0063
Acceleration of Ventilation-Weighted Free-Breathing Functional 1H MRI in Pediatric Cystic Fibrosis Lung Disease1Pulmonary Medicine, Cincinnati Children's Hospital, Cincinnati, OH, United States, 2Medical Biophysics, University of Toronto, Toronto, ON, Canada, 3Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 4Division of Respiratory Medicine, The Hospital for Sick Children, Toronto, ON, Canada
Synopsis
Keywords: Lung, Lung, hyperpolarized 129-Xenon, functional lung MRI
Motivation: Free-breathing pulmonary MRI acquisitions can be lengthy (i.e. 1-minute per slice) which can prove challenging for imaging pediatric lung diseases.
Goal(s): The purpose of this work is to determine if reducing the free-breathing MRI scan time will produce stable ventilation defect measures that agree with hyperpolarized 129Xenon-MRI (Xe-MRI).
Approach: Free-breathing MRI data acquired in cystic fibrosis patients were retrospectively truncated to compare measured Xe-MRI ventilation defects at shorter acquisition times.
Results: Free-breathing MRI ventilation defects showed minimal variability and similar correlation strength to Xe-MRI following approximately 40% reductions in scan time.
Impact: Free-breathing MRI can evaluate pulmonary ventilation in pediatric cystic fibrosis lung disease in agreement with 129Xenon-MRI but is lengthy. Accelerated free-breathing MRI allows for decreased scan durations, without compromising ventilation maps. This can potentially improve clinical translation, especially in pediatrics.
