0064
Preliminary Investigation of Feasibility, Tolerability, and Image Quality of Perfluoropropane Ventilation MRI in Pediatric Participants1Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 2Medical Biophysics, University of Toronto, Toronto, ON, Canada, 3Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, United Kingdom, 4Newcastle Magnetic Resonance Centre, Newcastle University, Newcastle upon Tyne, United Kingdom, 5Division of Respiratory Medicine, The Hospital for Sick Children, Toronto, ON, Canada
Synopsis
Keywords: Lung, Lung, 19F, Fluorine-19, Ventilation, Perfluoropropane, Gas
Motivation: Inert fluorinated gas MRI has potential as a lower cost alternative to hyperpolarized noble gas MRI for lung ventilation imaging. However, this technology has not yet been evaluated for use in pediatrics.
Goal(s): To investigate the feasibility, tolerability, and image quality of inert fluorinated gas MRI with perfluoropropane (PFP) in pediatric participants.
Approach: PFP MRI was performed in pediatric participants. Image quality, SNR, and ventilation defect percent (VDP) were evaluated.
Results: PFP MRI was well-tolerated and successfully performed in all pediatric recruits. Image quality was good and permitted quantification of ventilation defect percent (VDP).
Impact: PFP MRI was determined to be feasible in pediatrics, yielding ventilation images and image quality similar to hyperpolarized gas MRI. This may permit more widespread adoption for the study of pediatric lung disease in the future.
Introduction
Lung MRI may offer important insight into pediatric pulmonary function to complement current clinical methods1. Inert fluorinated (19F) gas MRI is an emergent technology with potential to be a lower cost, reduced infrastructure alternative to hyperpolarized (HP) gas MRI for functional lung imaging2, providing similar and/or complementary information3,4, including response to treatment5,6. Fluorinated gases, such as perfluoropropane (PFP;C3F8), are biologically inert, can be used in normoxic mixtures and, most importantly, do not require hyperpolarization. Instead, these gases rely on a relatively high number of 19F nuclei per molecule as well as signal averaging enabled by short T1, permitting imaging at thermal equilibrium2. Despite the advantages of inert fluorinated gas MRI for functional lung imaging, to our knowledge there are few or no demonstrations in the literature of this technology in pediatric subjects. The purpose of this work is to investigate the initial feasibility and tolerability of lung MRI using PFP in pediatric participants in anticipation of future applications to pediatric lung disease (eg. cystic fibrosis).Methods
