0043
Deep Learning Reconstruction for Free-Breathing Radial Cine Imaging1Department of Electrical Engineering, Stanford University, Stanford, CA, United States, 2Korea Institute of Science and Technology, Seoul, Korea, Republic of, 3Department of Radiology, Northwestern University, Chicago, IL, United States, 4GE Healthcare, Stanford, CA, United States, 5Department of Radiology, Stanford University, Stanford, CA, United States, 6Stanford Cardiovascular Institute, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Image Reconstruction, Cardiovascular
Motivation: We aim to introduce a cardiac cine imaging protocol to address the issues of motion susceptibility and robustness in the previous techniques.
Goal(s): Our objective is to demonstrate an accelerated acquisition and high-quality reconstruction framework based on free-breathing radial cardiac cine imaging that shows enhanced patient comfort and robustness against respiratory motion.
Approach: We synergistically leverage a raw k-space preprocessing module, region optimized coil compression, and deep learning reconstruction based on memory efficient unrolled neural networks.
Results: Our experiments indicate that the proposed framework achieves high reconstruction quality at large acceleration factors (e.g., 8x), in terms of spatial and temporal accuracy.
Impact: Conventional cardiac protocols use Cartesian k-space sampling and are susceptible to motion artifacts. We provide an acquisition and reconstruction framework based on a free-breathing protocol and deep learning reconstruction for enhanced patient comfort and robustness against motion artifacts.
Introduction
Cardiac magnetic resonance imaging (CMR) is an essential modality for non-invasive assessment of cardiac morphology and function 1,2. Conventional balanced steady state cine CMR uses Cartesian k-space sampling, which is susceptible to motion artifacts and is less robust at higher heart rates 3,4. Thus, patients