Introduction
Hyperpolarized 129Xe MRI (Xe-MRI) can evaluate ventilation defects in pediatric CF lung disease1 but requires a 7-9 second breath-hold and additional time to polarize the 129Xe gas. Alternatively, contrast-agent free, free-breathing 1H MRI techniques, such as phase-resolved functional lung (PREFUL)2 and dynamic mode decomposition (DMD)3 MRI, can assess regional pulmonary ventilation during ~1 minute of free-breathing per coronal slice of the lung. Reducing the number of image repetitions required for analysis may improve scan efficiency but it is unclear if the shorter acquisition times may impact the variability of the derived ventilation maps and ventilation defect percentage (VDP) values. Furthermore, PREFUL MRI has been used in CF lung disease4, while DMD MRI has not, and the direct comparison of these free-breathing 1H MRI techniques has not been reported in CF. Therefore, the purpose of this work is to determine the variability of ventilation-weighted PREFUL and DMD MRI during shorter scan durations in comparison to Xe-MRI in pediatric CF patients.Methods
MRI was performed on 8 pediatric CF patients (aged 15±2 years old) over 3-4 visits (total n=21), using a 3T scanner (Magnetom Prismafit, Siemens Healthcare, Erlangen, Germany) following REB-approved protocols. Xe-MRI was performed using an established protocol4. Participants performed spirometry5 and N2 multiple breath washout6 to obtain forced expiratory volume in one second (FEV1 % pred.) and lung