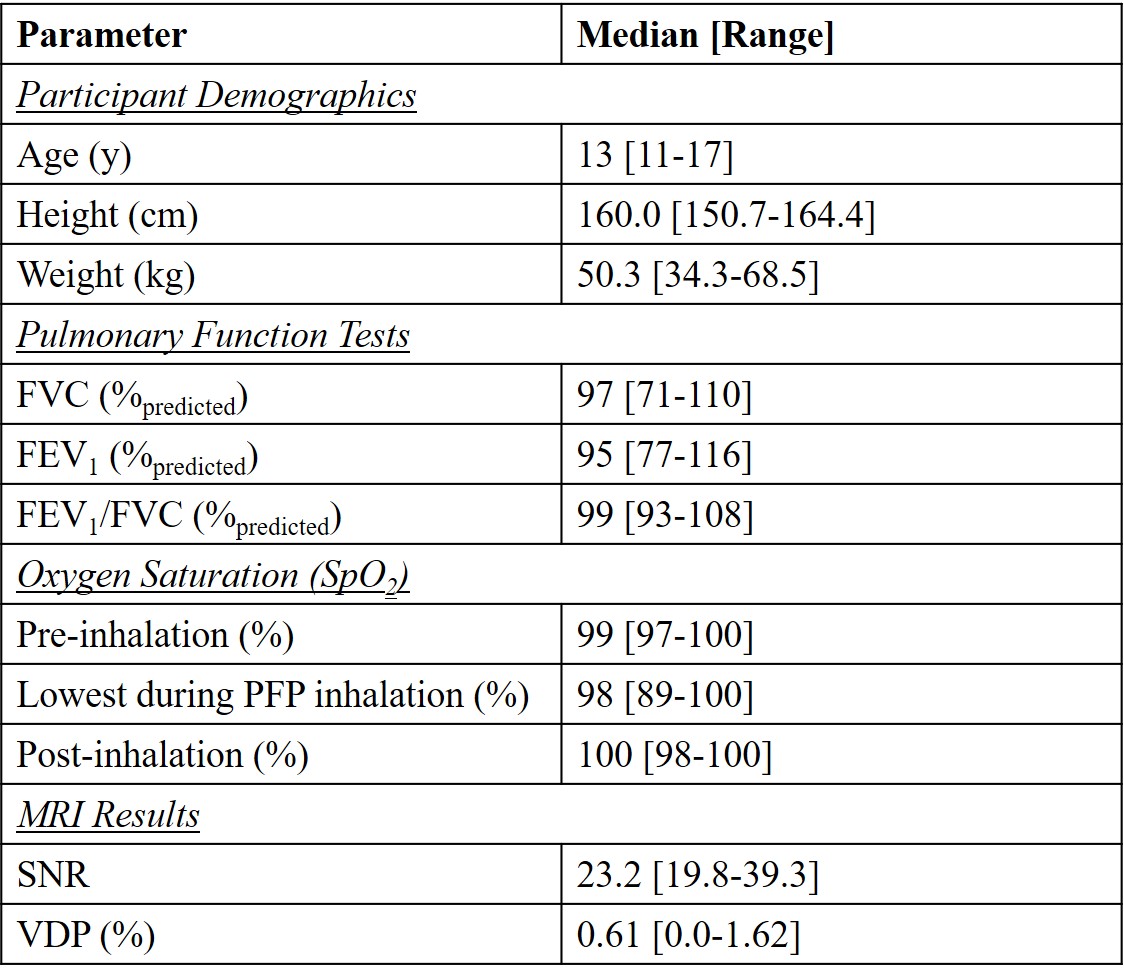
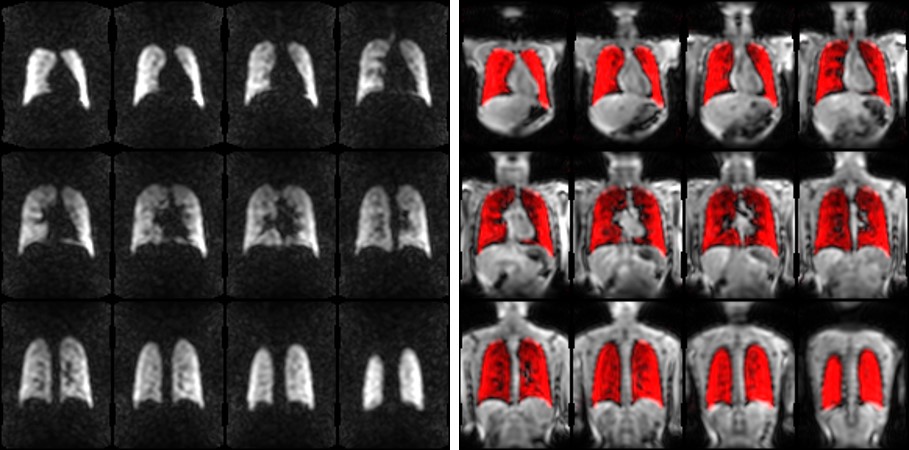
Seven pediatric participants (4 male, 3 female, 11-17 years) with no history of lung disease were recruited using an institutional and Health Canada approved protocol, performing spirometry and MRI in the same visit. Imaging was performed on a clinical 3T system (Siemens Prismafit, Erlangen, Germany) with a 19F rigid elliptical birdcage transmitter and 8-channel receive array (Rapid Biomedical, Rimpar, Germany). Participants were instructed to take 5 breaths from a reservoir of gas (21% O2/79% PFP) (AirGas, Radnor, PA) to saturate the lungs, then inhale to total lung capacity (TLC) and hold their breath for the duration of the MRI acquisition. For ventilation imaging, a 3D-GRE acquisition was used guided by previous literature7 with the following parameters: FOV=360×480×(180-240) mm3, acquisition matrix=36×48×(18-24), TE=1.67 ms, TR=8.7 ms, flip angle=45⁰, BW=500Hz/pixel, Navg=4, GRAPPA factor=2 (12 reference lines), breath-hold duration=12-16 sec. The acquired resolution was 10 mm isotropic interpolated to 5 mm isotropic. SpO2 was monitored and recorded prior to PFP inhalation, during the PFP administration and imaging procedure, and at 2 minutes post-inhalation (Expression 4400, InVivo). Lastly, a resolution-matched 1H thoracic cavity scan was acquired during a coached breath-hold at TLC. Images were analyzed offline in MATLAB 2022a (MathWorks, Natick, MA). SNR was measured on a central slice (trachea or first bifurcation visible) with a 4x4 cm2 ROI to measure signal in the middle of the right lung, and a 100 cm2 ROI placed below the lungs to measure noise. 1H images were segmented to extract a thoracic cavity mask. PFP ventilation images were registered to and masked by the thoracic cavity using a non-rigid demons registration. Voxels with signal intensity less than 2 standard deviations from the mean were classified as defects, and the total defect volume relative to the thoracic cavity volume was used to compute the ventilation defect percent (VDP).Results