hold their breath during the acquisition to avoid blurring and aliasing resulting from respiratory movements. However, breath-holding can lead to patient discomfort, and is often infeasible in pediatric cases 5. Furthermore, breath-hold protocols limit scan durations and hence image quality and resolution. Therefore, it is of great interest to develop patient-friendly CMR techniques that are at the same time robust against respiratory motion effects 6.We propose a novel free-breathing approach for acquisition and reconstruction of accelerated radial balanced steady state cardiac cine imaging. The radial acquisition improves motion robustness by recurrently capturing central k-space and distributing motion effects across radial directions 7-9. Meanwhile, the free-breathing protocol aids patient compliance and comfort. For reconstruction, we synergistically leverage a k-space processing module and deep learning to mitigate the challenges of streak artifacts.
Methods
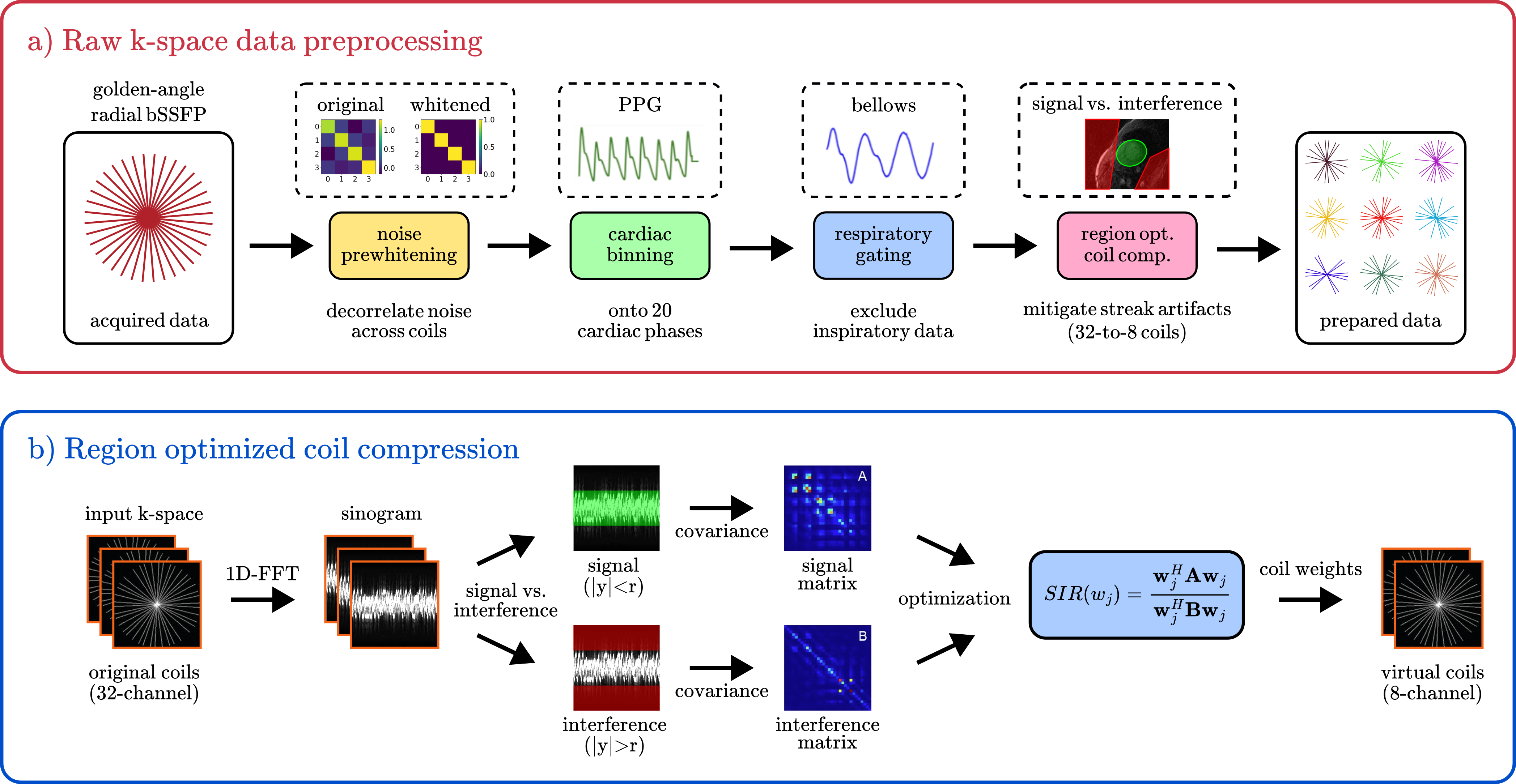
Raw k-space processing: Acquired raw k-space data are processed with 1) noise prewhitening to decorrelate noise across multi-coil k-space, 2) cardiac binning to synchronize acquisition with the cardiac cycle, 3) respiratory gating to exclude inspiratory data for mitigated motion, 4) region optimized coil compression to reduce streak artifacts originating from interference regions 10 (Fig. 1a).Region optimized coil compression: As opposed to traditional coil compression methods maintaining signal-to-noise ratio (SNR), we introduce region optimized coil compression (Fig. 2) to maximize signal-to-interference ratio (SIR). This technique computes 1D Fourier transforms of the radial k-space data to obtain sinograms, and then defines the region-of-interest as the center ($$$r<R$$$) and the interference region as the exterior, since streak artifacts are typically originating from signals in peripheral anatomic regions.
