0060
Investigating Gravitational Influence on Normal Lung Function Using PREFUL MRI on an Open Scanner1Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham, United Kingdom, 2Nottingham NIHR Biomedical Research Centre, University of Nottingham, Nottingham, United Kingdom
Synopsis
Keywords: Lung, Lung
Motivation: Insights into the factors contributing to local ventilation and perfusion variation within the lungs are of crucial importance to improving patient care.
Goal(s): To investigate the gravity dependent contributions to regional heterogeneity of normal lung function including ventilation and perfusion.
Approach: With use of an open MRI system, participants were scanned in three positions to vary the direction of gravity experienced by the lungs. PREFUL analysis was employed to attain fractional ventilation, normalised perfusion, and associated Time-To-Peak markers.
Results: Contributions from both gravity and physiological factors were observed in ventilation and perfusion distribution for each of the three positions.
Impact: Enhanced understanding of the causes of functional variations in healthy lungs will allow physicians to make more informed decisions regarding patient care. Additionally, posture dependent lung function could serve as a marker for lung disease and support stratified treatment approaches.
Introduction
Understanding the factors influencing local ventilation and perfusion within the lungs is of great importance for improving patient care. Initially attributed solely to gravity and compression of lung parenchyma, our insight into the determinants of lung function heterogeneity have evolved with improvements in imaging methodologies. Differences in ventilation and perfusion within gravitational planes have contributed to the theory that the geometry of vascular and airway trees also play a role in regional lung function1.Phase Resolved Functional Lung (PREFUL) MRI2 has been demonstrated to visualise dynamic lung function in health and disease. However, conventional MRI systems typically offer limited opportunity to investigate the effect of gravity on the lungs. In contrast, open MRI systems allow for a greater range of scanning positions beyond lying down in an enclosed space. This capability is valuable for exploring posture-dependent lung function, which could serve as a marker for lung disease and be crucial to support stratified treatment approaches.
Methods
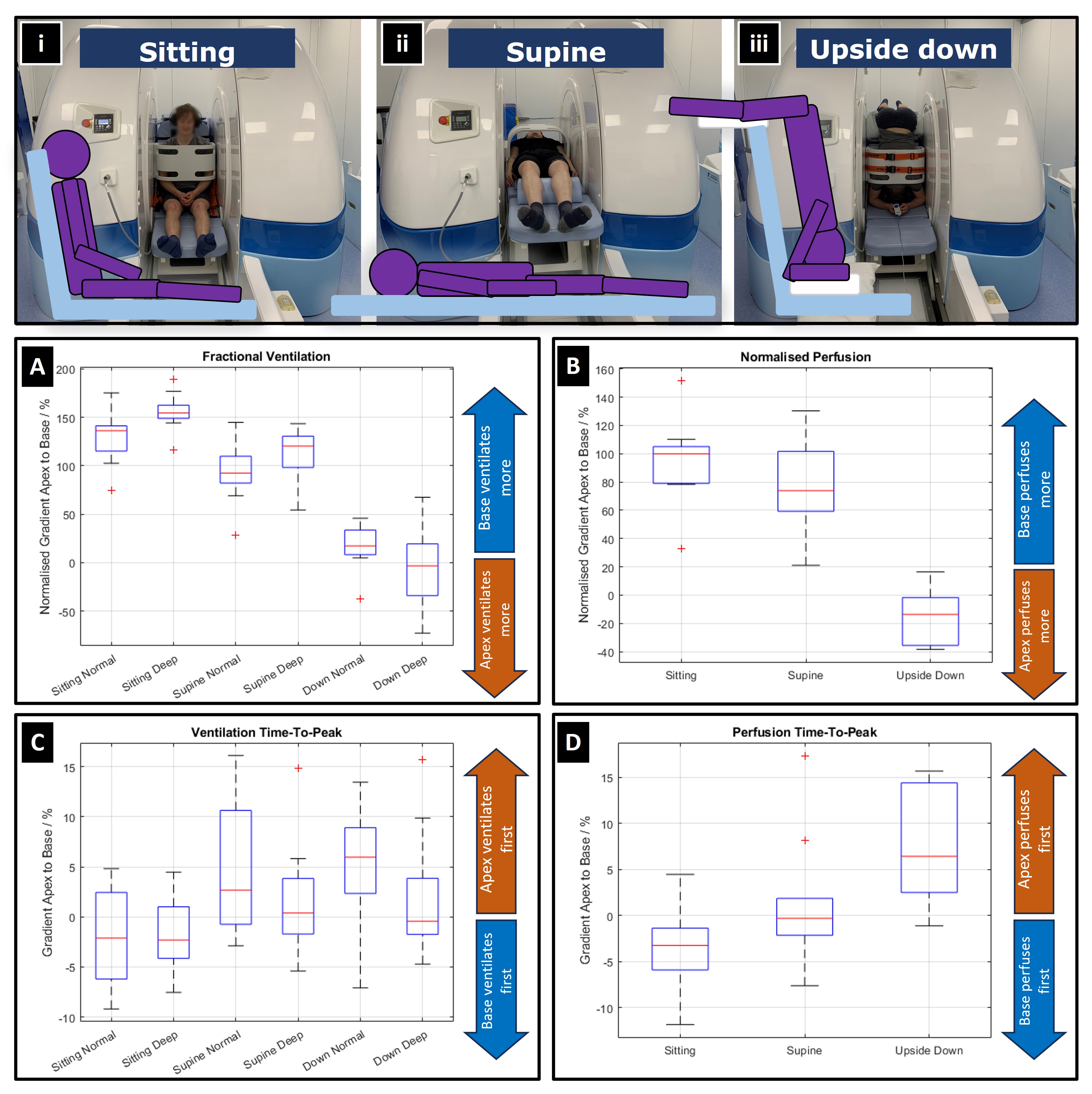
Ten healthy volunteers (average age 21±2yrs.) were recruited with ethics approval from the University of Nottingham Medical School Ethics Committee. Subjects were scanned in three postures: Supine, Sitting and Upside-Down (Figure1) whilst breathing normally and deeply. All experiments were carried out on a 0.5T Open MRI Scanner (Paramed, Italy) with a four channel receive body coil and a gradient system with a maximum power of 20mT/m and rise time 0.2ms. 200 dynamic images were captured at a rate of 2.6Hz using a 2D GRE protocol: TR/TE=5.7/1.2ms, FOV=32×32cm2, matrix size=89×89, slice thickness=10mm.PREFUL analysis was implemented in MATLAB-R2022b to reconstruct ventilation and perfusion maps. Ventilation and cardiac phase were determined for each frame using diaphragm position and aorta artery intensity respectively. Each image was registered to an intermediary inhalation position such that the lung parenchyma appears stationary throughout the time series. These images were used to reconstruct a single breath and single heartbeat consisting of 20 frames, interpolated onto an equidistant time series using a gaussian kernel (σ=0.05π). Changes in lung voxel intensity were used to attain local ventilation, perfusion, and respective time-to-peak information. Variation along the vertical axes was fitted via weighted linear model to attain the rate of change, apex to base.
