary impedance without capillary blood volume loss. Oscillations were then plotted against VC’ in the non-PH cohort, and the data was fit to a functional form of the model, taking all physiological parameters but VC’ to be unknown. Taking the ratio of fit parameters, we estimated the relative contributions of pulmonary capillary impedance and venous impedance to overall PVR. Additionally, the fit function enables estimation of oscillation amplitude when VC’ is unity. Dividing that estimate by the function itself yielded a correction factor which mitigates oscillation dependence on VC’. This factor was used to generate corrected oscillations in the RHC cohort, which were regressed against the subjects’ known PVR to obtain an equation for PVR estimation.Results
In non-PH subjects, oscillations increased sharply as VC’ decreased according to: $$Osc.=\frac{3.73\%}{V_C'}+6.76\%,$$ showing strong agreement with the functional form of the oscillation model (radj2=0.53) (Figure 2). These parameter estimates indicate that pulmonary capillary impedance is ~10% greater than pulmonary venous impedance. The resulting oscillation correction factor for reduced VC’ is given by: $$Corr.=\frac{2.81V_C'}{1.81V_C'+1}.$$ Applying this factor in the RHC cohort yielded corrected oscillations consistent with healthy reference values for subjects with low PVR (Figure 3), while enhancing sensitivity to PH for subjects with high PVR (Figure 4). Specifically, for every 1WU increase in PVR, an absolute reduction of 0.54% was observed in corrected oscillations (p=0.002) (Figure 3), yielding a PVR estimate of: $$PVR=\frac{1 WU}{0.54%}(10.28\%-Osc_{Corr}\%).$$Discussion
129Xe RBC oscillations increase when capillary blood volume is reduced, consistent with the hypothesized model of blood-flow, pulmonary capillary compliance and impedance. This permits estimation of the contribution of pulmonary capillary impedance and venous impedance to overall PVR. Notably, this also permits oscillations to be corrected for reduced capillary blood volume, thereby yielding a non-invasive means of estimating PVR. Given that this PVR estimate depends on two of the weaker signals in 129Xe MRI/MRS (RBC transfer images and RBC oscillations), it is imperative to optimize the SNR of both acquisitions. Furthermore, given the hypothesized physiological model, future work will distinguish changes in the ratio of pulmonary capillary compliance to mean healthy capillary blood volume from changes in systolic and diastolic blood-flow, as a function of PVR, in order to determine which physiological parameters are driving the negative linear correlation between corrected oscillations and PVR. Nonetheless, these results suggest the potential for improved utility of 129Xe MRI/MRS in assessing PH, thus limiting the need for RHC.Acknowledgements
R01HL105643, R01HL153872References
1. Bier EA, Robertson SH, Schrank G, Rackley C, Mammarappallil J, Rajagopal S, McAdams HP, Driehuys B. A protocol for quantifying cardiogenic oscillations in dynamic 129Xe gas exchange spectroscopy: the effects of idiopathic pulmonary fibrosis. NMR in Biomedicine 2019;32(1)
2. Wang Z, Bier EA, Swaminathan A, Parikh K, Nouls J, He M, Mammarappallil JG, Luo S, Driehuys B, Rajagopal S. Diverse cardiopulmonary diseases are associated with distinct xenon magnetic resonance imaging signatures. European Respiratory Journal 2019;54(6)
3. Costelle A, Lu J, Bechtel A, Bier EA, Kabir S, Mammarrappallil J, Dai H, Mummy D, Driehuys B. Quantifying cardiogenic oscillations of hyperpolarized 129Xe gas exchange MR spectra in a healthy reference cohort. In: Proceedings from ISMRM; June 3-June 8, 2023; Toronto, ON. Abstract 0857.
4. Gerringer JW, Wagner JC, Vélez-Rendón D, Valdez-Jasso D. Lumped-parameter models of the pulmonary vasculature during the progression of pulmonary arterial hypertension. Physiol Rep. 2018 Feb;6(3):e13586.
5. Niedbalski, P. J. et al. Protocols for multi-site trials using hyperpolarized 129Xe MRI for imaging of ventilation, alveolar-airspace size, and gas exchange: A position paper from the 129Xe MRI clinical trials consortium. Magn Reson Med 86, 2966–2986 (2021).
6. Wang Z, Rankine L, Bier EA, Mummy D, Lu J, Church A, Tighe RM, Swaminathan A, Huang YT, Que LG, Mammarappallil JG, Rajagopal S, Driehuys B. Using hyperpolarized 129Xe gas-exchange MRI to model the regional airspace, membrane, and capillary contributions to diffusing capacity. J Appl Physiol (1985). 2021 May 1;130(5):1398-1409.