clearance index (LCI), respectively. During free-breathing MRI, 4-5 coronal slices of the lung were acquired for 512 repetitions (~60 seconds per slice) using a TurboFLASH sequence as previously described4. Using MATLAB (MathWorks, Natick, MA), group-oriented registration7 to the mid-respiration phase was performed to each set of 512 images and separate fractional ventilation (FV) maps were determined following the PREFUL2 and DMD (https://github.com/EfeIlicak/DMD_Lung)3 algorithms. PREFUL and DMD MRI VDP (VDPPREFUL and VDPDMD, respectively) were determined using linear binning8 where 6 age-matched healthy controls were used to determine corresponding reference histograms. Xe-MRI VDP (VDPXe) was determined using a threshold of 60% of the mean signal9. Additionally, the number of repetitions acquired for each slice was retrospectively truncated to determine FV maps and VDP values corresponding to 60-, 48-, 36-, 24-, and 12-second acquisition times respectively. Differences in VDPPREFUL and VDPDMD at different acquisition times were compared using a Wilcoxon signed-rank test. Correlations between free-breathing VDP metrics determined at different acquisition times and VDPXe, FEV1, and LCI were determined using the Pearson correlation coefficient (r). VDPPREFUL and VDPDMD were compared using Bland-Altman analysis.Results
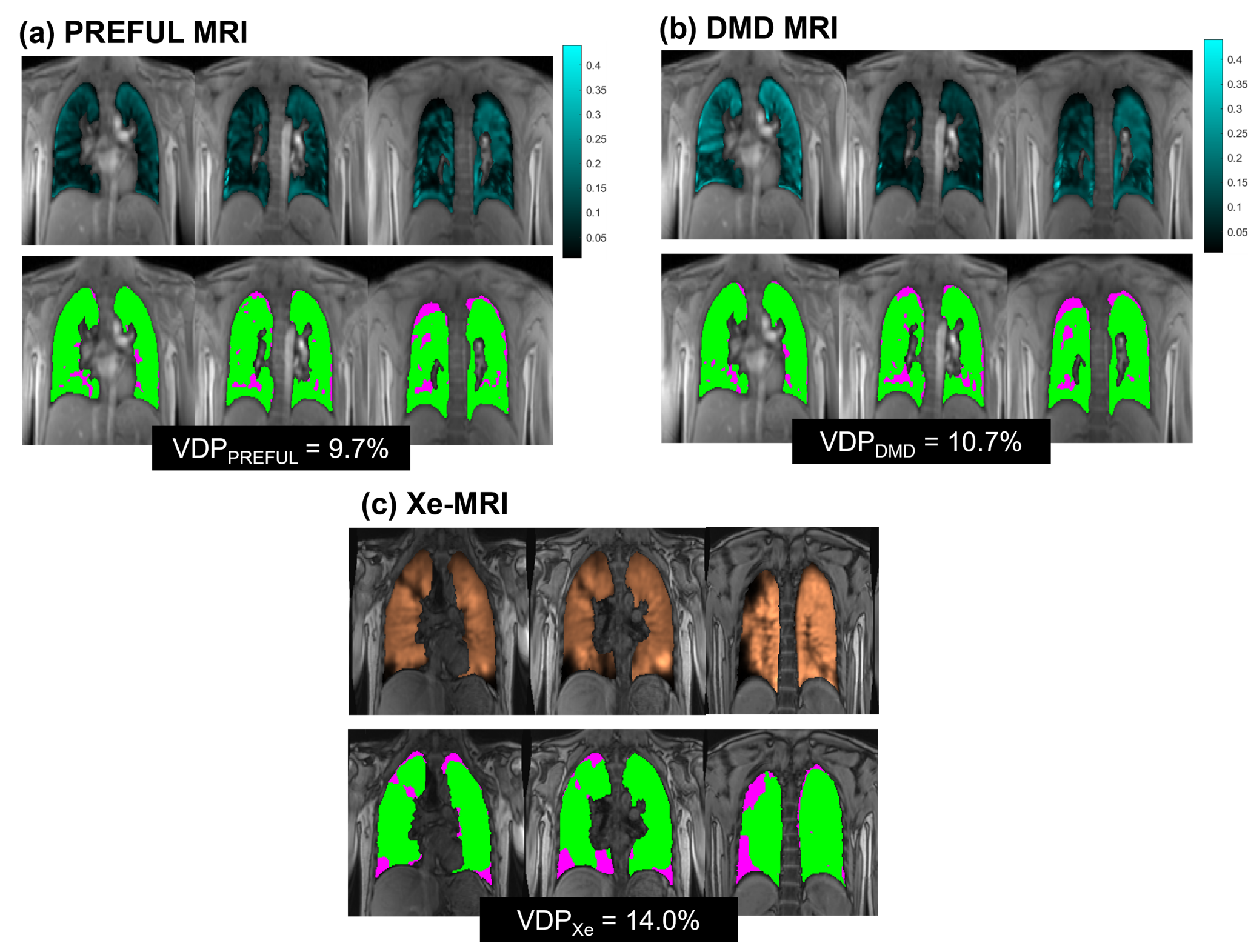
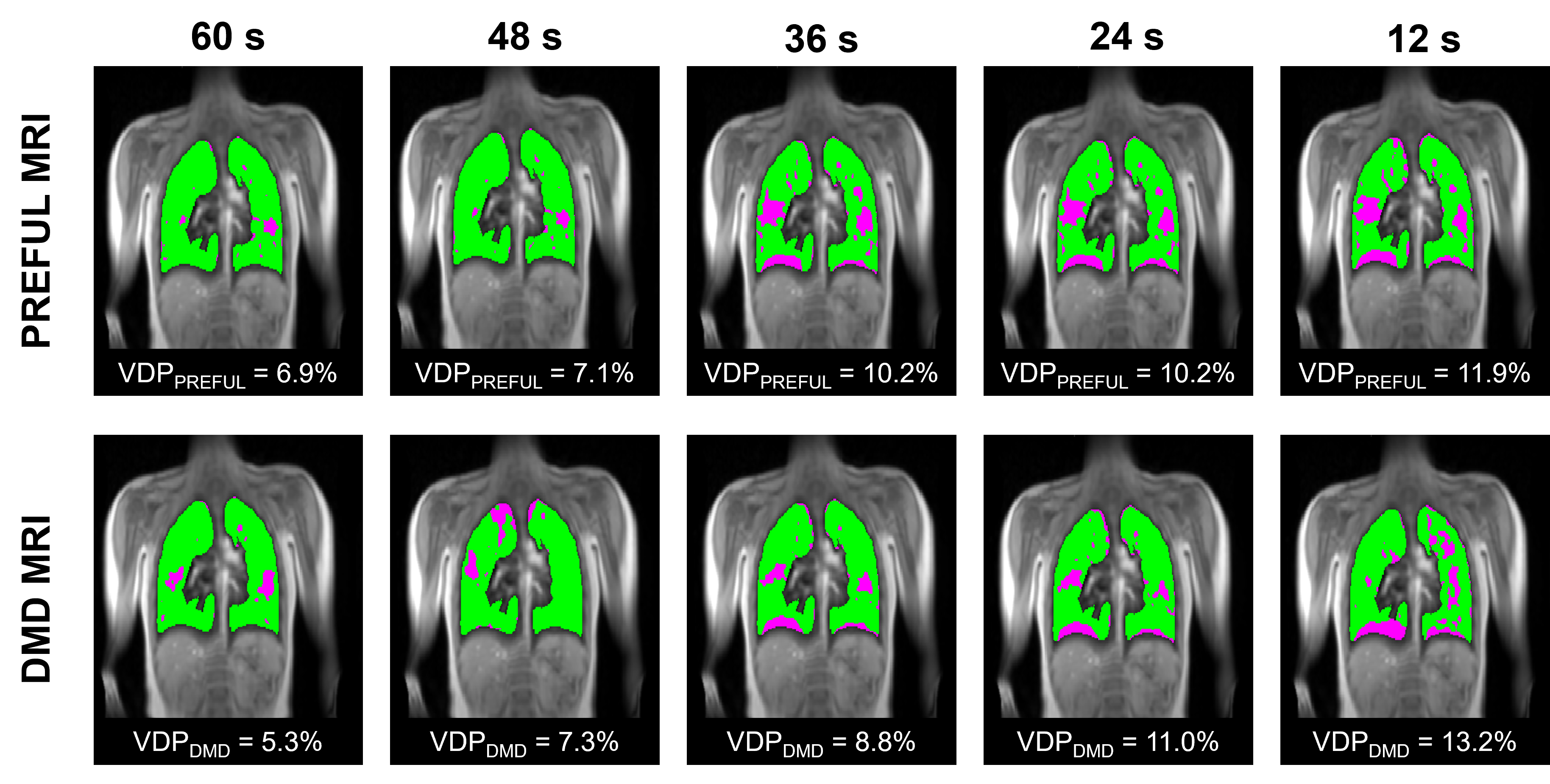
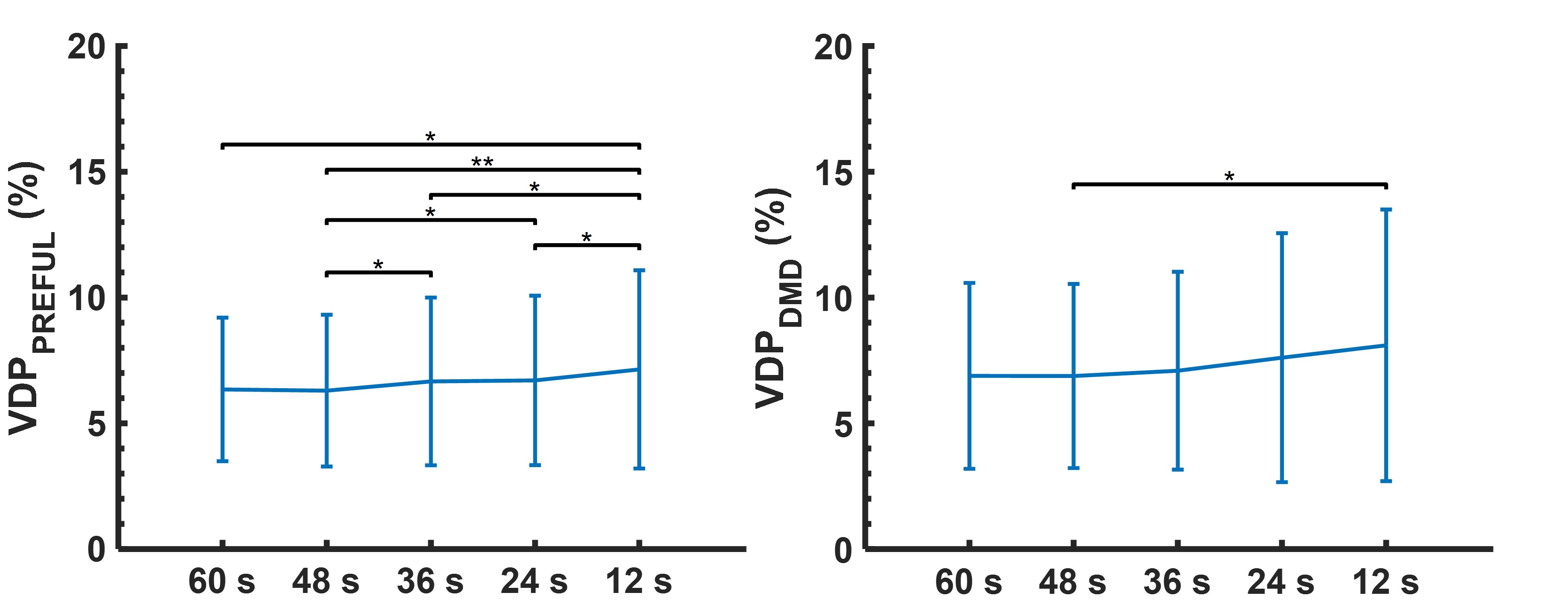
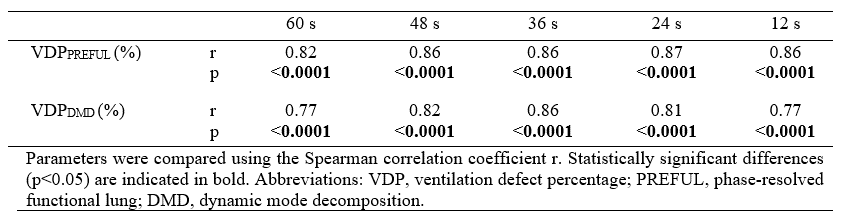