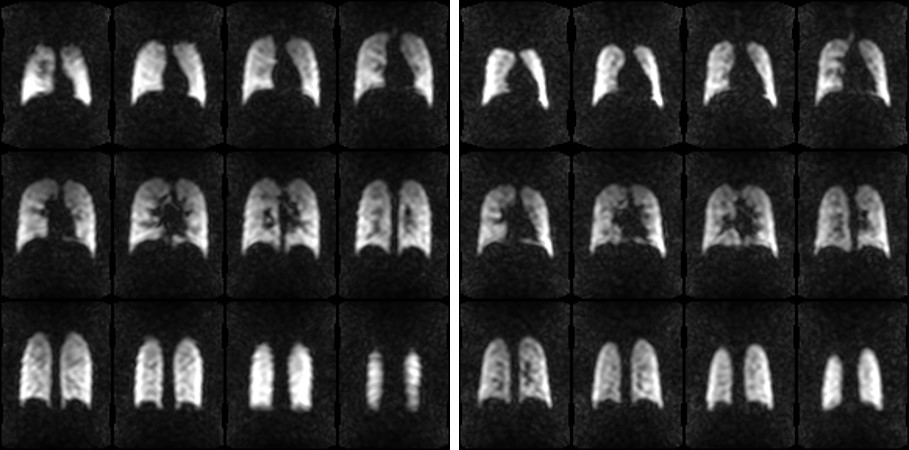
Participant demographics, pulmonary function, and oxygen saturation measurements are shown in Table 1. All MRI procedures were well-tolerated, and completed by all participants. SpO2 measured during the PFP administration and imaging procedure were well-tolerated with only minor, transient desaturations in a few cases. Figure 1-3 shows representative PFP ventilation images, and registration to 1H thoracic cavity scans. The median [range] of SNR across all subjects was 23.2 [19.8-39.3], while VDP was determined to be 0.61 [0.0-1.62] %.Discussion
Inert fluorinated gas MRI was determined to be feasible in pediatric participants. Ventilation images exhibited homogeneous signal distribution with no obvious defects, consistent with health in this population. The SNR measured across this cohort of pediatrics was reasonably consistent with previous studies in adults7, enabling quantification of ventilation defect. VDP was nearly zero, as expected in these healthy volunteers. Limitations of the current work are the small numbers, and the focus on healthy volunteers only at this time. However, the results of this work indicate that inert fluorinated gas MRI is promising for future deployment in pediatric patient populations. Work is ongoing to explore this technology in pediatric lung disease (eg. cystic fibrosis) alongside hyperpolarized 129Xe for comprehensive evaluation and validation. As with hyperpolarized gases, fluorinated gases are also useful for probing terminal airway microstructure by way of diffusion-weighted imaging, which we also plan to explore in pediatrics8. Additionally, since fluorinated gases may be freely mixed with oxygen, extended, free-breathing experiments that permit more comprehensive investigation of gas washin and washout kinetics in the lungs are possible to complement static imaging9–11.Conclusion
In this preliminary work, inert fluorinated gas MRI was demonstrated to be safe, tolerable, and feasible in children as young as 11 y.o.Acknowledgements
The authors thank Sharon Braganza, Daniel Li, Tammy Rayner, and Ruth Weiss for assistance with imaging experiments. Special thanks to Dr. Tobias Wichmann for technical assistance with calibration and deployment of the 19F hardware used in this work. This work was supported by CIHR, NSERC Alliance, and Siemens Healthineers.References