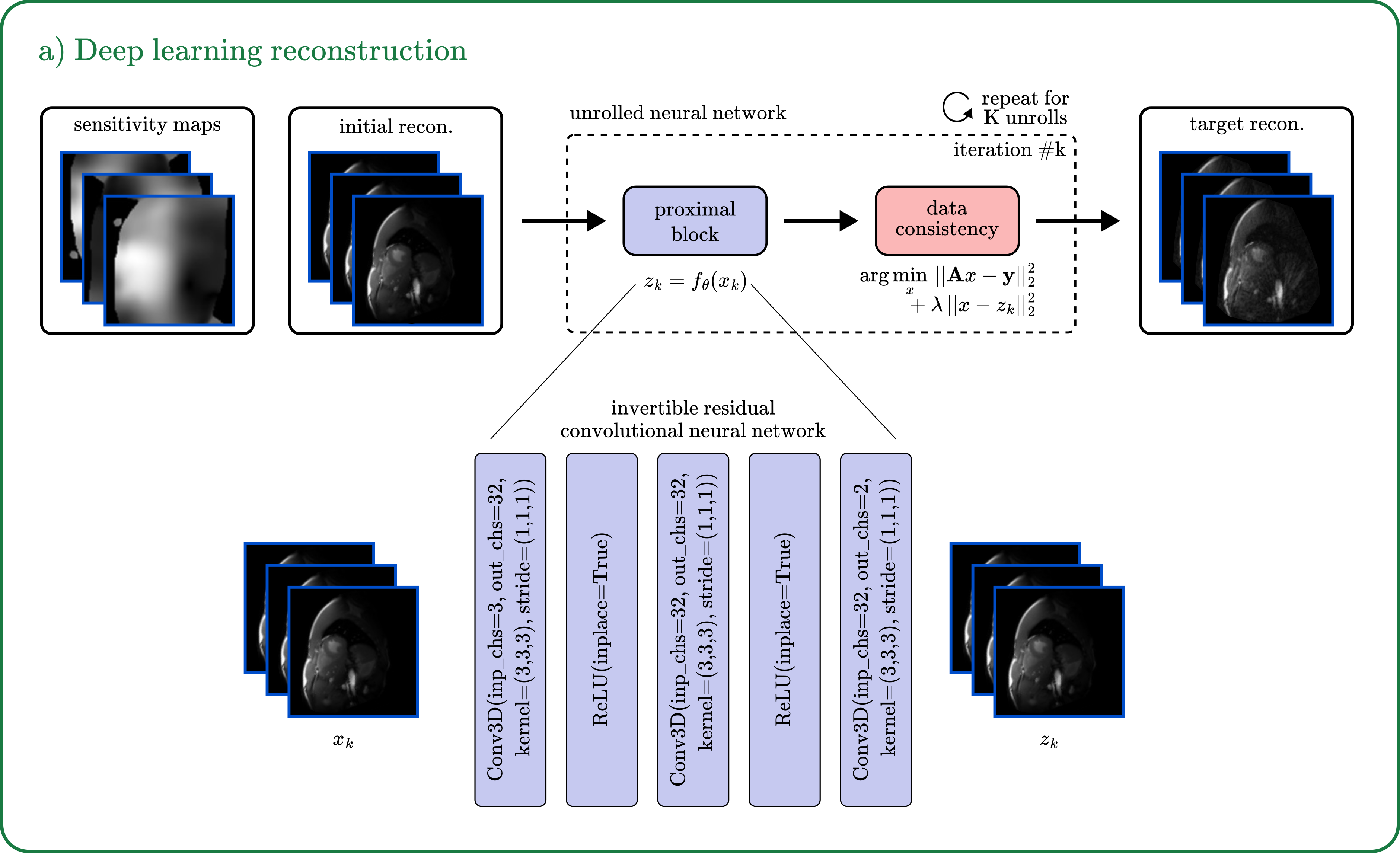
Deep learning reconstruction: An unrolled neural network is used with proximal block implemented via a 3-layer convolutional neural network, $$$z_n=CNN(x_n)$$$, and data consistency implemented via conjugate gradient, $$$\arg\min_{x}||Ax-y||_2^2+\lambda||x-z_n||_2^2$$$ (Fig. 2 for details). To address the large memory requirements of high-dimensional reconstruction, we employed memory efficient learning that only saves the intermediate inputs and outputs of each unrolled block, rather than the entire computational graph 11. Therefore, we opted for reversible residual learning in our network 12.