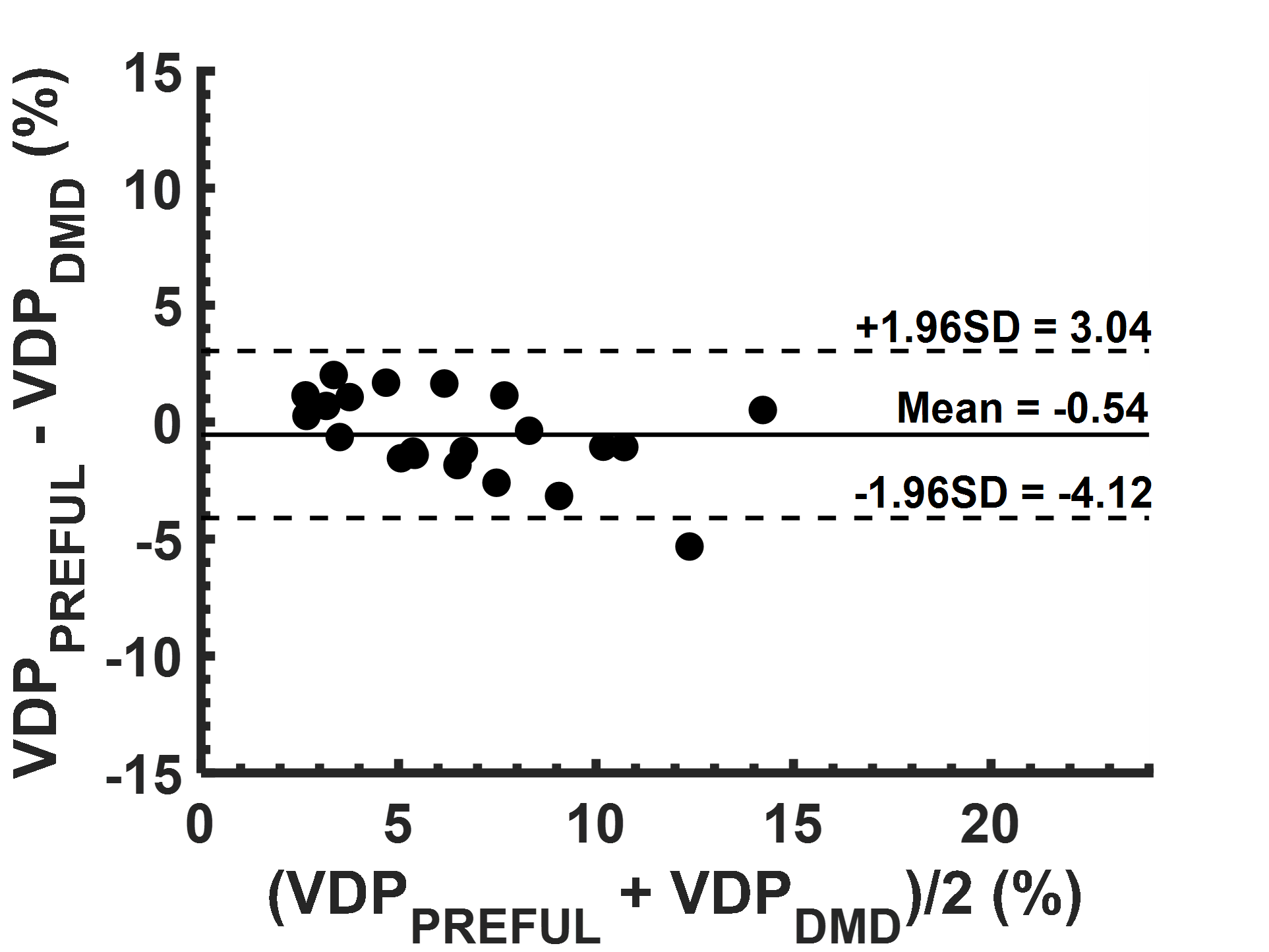
Figure 1 shows the ventilation maps of a representative CF participant that were derived from the free-breathing MRI techniques (using a full 60-second acquisition) and Xe-MRI. Figure 2 shows the VDP values, for a representative CF participant, from the free-breathing MRI methods with five different acquisition durations. Figure 3 illustrates the VDP differences across the entire CF cohort. Both VDPPREFUL and VDPDMD trended higher following scan time reductions below 36 seconds for two patient visits. The correlation of free-breathing MRI VDP values for varying acquisition durations to VDPXe are shown in Table 1. VDPPREFUL and VDPDMD showed a consistently strong correlation to VDPXe across all acquisition durations (all r>0.77; p<0.0001). All VDP metrics significantly correlated with LCI (all r>0.60; p<0.007), but none correlated with FEV1 (all p>0.05). Across all CF patient visits, VDPPREFUL and VDPDMD were not significantly different (p>0.05) and showed a negligible negative bias (Figure 4).Discussion
VDPPREFUL had a statistically significant increase at scan durations shorter than 36 seconds, and VDPDMD showed a significant increase at 12 seconds relative to a 48-second acquisition. However, the trend towards higher VDP values was largely driven by two patients in which VDP changed by 6-8% with decreased acquisition time. Additionally, VDPPREFUL and VDPDMD both strongly correlated with VDPXe across all acquisition durations despite the overall increase. Limitations