1. Zanette B, Greer M-LC, Moraes TJ, Ratjen F, Santyr G. The argument for utilising magnetic resonance imaging as a tool for monitoring lung structure and function in pediatric patients. Expert Rev Respir Med. 2023;17(7):527-538. doi:10.1080/17476348.2023.2241355
2. Couch MJ, Ball IK, Li T, Fox MS, Biman B, Albert MS. 19 F MRI of the Lungs Using Inert Fluorinated Gases: Challenges and New Developments. J Magn Reson Imaging. 2019;49(2):343-354. doi:10.1002/jmri.26292
3. Obert AJ, Gutberlet M, Kern AL, et al. 1H-guided reconstruction of 19F gas MRI in COPD patients. Magn Reson Med. 2020;84(3):1336-1346. doi:10.1002/mrm.28209
4. McCallister A, Chung SH, Antonacci M, et al. Comparison of single breath hyperpolarized 129 Xe MRI with dynamic 19 F MRI in cystic fibrosis lung disease. Magn Reson Med. 2021;85(2):1028-1038. doi:10.1002/mrm.28457
5. Goralski JL, Chung SH, Ceppe AS, et al. Dynamic Perfluorinated Gas MRI Shows Improved Lung Ventilation in People with Cystic Fibrosis after Elexacaftor/Tezacaftor/Ivacaftor: An Observational Study. J Clin Med. 2022;11(20). doi:10.3390/jcm11206160
6. Neal MA, Holland C, Pippard BJ, et al. 19F-MRI of pulmonary ventilation: Assessment of response to treatment in asthma and COPD. Proc Intl Soc Mag Reson Med. 2023;31:0714.
7. Pippard BJ, Neal MA, Maunder AM, et al. Reproducibility of 19F-MR ventilation imaging in healthy volunteers. Magn Reson Med. 2021;85(6):3343-3352. doi:10.1002/mrm.28660
8. Maunder A, Chan HF, Hughes PJC, et al. MR properties of 19F C3F8 gas in the lungs of healthy volunteers: T2∗ and apparent diffusion coefficient at 1.5T and T2∗ at 3T. Magn Reson Med. 2021;85(3):1561-1570. doi:10.1002/mrm.28511
9. Gutberlet M, Kaireit TF, Voskrebenzev A, et al. Free-breathing dynamic 19F gas MR imaging for mapping of regional lung ventilation in patients with COPD. Radiology. 2018;286(3):1040-1051. doi:10.1148/radiol.2017170591
10. Goralski JL, SH C, Glass T, et al. Dynamic perfluorinated gas MRI reveals abnormal ventilation despite normal FEV1 in cystic fibrosis. JCI Insight. 2020;5(2):e133400. doi:https://doi.org/10.1172/jci.insight.133400
11. Obert AJ, Kern AL, Gutberlet M, et al. Volume-Controlled 19F MR Ventilation Imaging of Fluorinated Gas. J Magn Reson Imaging. 2023;57(4):1114-1128. doi:10.1002/jmri.28385
Figures