Data Acquisition
Free-breathing golden-angle radial cine short-axis stacks were collected from 11 volunteers with IRB approval and written informed consent, with 8 subjects for training, 1 for validation, and 2 for testing. From each subject, 11-15 short-axis slices were acquired with tiny golden angle using slice thickness = 6mm, bandwidth = 976.562 Hz/px, flip angle = 30°, TE/TR = 2.06/4.124 ms, number of phase encode = 320, field-of-view = 32cm, number of frequency encode = 512, and 70-80 seconds of data per slice. Four-chamber views were additionally acquired from 1 subject for testing. Respiratory bellows and photoplethysmography (PPG) signals were recorded for respiratory gating (to exclude inspiratory data) and cardiac binning (20 phases). For demonstrations, data were retrospectively undersampled by a factor of R=8x.Results
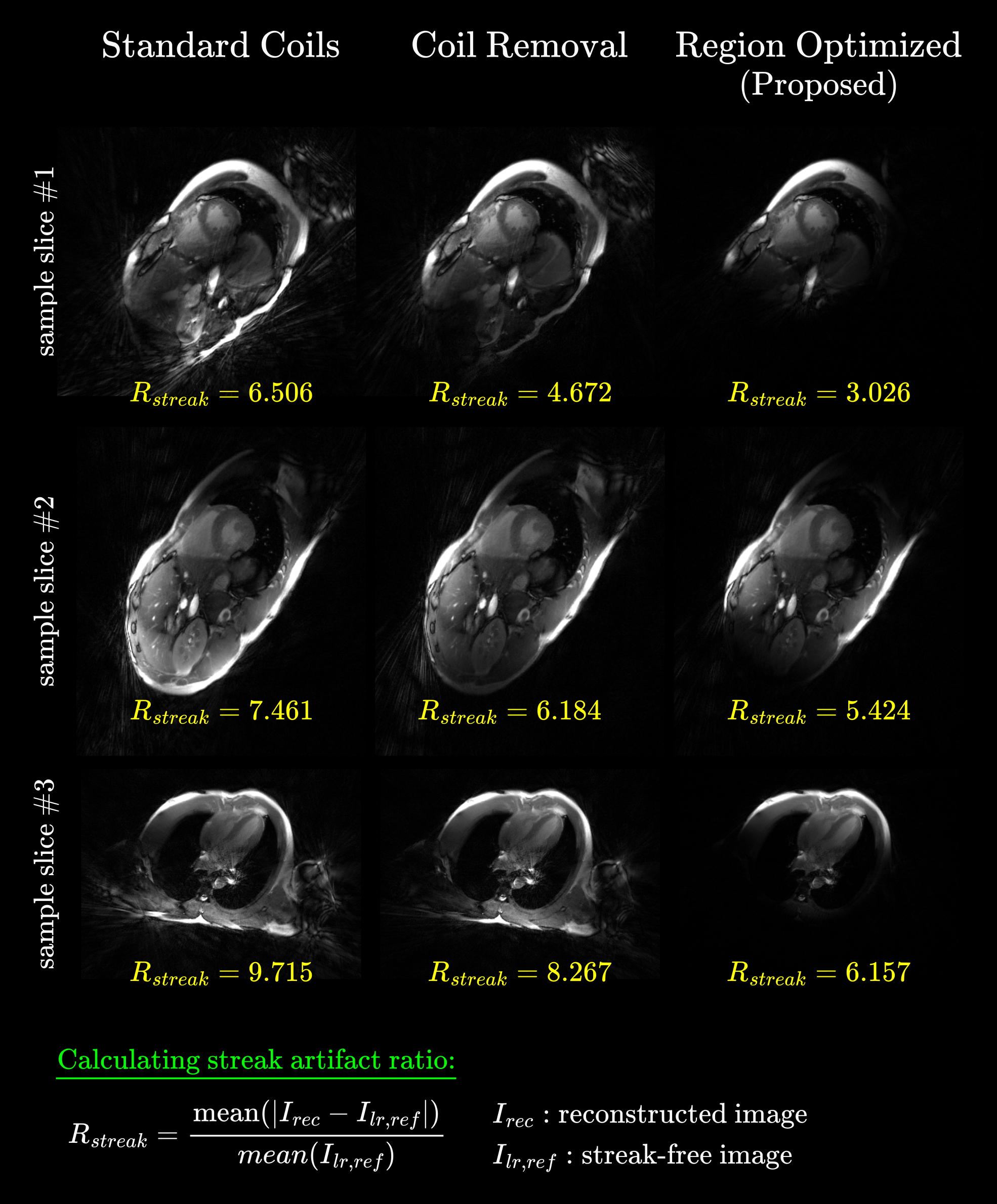
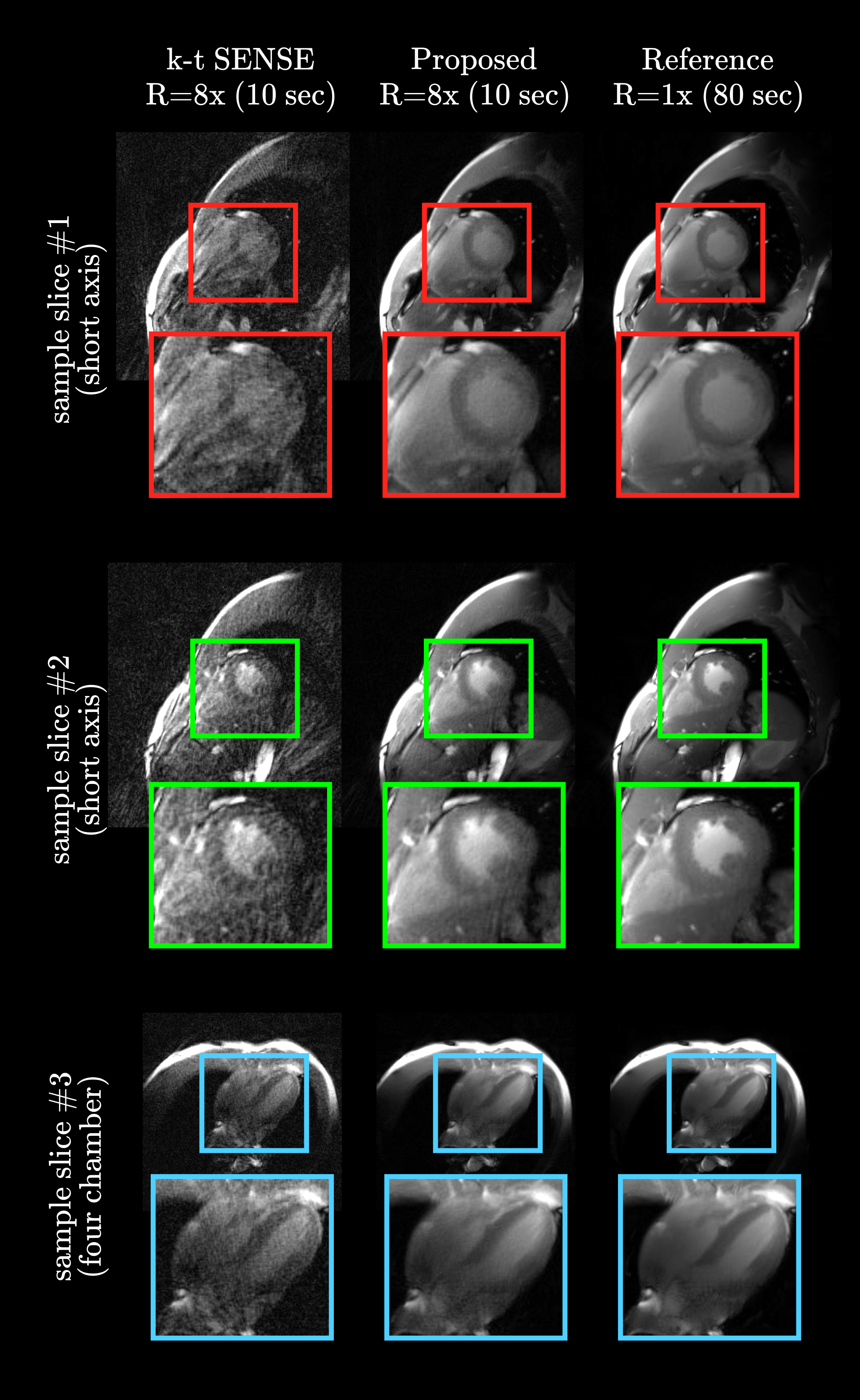
We first assessed the efficacy of the proposed coil compression. Fig. 3 displays coil combined images from standard coil compression (singular value decomposition), coil removal (automated subset selection 13), and the proposed region optimized compression (ROC). Representative slices from short-axis and four-chamber views indicate that ROC accurately removes signal from non-cardiac regions, mitigating streaking artifacts. Fig. 3, defines and displays streak artifact ratios for each slice, comparing coil compressed images from each method against streak-free low resolution images obtained from Hanning filtered k-space 14.Then, we performed experiments to demonstrate our deep learning (DL) reconstruction. Fig. 4 displays the reconstructed images at R=8x (10 sec acquisition per slice) via k-t SENSE and DL, together with reference fully-sampled images. DL yields high recovery quality on both short-axis and four-chamber views.