of this study include a low number of healthy controls used to determine VDP threshold values for linear binning analysis. Furthermore, a majority of the CF patients in this study presented mild disease (i.e. LCI=6-7) and analysis of intra-scan variability would benefit from a wider range of disease severity. Overall, both free-breathing MRI methods showed minimal change across decreasing acquisition windows for 40% (i.e. 36-second acquisition) reductions in scan time and showed a strong correlation to Xe-MRI for up to an 80% (i.e. 12-second acquisition) data reduction. Thus, acceleration of the free-breathing MRI techniques may be feasible for determining reliable ventilation maps and corresponding VDP values.Conclusion
A reduction in acquisition time of ~40% in free-breathing MRI techniques is possible when assessing pulmonary ventilation in CF lung disease and may lead to easier clinical translation.Acknowledgements
We would like to thank the following sources of funding: The Hospital for Sick Children, Natural Sciences and Engineering Research Council of Canada (NSERC) Discovery grant (RGPIN 217015-2013), the Cystic Fibrosis Foundation (CFF), Canadian Institutes of Health and Research (CIHR) operation and project grants (MOP 123431, PJT 153099). Samal Munidasa would like to thank the SickKids Restracomp program and NSERC for their support.References
- Santyr G, Kanhere K, Morgado F, et al. Hyperpolarized Gas Magnetic Resonance Imaging of Pediatric Cystic Fibrosis Lung Disease. Acad Radiol. 2019;26(3):344-354.