7. Munkholm M, Marott JL, Bjerre-Kristensen L, Madsen F, Pedersen OF, Lange P, Nordestgaard BG, Mortensen J. Reference equations for pulmonary diffusing capacity of carbon monoxide and nitric oxide in adult Caucasians. Eur Respir J. 2018 Jul 19;52(1):1500677.
Figures
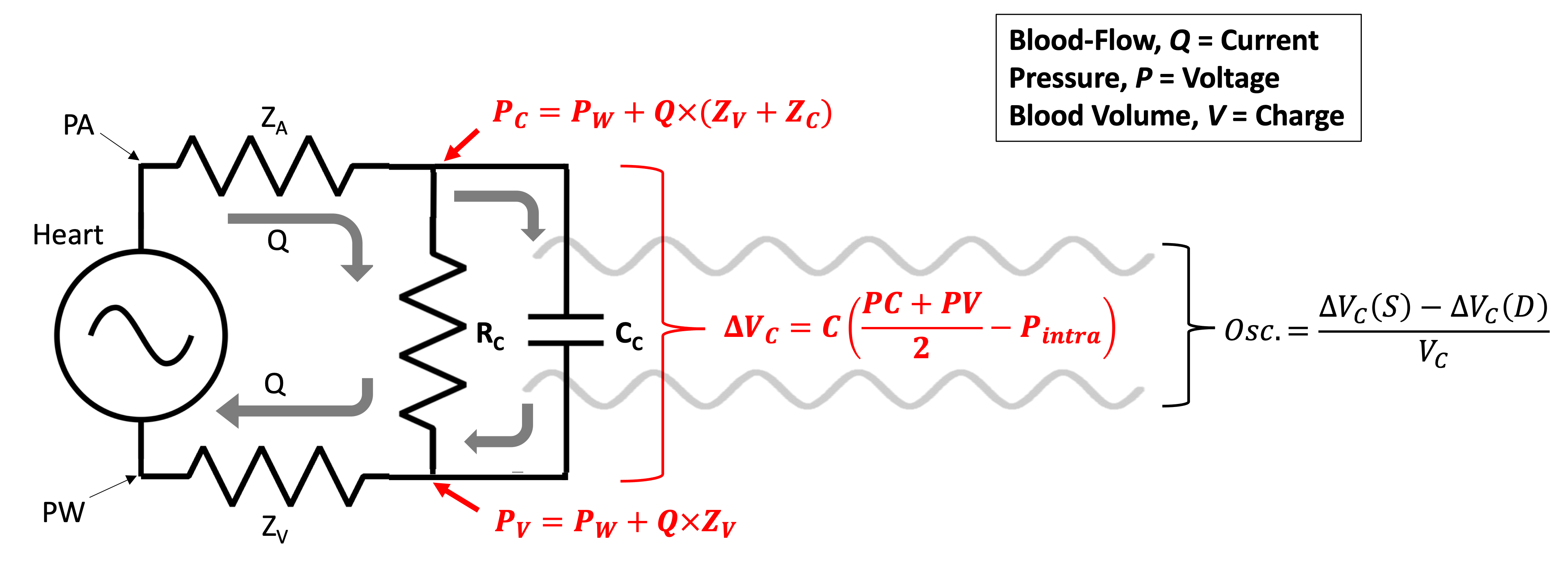
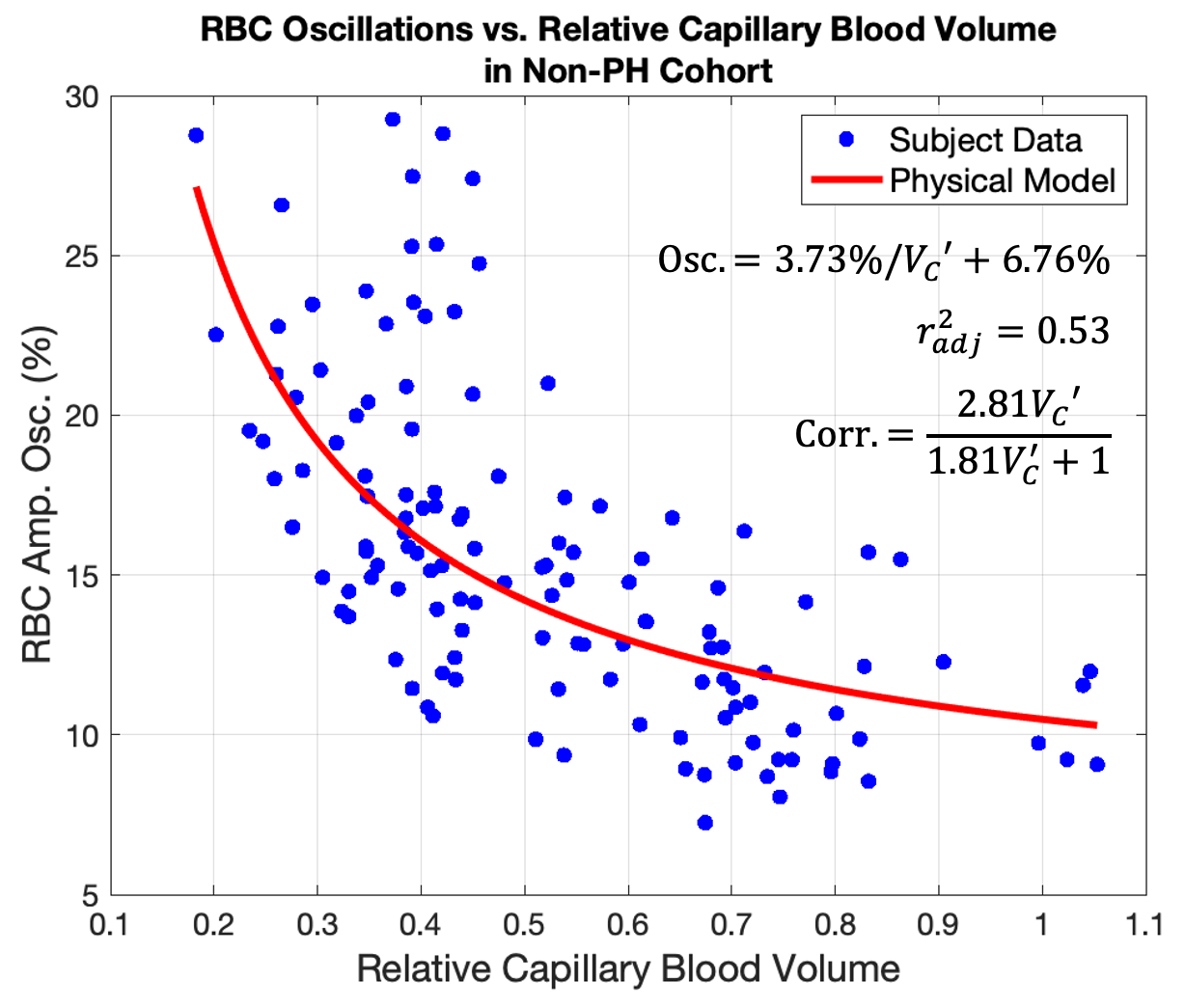
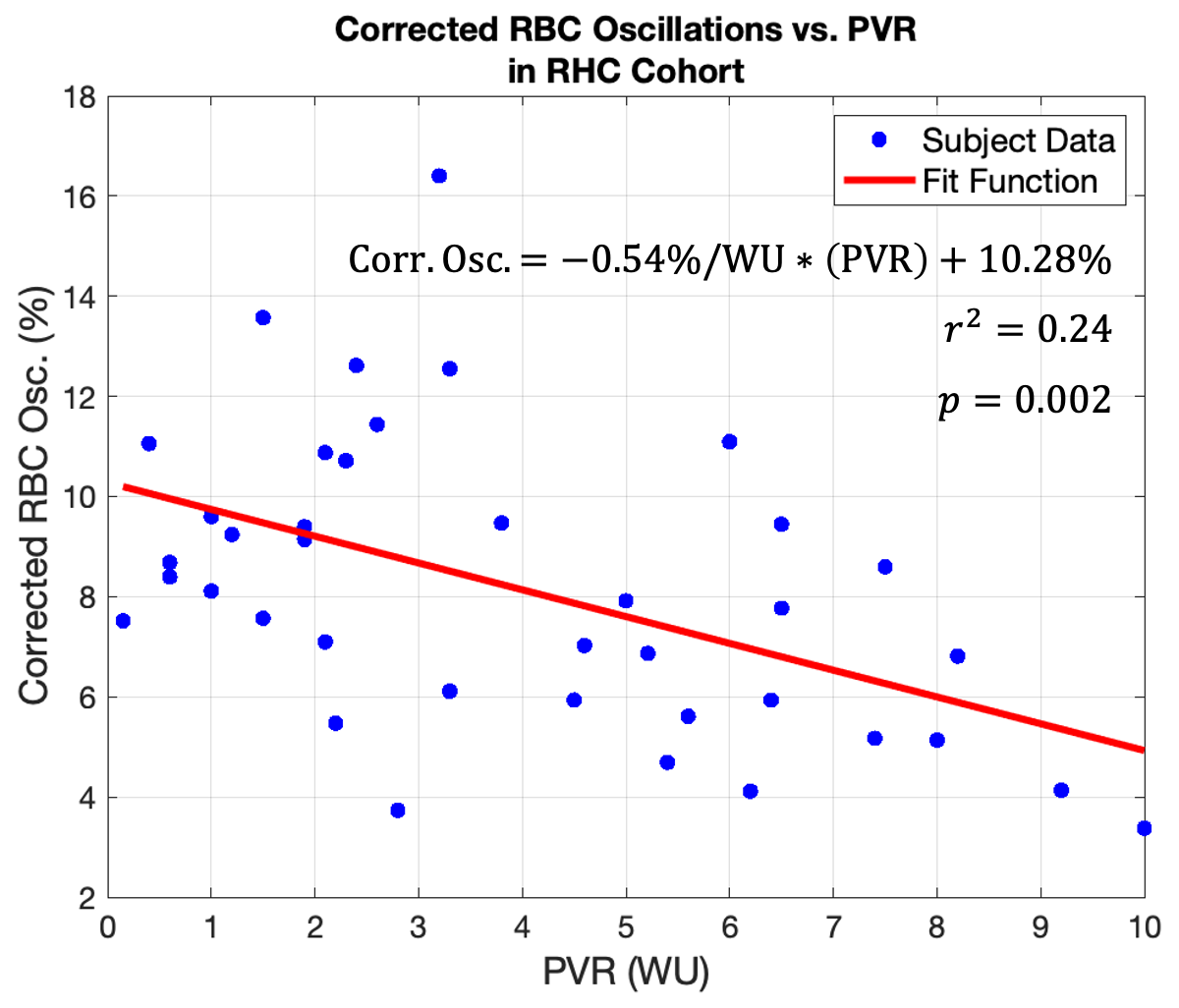
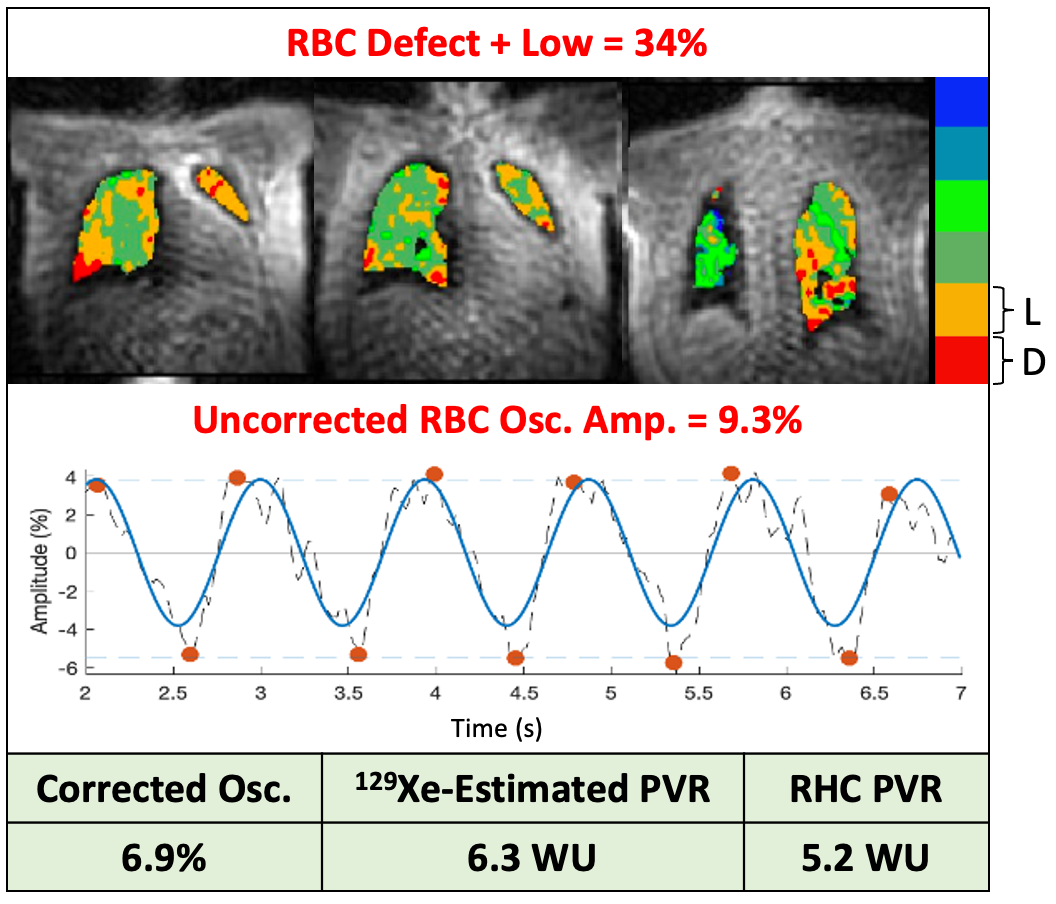
Figure 4. Representative RBC transfer images and oscillations in a subject with pre-capillary PH. For this subject, who has significant regions of low and defective RBC transfer, uncorrected oscillations fall within the healthy reference range. Once corrected for RBC transfer, oscillations decrease and are now indicative of high PVR.