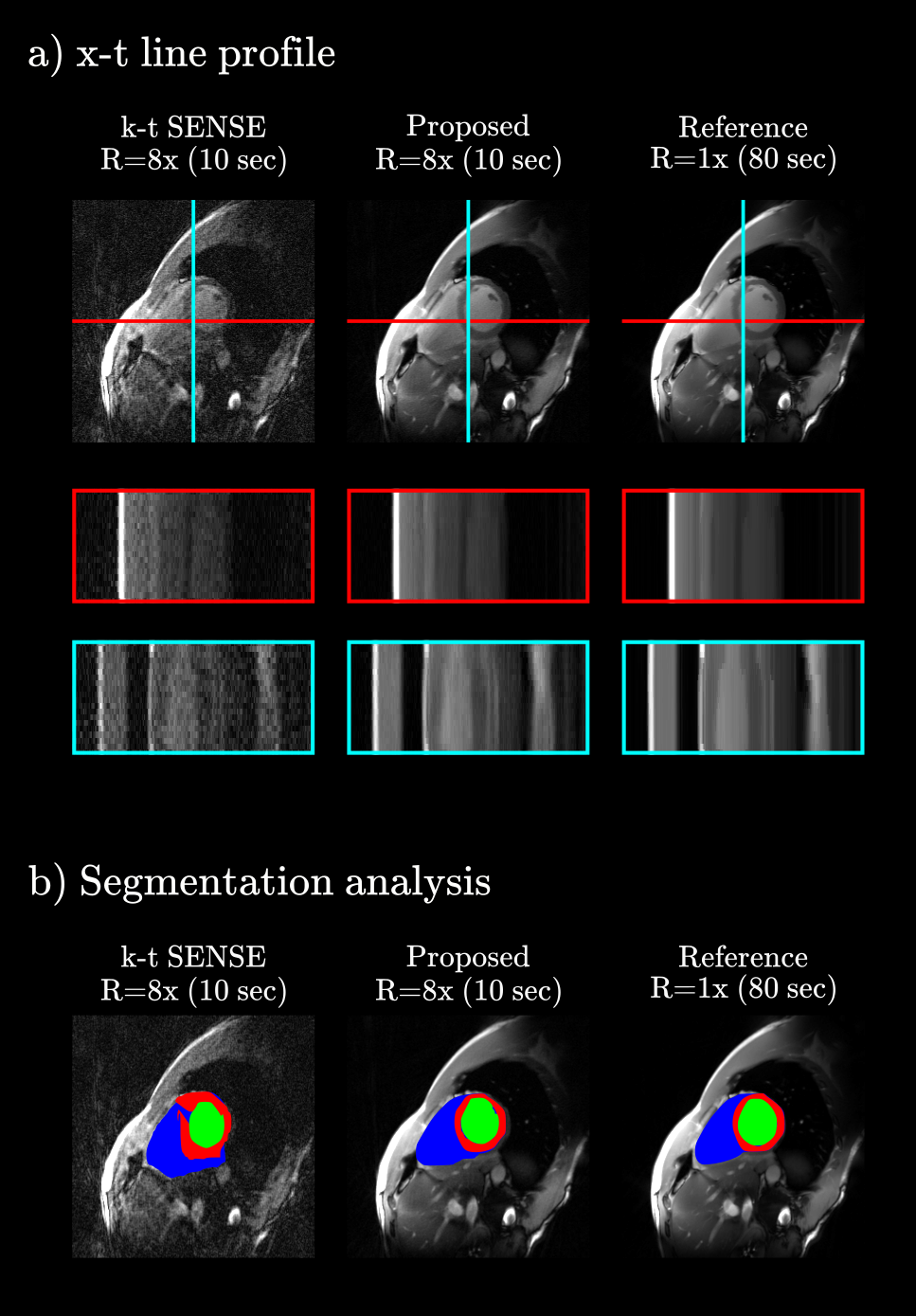
Fig. 5a show x-t line profiles, with DL yielding high recovery accuracy in the temporal dimension. Finally, we performed a downstream image analysis task based on segmentation via segment anything model 14. Results shown in Fig. 5b demonstrate that the recovery quality of the proposed method accurately translates to the segmentation task.