- Voskrebenzev A, Gutberlet M, Klimeš F, Kaireit TF, Schönfeld C, Rotärmel A, Wacker F, Vogel-Claussen J. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med. 2018 Apr;79(4):2306-2314
- Ilicak E, Ozdemir S, Zapp J, Schad LR, Zöllner FG. Dynamic mode decomposition of dynamic MRI for assessment of pulmonary ventilation and perfusion. Magn Reson Med. 2023 Aug;90(2):761-769.
- Munidasa S, Zanette B, Couch M, Grimm R, Seethamraju R, Dumas MP, Wee W, Au J, Braganza S, Li D, Woods J, Ratjen F, Santyr G. Inter- and intravisit repeatability of free-breathing MRI in pediatric cystic fibrosis lung disease. Magn Reson Med. 2023 May;89(5):2048-2061.
- Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319-338.
- Robinson PD, Latzin P, Verbanck S, et al. Consensus statement for inert gas washout measurement using multiple- and single breath tests. Eur Respir J. 2013;41:507-522.
- Voskrebenzev A, Gutberlet M, Kaireit TF, Wacker F, Vogel-Claussen J. Low-pass imaging of dynamic acquisitions (LIDA) with a group-oriented registration (GOREG) for proton MR imaging of lung ventilation. Magn Reson Med. 2017 Oct;78(4):1496-1505.
- He M, Driehuys B, Que LG, Huang YT. Using Hyperpolarized 129Xe MRI to Quantify the Pulmonary Ventilation Distribution. Acad Radiol. 2016 Dec;23(12):1521-1531.
- Thomen RP, Walkup LL, Roach DJ, Cleveland ZI, Clancy JP, Woods JC. Hyperpolarized 129Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. J Cyst Fibros. 2017 Mar;16(2):275-282.
Figures