Results
Fractional VentilationWhilst sitting, an increasing gradient of ventilation from the lung’s apex to base was apparent. This gradient increased when the subjects took deep breaths. A similar effect, albeit to a lesser magnitude was observed when supine. However, when positioned upside-down, the gradient decreased substantially to near zero and was further reduced when breathing deeply.
Ventilation Time-To-Peak
No discernible posture dependence of the Time-To-Peak ventilation.
Perfusion
When sitting, the base of the lung exhibited greater perfusion than the apex. This effect was persisted whilst supine, though to a lesser degree. When upside-down this effect reversed, albeit with a reduced magnitude compared to the other postures.
Perfusion Time-To-Peak
Whilst sitting, the base of the lung reached peak perfusion before the apex. Conversely, when upside-down the effect is reversed; the apex of the lung reaches peak perfusion before the base. When the subjects were supine, there was no significant variation in perfusion Time-To-Peak between the apex and base of the lung.
Discussion
The variation in fractional ventilation indicates that it depends both on gravity and physiological factors. If gravity were the sole mechanism, an inverse effect would be anticipated when participants were upside-down compared to seated. Instead, gravitational forces on inverted lungs appears to counter physiological effects to nullify most vertical variation. Furthermore, when the subjects were supine, the base of the lung continued to exhibit greater ventilation than the apex. As neither region experienced greater compressive forces than the other, this is likely attributed to physiology.The observed variation in perfusion mirrored that of ventilation. Greater magnitude at the base of the lung whilst supine suggests physiological contributions. When sitting or upside-down the effect was amplified or reversed respectively possibly due to the change in hydrodynamic pressure and tissue density. The lower magnitude observed whilst upside-down and positive effect whilst supine suggests sustained influence from physiological factors.
Perfusion Time-To-Peak variation indicates that the lung area situated lower, experiencing the greatest hydrodynamic pressure, achieves peak perfusion first. Thus, the base perfuses first when seated and the apex when inverted.
Conclusion
This work suggests that regional variation in lung function depends on both gravitational and physiological effects. The lungs appear to naturally ventilate and perfuse more at the base. This effect is amplified when upright and reduced (but not reversed) when upside-down. Additionally, whichever part of the lung is positioned lowest achieves its peak perfusion first.Acknowledgements
No acknowledgement found.References
[1] Glenny RW. Determinants of regional ventilation and blood flow in the lung. Intensive Care Med. 2009 Nov;35(11):1833-42. doi: 10.1007/s00134-009-1649-3. PMID: 19760203.
[2] Voskrebenzev A, Gutberlet M, Klimeš F, Kaireit TF, Schönfeld C, Rotärmel A, Wacker F, Vogel-Claussen J. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med. 2018 Apr;79(4):2306-2314. doi: 10.1002/mrm.26893. Epub 2017 Aug 30. PMID: 28856715.
Figures