Discussion
We proposed an acquisition and reconstruction framework for free-breathing radial bSSFP cardiac cine imaging. Continuing work involves deep learning improvements to better capture information across temporal and spatial dimensions. Clinical studies with a large subject cohort are warranted.Acknowledgements
This work is partially supported by GE Healthcare, and in part by Stanford Cardiovascular Institute, and by NIH U01EB029427.References
[1] Ismail, T. F., Strugnell, W., Coletti, C., Božić-Iven, M., Weingaertner, S., Hammernik, K., ... & Kuestner, T. (2022). Cardiac MR: from theory to practice. Frontiers in cardiovascular medicine, 9, 826283.[2] McDonagh, T. A., Metra, M., Adamo, M., Gardner, R. S., Baumbach, A., Böhm, M., ... & Kathrine Skibelund, A. (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. European heart journal, 42(36), 3599-3726.
[3] Zaitsev, M., Maclaren, J., & Herbst, M. (2015). Motion artifacts in MRI: A complex problem with many partial solutions. Journal of Magnetic Resonance Imaging, 42(4), 887-901.
[4] Feng, L. (2022). Golden‐angle radial MRI: basics, advances, and applications. Journal of Magnetic Resonance Imaging, 56(1), 45-62.
[5] Vasanawala, S. S., Alley, M. T., Hargreaves, B. A., Barth, R. A., Pauly, J. M., & Lustig, M. (2010). Improved pediatric MR imaging with compressed sensing. Radiology, 256(2), 607-616.
[6] Oscanoa, J. A., Middione, M. J., Alkan, C., Yurt, M., Loecher, M., Vasanawala, S. S., & Ennis, D. B. (2023). Deep learning-based reconstruction for cardiac MRI: A Review. Bioengineering, 10(3), 334.
[7] Ryu, K., Sandino, C. M., Li, Z., Zhu, X., Coristine, A., Janich, M., & Vasanawala, S. S. (2021, May). Improving deep unrolled neural networks for radial cine cardiac image reconstruction using memory-efficient training, Conv-LSTM based network. In International Society for Magnetic Resonance in Medicine (ISMRM) 29th annual meeting (Vol. 19).
[8] Block, K. T., Uecker, M., & Frahm, J. (2007). Undersampled radial MRI with multiple coils. Iterative image reconstruction using a total variation constraint. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine, 57(6), 1086-1098.
[9] Feng, L., Grimm, R., Block, K. T., Chandarana, H., Kim, S., Xu, J., ... & Otazo, R. (2014). Golden‐angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden‐angle radial sampling for fast and flexible dynamic volumetric MRI. Magnetic resonance in medicine, 72(3), 707-717.
[10] Kim, D., Cauley, S. F., Nayak, K. S., Leahy, R. M., & Haldar, J. P. (2021). Region‐optimized virtual (ROVir) coils: Localization and/or suppression of spatial regions using sensor‐domain beamforming. Magnetic Resonance in Medicine, 86(1), 197-212.
[11] Wang, K., Kellman, M., Sandino C., Zhang K., Vasanawala S., Tamir J., Yu S., Lustig M., (2021). Memory-efficient learning for high-dimensional MRI reconstruction. MICCAI
[12] Gomez, A. N., Ren, M., Urtasun, R., & Grosse, R. B. (2017). The reversible residual network: Backpropagation without storing activations. Advances in neural information processing systems, 30.
[13] Xue, Y., Yu, J., Kang, H. S., Englander, S., Rosen, M. A., & Song, H. K. (2012). Automatic coil selection for streak artifact reduction in radial MRI. Magnetic resonance in medicine, 67(2), 470-476.
[14] Kirillov, A., Mintun, E., Ravi, N., Mao, H., Rolland, C., Gustafson, L., ... & Girshick, R. (2023). Segment anything. arXiv preprint arXiv:2304.02643.
Figures